
Abstract
Advances in glucose monitoring technologies have led to the development of different types of continuous glucose monitoring (CGM) platforms: traditional CGM and flash CGM. Both platforms provide critical glucose data that enable persons with diabetes (PwDs) to make more informed decisions in their self-management. Until recently, a key advantage of traditional CGM over flash CGM was the availability of automatic alarms that warn users about current or impending hypoglycemia and hyperglycemia. However, with the introduction of the FreeStyle Libre 2 (FSL2) system (Abbott Diabetes Care, Alameda, CA), PwD can now utilize flash CGM with the option to set low and high glycemic thresholds and receive alarms when these thresholds are crossed. In addition, having the option to use or not use the alarms may attract previous traditional CGM users who grew fatigued by constant alarms. However, despite the additional layer of safety that alarms provide, many PwD are reluctant to switch from self-monitoring of blood glucose to CGM due to concerns about how alarms could impact the quality of their daily lives. This reluctance is heightened by their perceptions that use of alarms is mandatory. Because the functionality of the FSL2 alarms differs from current traditional CGM devices, it is important that clinicians become familiar with these differences. Moreover, clinicians will be challenged to help PwD overcome their concerns about the use of alarms. This article presents a comprehensive description of the FSL2 alarms function and provides guidance to clinicians when counseling PwDs about the strengths, limitations, and various ways that the FSL2 alarms can be used in daily diabetes self-management.
Introduction
Currently there are two continuous glucose monitoring (CGM) technologies available: traditional CGM and flash CGM. The Dexcom G6 system (Dexcom, Inc., San Diego, CA) and Medtronic Guardian Connect system (Medtronic, Inc., Northridge, CA) are the most prominent traditional CGM systems that are commercially available. The FreeStyle Libre 2 (FSL2) system (Abbott Diabetes Care, Alemeda, CA) is the newest flash CGM system available today in the United States.
Large randomized controlled trials have demonstrated that use of both technologies improves glycemic control and use of flash CGM improves glycemic control, reduces hypoglycemia, and increases treatment satisfaction among individuals with type 1 diabetes (T1D) 1 –5 and type 2 diabetes (T2D) 5 –10 treated with intensive insulin therapy. Results from recently published prospective, observational studies have reported similar glycemic benefits while demonstrating the value of flash CGM use on reductions in diabetes-related events and hospitalizations among individuals with T1D 11 –17 and T2D treated with intensive insulin 18 or nonintensive therapies. 19
Although both types of systems provide the same glucose information, flash CGM users obtain their glucose data by scanning the glucose sensor with a handheld reader or smartphone, whereas glucose data are automatically transmitted to traditional CGM users. However, until recently, the major difference between the technologies was the availability of active alerts that warn users of immediate and impending hypoglycemia/hypoglycemia events. All traditional CGM devices currently include active alarms, whereas previous generations of the FreeStyle Libre systems did not offer this feature.
With the recent introduction of the FSL2 in 2020, persons with diabetes (PwDs) now have the ability to set low and high glycemic thresholds and receive real-time alarms when these thresholds are crossed. Due to the fact that the functionality of the FSL2 alarms differs from current traditional CGM devices, it is important that clinicians become familiar with these differences given the rapid adoption of the FSL2 by individuals with T1D and T2D. 20 However, because some PwD may be resistant to using CGM due to perceptions of how alarms may disrupt their daily lives, clinicians must also develop strategies for helping PwDs overcome their resistance and, thus, benefit from the improved glycemic control offered by CGM.
This article presents a comprehensive description of how the FSL2 alerts function and provides guidance to clinicians when counseling PwDs about the strengths, limitations, and various ways the alerts can be used in daily diabetes self-management.
FSL2 CGM System with Optional Alerts
Overview
The FSL2 CGM system utilizes two components: a disposable sensor and a separate handheld touchscreen reader device. The sensor, which is inserted into the user's upper arm, continuously samples and measures interstitial glucose levels, generating a new glucose value each minute. Each FSL2 sensor can be worn for up to 14 days, thereby facilitating the ability to obtain enough glucose readings to ensure reliable data. 21 Users scan the sensor with the device reader to obtain their glucose data.
The glucose data are presented in both numerical and graphical formats, which include the current glucose level, trend arrows that indicate the velocity and direction of changing glucose, and a trend graph that shows the most recent 8 h of glucose data. The touchscreen also presents relevant messages (e.g., glucose going low) and the ability to add notes to the current glucose reading.
The user scans the sensor with the reader to transfer data and view real-time glucose information on the reader. As each scan provides the last 8 h of data, users should be instructed to scan at least every 8 h to avoid gaps in the data. In addition, all CGM systems have a warm-up period before glucose values are available. The FSL2 and Dexcom G6 sensors have a warm-up period of 1 and 2 h, respectively. Therefore, PwDs should be encouraged to scan frequently to ensure full data capture, optimize use of their device, and to wait until after the warm-up period before using their glucose data for therapy decision making.
A new feature of the FSL2 system is the LibreLinkUp, a free mobile app that enables patients to send glucose readings to family and friends. The app is compatible with Android phones running Android OS 6.0 and higher and iPhones running iOS 11 and higher. The LibreLinkUp app is currently available in Canada, Europe and the US.
Why optional alarms are important
An important feature of the FSL2 is that users now have the option to turn off their alarms according to their individual needs and preference. If users have their alarms turned ON, the FSL2 automatically alerts them when glucose levels have crossed the glycemic thresholds set by the user and if the signal between the sensor and reader is lost. In these situations, users are alerted on the reader through sound or vibration.
Although alarms can be important in reducing the incidence and severity of acute glycemic events by warning users of current and impending hypoglycemia and hyperglycemia when they are not frequently reviewing their glucose data, 22 –24 they can also become a source of annoyance and disrupt daily life. 25 Importantly, CGM users who experience frequent alarms often become overwhelmed and fatigued with the constant interruptions caused by frequent alarms, 25,26 and many users eventually fail to respond to them. 27
Because greater treatment satisfaction has been shown to be strongly associated with improved adherence and persistence with prescribed treatment regimens, 28,29 it is important that individuals with diabetes have the flexibility and freedom to manage their diabetes in ways that accommodate their individual preferences and lifestyles. By offering the option to turn off alarms, the FSL2 has the potential to reduce “alarm fatigue” among users who find alarms troublesome and inconvenient and thus improve treatment satisfaction and adherence.
In addition to alarm fatigue, there is also the issue with “alarm embarrassment”; what does one do in the middle of an important meeting? Adolescents are particularly concerned about this issue and often will not wear a CGM with too many alarms due to worry about the alarm going off in school and causing them to be the focus of attention.
Setting up optional alarms
The optional alarms are triggered without scanning the sensor. When any of the alarmed events occur, the system will display the event on the reader screen and alert the user through sound or vibration, according to the user's preference. Once alerted, the user will need to scan the sensor to obtain the glucose level corresponding to the alarm. The automatic alarms allow users to take appropriate action as needed to address the immediate issue, and they provide guidance when it comes to decisions related to medication or diet. Figure 1 presents the alarm messages displayed in the reader.
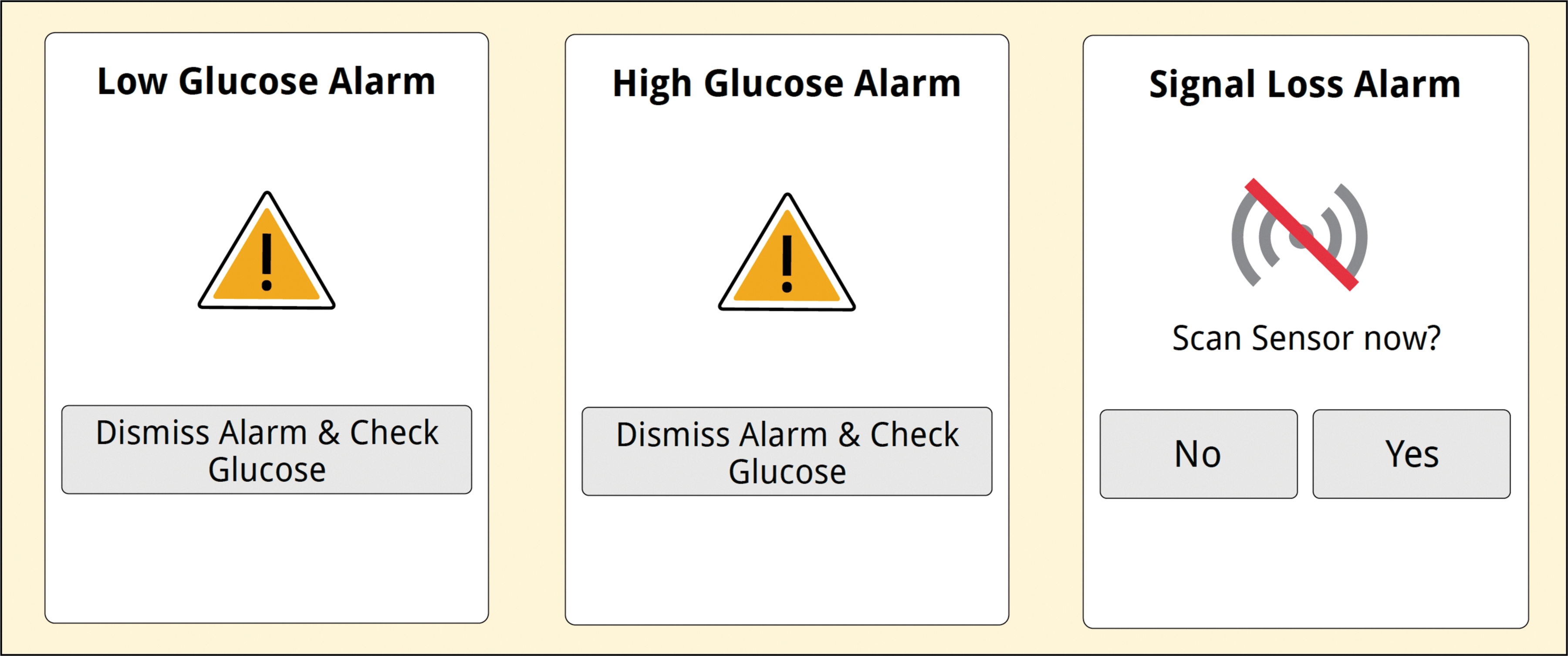
Alarms for low glucose, high glucose, and signal loss.
To receive an alarm, the alarms must be turned on and the reader should be always within 20 feet of the user. In the United States, the alarms are preset to the ON position. It is important that users make sure that the reader always is sufficiently charged and that the sound and/or vibration is turned on. Users who do not want the alarms can choose to leave them turned off to avoid being disrupted by unwanted alarms. Figure 2 explains how to set the alarms.
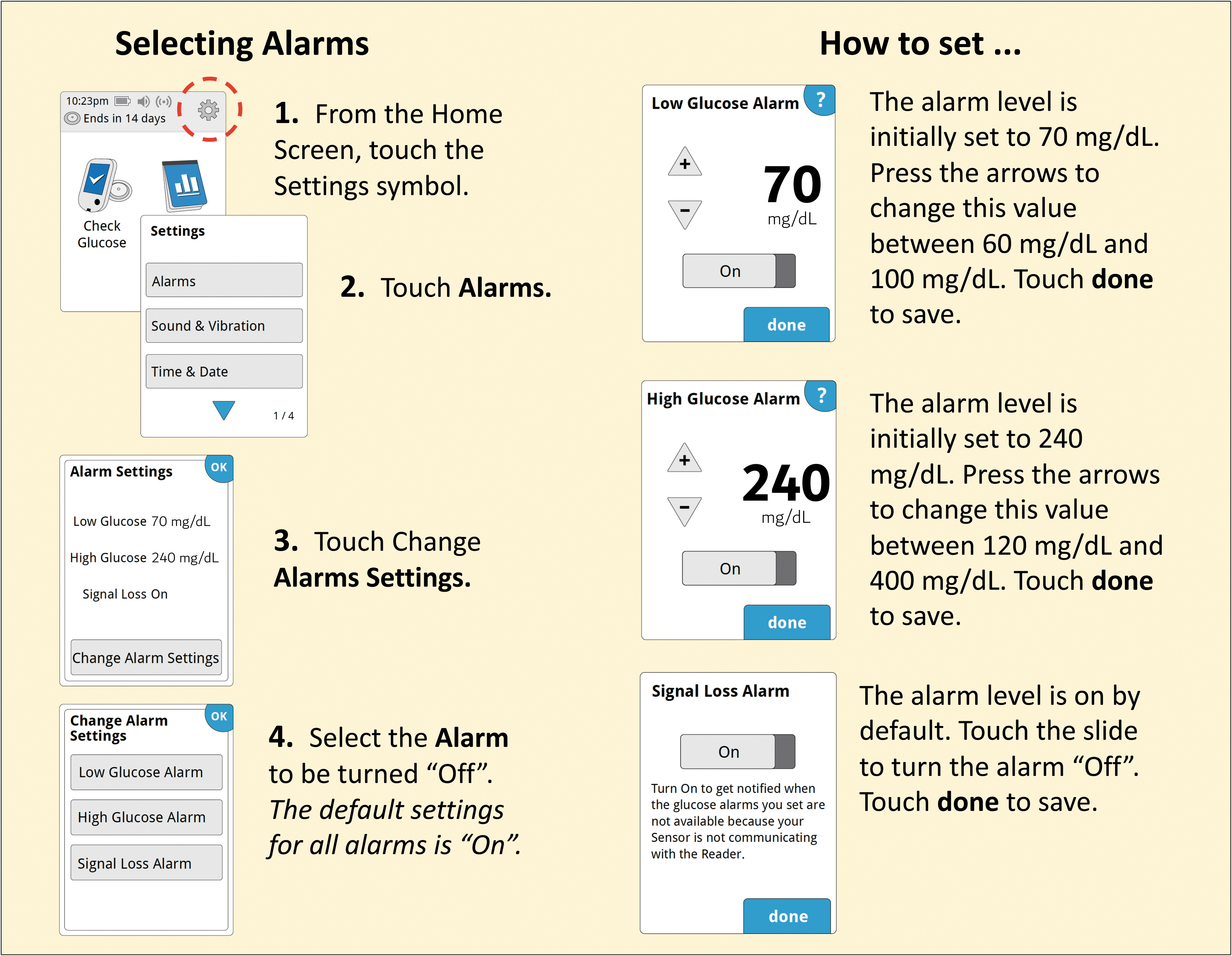
Setting the optional alarms.
Counseling PwD About Use of Optional Alarms
Where the science and the PwD intersect
Current clinical guidelines based on scientific evidence recommend CGM use in individuals with T1D and T2D treated with intensive insulin therapy. 30 –32 A growing body of evidence also supports the use of CGM in individuals with problematic hypoglycemia (e.g., severe and/or frequent, hypoglycemia unawareness) regardless of their therapy. 19,33 –36 Given that the majority of studies demonstrating the clinical benefits of CGM involved devices that feature alarms and alerts, it makes good “clinical” sense to strongly encourage patients to immediately start using their alarms when they initiate their FSL2 regimen. But, does this make practical sense?
We do not believe so. In fact, it can often be counter-productive. Although many individuals who choose to use the FSL2 device do so because it now offers alarms, those PwD who are reluctant (or adamantly opposed) to even trying CGM due to concerns about how the alarms will affect the quality of their lives may perceive this approach as an “all or none” proposition: CGM with alarms or no CGM.
When we talk about person-centered care, we often conflate this with whether the PwD can afford the prescribed treatment or has an adequate support system. Often, the individual's preferences and concerns receive little or no attention. Moreover, when presenting the various diabetes tools and technologies, there is a tendency for clinicians to recommend the devices that we prefer because of the features that are of the greatest convenience to us (e.g., specific data download interfaces or device features). Then, we spend our time trying to convince our patients that our preferred device is the “best” device for them.
A more practical approach
In our view, person-centered care means meeting each PwD where they are in their diabetes journey and understanding that their preferences and concerns are based on their current treatment regimen. For PwD who are resistant to alarms, the key is to “ease into” using the alarm features. We have developed a five-step approach that may help clinicians make this transition with their PwD (Table 1).
Five-Step Approach to Transitioning Patients to Continuous Glucose Monitoring
CGM, continuous glucose monitoring.
Step 1: Uncover the obstacles and concerns relevant to everyone's current diabetes self-management regimen. Do they feel safe? Discouraged? Powerless? Do they know what their glucose testing numbers mean and/or what to do with them? What has worked for them in the past? What hasn't?
Step 2: Ask the PwD to discuss how changes in their current regimen would satisfy their preferences and address their fears and concerns. How would fewer fingerstick tests improve their quality of life? How could seeing where their glucose is heading and how fast it is changing affect their sense of safety and confidence in their therapy decision making? Answers to these questions provide insights that can guide clinicians in presenting CGM as an option to traditional blood glucose testing.
Step 3: Present the relevant benefits of CGM. Although PwD should be made aware of the long-term clinical consequences of uncontrolled diabetes, clinicians should avoid using “scare tactics,” which is ineffective and often backfires, causing the PwD to shut down or give up trying to manage their diabetes. 37 A more effective approach is to focus on how CGM directly addresses the preferences and concerns identified by the PwD.
Step 4: Ask how the patient believes CGM would work for them in their daily lives. Although the temptation is to focus on convincing the PwD to use the alarms, this may not be appropriate in many cases. Some PwD may need to learn to appreciate how using the alarms can reduce their fears and improve the quality of their lives. Having the option to turn off their alarms, initially, allows PwD to develop this appreciation in their own time without feeling pressured. In addition, it may be the first time that a PwD is “wearing” anything on their person. So, it is important that they first get comfortable with simply wearing the device and then slowly increasing the interaction with the device. It is also important to reassure PwD that it is okay not to use the alarms if this is an issue. Instead, we should recommend that they scan their sensor frequently during the first few days and nights to see when they tend to go high or low. If they find they are frequently going low, advise them to review their download reports to determine when this is occurring, how low their glucose is dropping, and then reflect on why they think this is occurring. What were the potential causes? What could they have done to prevent the lows? Then, the PwD can make a choice. Do they want to use this information to pay more attention to their glucose during these periods through more frequent scanning? Or do they want to try using the optional alarms, which would provide an early warning of impending low glucose without the burden of additional scanning.
Step 5: If the PwD chooses to use the alarms, the final step is counsel them on how to effectively utilize this option in ways that meet their individual needs. This involves confirming when problematic glycemic events are occurring, adjusting the glucose thresholds to effectively respond to these events, and counseling the PwD to make sure the alarms are set for the appropriate times.
Conclusions
Numerous studies have demonstrated the clinical benefits of earlier generation FreeStyle Libre CGM systems in individuals with T1D 1,2,11,12,38,39 and T2D. 6,7,12,18,19,38 –41 With the introduction of the FSL2 system, PwD can now benefit from an additional level of safety and improved glycemic control with the availability of optional alarms. This feature has the potential to improve adherence with CGM use, particularly in patients who find CGM systems with compulsory alarms troublesome. However, changing PwD perceptions of how use of CGM would impact the quality of their lives will require clinicians to take a true person-centered approach that focuses first and foremost on the individual needs and concerns of each PwD.
Footnotes
Acknowledgments
The authors wish to thank Christopher G. Parkin, MS, CGParkin Communications, Inc., for editorial support.
Author Disclosure Statement
E.M. has received consulting fees from Abbott, Astra Zeneca, Novo Nordisk Boehringer Ingelheim, Eli Lilly, Merck, Sanofi U.S., and has acted as a speaker for Abbott, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk. L.K.M. has served on scientific advisory boards for Abbott Diabetes Care, and his institution has received research support from Abbott Diabetes Care.
Funding Information
Funding for the development of this article was provided by Abbott Diabetes Care.