
Abstract
Background:
Development of coordinated management approaches is important to facilitate self-care in people with diabetes (PwD). Gaining a better understanding of suboptimal insulin use is key in this endeavor. This review aimed, for the first time, to systematically identify and narratively summarize real-world evidence on the extent of suboptimal insulin use (missed and mistimed insulin) in PwD.
Methods:
A systematic literature search of MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews identified studies reporting on missed and mistimed insulin dosing.
Results:
From 3305 studies, 37 publications reporting on 30 unique studies that involved 58,617 PwD were included. Studies were conducted across 12 different countries and most employed cross-sectional surveys. Observations regarding missed and mistimed insulin doses were reported in 25 and 10 studies, respectively. PwD reported missing insulin doses, but rates varied due to differences in reporting methods, participant populations, and insulin regimens. The association between missed dosing and glycemic control was evaluated in ten studies in which the authors reported lower glycated hemoglobin (HbA1c) levels in PwD who did not omit insulin. The proportion of PwD reporting mistiming of insulin was in the range of 20–45%, depending on the study; this was associated with higher rates of hypoglycemia and higher HbA1c as reported by study authors. Reasons for suboptimal insulin use were multifactorial, occurring due to disrupted daily routines, social situations, and hypoglycemia avoidance.
Conclusions:
This review suggests that suboptimal insulin use is widespread and that PwD using insulin may still be struggling with disease management. There is an unmet need for better integrated support in managing the complexities of insulin therapy and for the development of systems (e.g. digital solutions) that empower people to take control of insulin-treated diabetes.
Introduction
Over the past several decades, the management of diabetes has seen significant improvements through advances in drug development and device technology. Yet despite all the innovations, diabetes remains a significant human and economic burden. 1 In general, levels of glycemic control do not appear to have improved in recent years or have even deteriorated. 2 –4 Furthermore, evidence suggests that many insulin-treated people with diabetes (PwD) are still failing to reach glycemic targets. 5 –9 This trend of inadequate glycemic control is already having a detrimental impact, with national statistics and epidemiological studies demonstrating that rates of diabetes-related complications have increased in recent years. 10
Failure to achieve glycemic control at a population level has been linked with the inherent complexities of medication taking. 11 With respect to insulin treatment, it is important that PwD do not miss doses, take insulin at suitable times, and take the appropriate dose accounting for glucose measurements, carbohydrate intake, and physical activity. Successful disease management is, therefore, highly challenging for insulin-treated individuals (who must engage in multiple time-consuming and complex behaviors while trying to live as normal a life as possible) and for their physicians. 12 Unsurprisingly, inadequate management of prescribed insulin regimens has been widely reported. 13 –15
Understanding the extent, impact, and possible causes of suboptimal insulin use is key for the development of coordinated management approaches that integrate the benefits of monitoring, education, and clinical support to facilitate self-care among PwD. The current systematic literature review was therefore undertaken to identify and narratively summarize evidence on the extent of suboptimal insulin use with respect to missed and mistimed doses in PwD in real-world practice.
Materials and Methods
The systematic literature search was conducted according to a reproducible protocol that described the proposed approach, objectives, search strategy, study selection criteria, methods for data extraction and synthesis, and outcomes of interest that were specified a priori. This article is a review and analysis of previously published studies and does not include any new studies on human or animal subjects performed by any of the authors, therefore ethics approval was not required
Search strategy
Journal articles published in English between January 2005 and February 2020 were identified from searches of MEDLINE, EMBASE, and the Cochrane Database of Systematic Reviews. To capture recent relevant studies that might not yet be published, abstract books were electronically searched on EMBASE from relevant congresses held during 2019 as follows: all congresses of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR), the European Association for the Study of Diabetes (EASD), and the American Diabetes Association (ADA). In addition, the abstract book from the Advanced Technologies and Treatments for Diabetes Conference (ATTD), which was not indexed on EMBASE, was hand-searched for relevant studies. A hand-search of the reference lists of eligible studies identified in the main review was also conducted.
A search strategy was developed for each database to understand suboptimal insulin use in PwD (search strings for each database are provided in the Supplementary Tables S1–S3. The main search strategy consisted of three concepts: diabetes mellitus, insulin, and suboptimal dosing outcomes. Terms for nonspecific “insulin” and insulin brand names were those as provided at:
A gray search of the literature was undertaken based on the authors' own knowledge of the field and review of company websites based on known congress presentations.
Inclusion criteria
Study inclusion and exclusion criteria as related to patient population, interventions, outcomes, and study type are given in Table 1.
Study Eligibility Criteria
Exclusion criteria further refined based on cluster of studies found with these comorbid conditions that was deemed out of scope based on the study aim and eligibility.
Clinical outcomes were only reported if included in studies that reported suboptimal insulin dosing behavior.
Mistimed doses defined as insulin doses not taken at the specified times and so includes delayed administration (e.g., postprandial) and irregular dose timing.
DM, diabetes mellitus; EHR, electronic health record; PwD, people with diabetes; RCT, randomized controlled trial.
Article selection
Results obtained using the search strategy were assessed independently by two reviewers using a two-phase approach. Initial screening involved a broad review of titles and/or abstract of results to identify studies meeting or possibly meeting eligibility criteria. Studies identified as being potentially eligible were subject to in-depth full-text review. Articles excluded at this stage were assigned an exclusion code and reported in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. Any discrepancies between reviewers were discussed until consensus was reached or by involving a third reviewer.
Data extraction and reporting
Data were extracted from the included full-text articles. The following fields were included country of conduct, study objective, design, setting, and duration, methods of data collection, insulin dosing behavior captured, and patient population (number, diabetes type, age, and gender). A data extraction table was populated by one team member and quality checked by a second. Synthesis of findings was narrative.
Results
Study selection
In total, the literature research resulted in the selection of 37 full journal publications describing 30 unique studies. Four different studies yielded 11 separate publications: the first Global Attitudes of Patients and Physicians in Insulin Therapy Survey (GAPP1) contributed data to three separate publications 16 –18 ; the GAPP2 survey contributed data to four publications 19 –22 ; a U.S. cross-sectional survey (using Harris Interactive Chronic Illness Panel) regarding the burden of insulin therapy contributed data to two publications 23,24 ; and a Swedish qualitative study contributed data to two publications. 25,26 No relevant congress abstracts were identified. The study selection process is shown in the PRISMA flow diagram (Fig. 1).
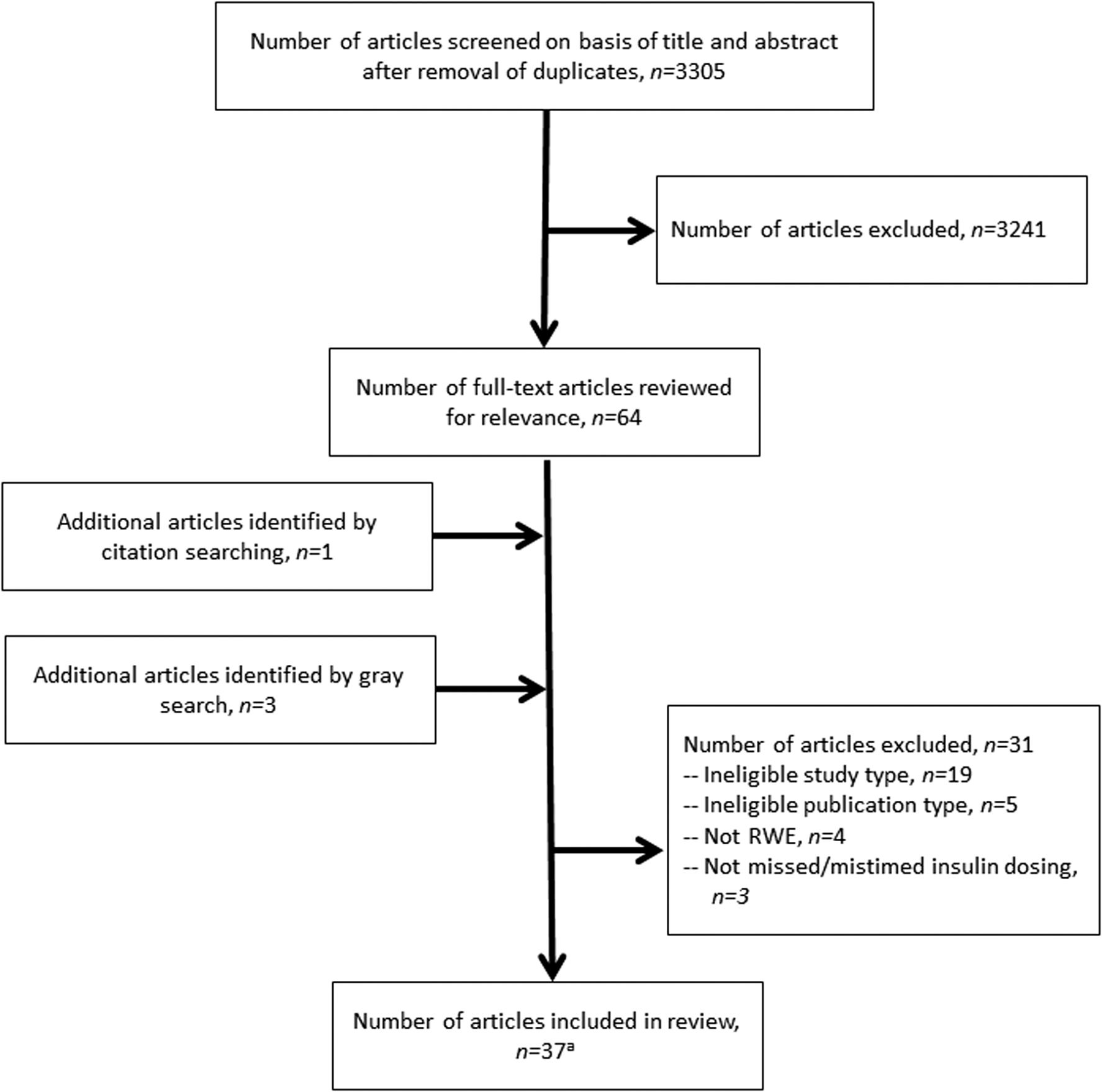
PRISMA flow diagram. aArticles describe data from 30 unique studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RWE, real-world evidence.
Study characteristics
Detailed study characteristics are given in Supplementary Table S4 in the Supplementary Data. Included articles were published between 2005 and 2019. Studies were conducted in 12 different countries, with the United States being the most represented (n = 15 studies); four studies were multinational, and one was conducted in Canada and the United States. Most studies employed cross-sectional surveys that were administered in a variety of ways including online, face-to-face, or through telephone interview. Each survey was administered at a point in time and requested information regarding insulin dosing irregularities over a specified retrospective period, which generally varied from 1 week to 3 months across studies. A total of 58,617 PwD were included in the 30 unique studies. People with type 1 diabetes (T1D) were included in 17 unique studies (n = 48,554) and those with type 2 diabetes (T2D) in five unique studies (n = 6333). A mixed population of T1D and T2D were included in eight unique studies (n = 3730) and health care professional responses regarding the insulin dosing behaviors of their PwD were solicited in three studies that involved 2473 health care professionals (HCPs) in total. Observations regarding missed insulin doses were reported in 25 studies (32 publications) and on mistimed insulin doses in 10 studies (14 publications). Missed or mistimed dosing was reported with bolus insulin in 11 studies, basal insulin in 3 studies, and both basal and bolus insulin in 3 studies. Nearly half of the included publications did not specify insulin when reporting on suboptimal insulin dosing behaviors.
Missed insulin doses
Studies in T1D
Evidence for missed insulin dosing was reported in 16 studies in people with T1D. All studies identified reported various degrees of missed dose behavior, with rates varying considerably on account of differences in reporting methodologies and time ranges, patient population. For example, in one study it was reported that 56.2% of adults missed at least one bolus insulin dose in the last month, 27 another demonstrated that 21.4% missed at least one dose (insulin type not specified) in the last week, 28 and a third study reported that 12% missed at least one bolus dose per day. 29 Key findings from studies in T1D are given in Table 2. Some studies in T1D involved adolescents (13 to <18 years) or emerging adults (18 to <26 years), and these demonstrated that there were differences in the frequency of missed insulin doses according to age (Table 2). Adolescents/emerging adults were more likely to miss bolus doses compared with younger children and compared with older individuals (≥45 years). 29,33 Insulin dose omission was also commonly reported among children and adolescents with T1D who were using continuous subcutaneous insulin infusions (CSII), with frequent missing of bolus insulin at mealtimes and when snacking (Table 2). 37 –39
Key Findings From Studies Reporting Missed Insulin Doses
Same patient cohort as Rubin et al. 23 but additional data reported in the publication.
Appears to be same patient cohort as Peyrot et al. 16 but some differences in the data reported.
CGM, continuous glucose monitoring; CSII, continuous subcutaneous insulin infusion; GAPP, Global Attitudes of Patients and Physicians in Insulin Therapy for Diabetes Mellitus; HCP, health care professional; PwD, people with diabetes; T1D, type 1 diabetes; T2D, type 2 diabetes.
Studies in T2D
Four studies (n = 7 publications) reported missed insulin dosing among people with T2D, with much of the data deriving from the GAPP2 study) (Table 2). For example, missing at least one dose of basal insulin in the previous 30 days was reported in 16%, 22%, and 23% of the United Kingdom, global, and Canadian GAPP2 cohorts, respectively, 20 –22 although this was reported in only 1% of the Spanish cohort possibly because of a shorter disease duration at baseline in these individuals compared with other countries. 19 Most PwD participating in the GAPP2 study missed insulin doses unintentionally (Table 2). 19 –21 Similar rates of insulin omission were reported in the other included studies. 40,41 A single study compared insulin regimens and found that more PwD on a basal-bolus insulin missed insulin doses compared with those on premix or basal insulin (61.3% vs. 22.7% and 15.9%, respectively). 41
Studies in types 1 and 2 diabetes
Five studies (n = 8 publications) that described results from a mixed population of PwD also indicated that insulin omission occurred in a substantial proportion of participants (Table 2). For example, in the GAPP1 survey 44% and 33.2% of PwD in the Japanese and multinational cohorts, respectively, omitted insulin or did not take insulin as prescribed over the previous month. 16,18 Physicians included in GAPP1 and in another U.S. survey indicated that a high proportion of PwD missed insulin doses or failed to take insulin as prescribed (Table 2). 16,18,23 Omission of insulin was reported to occur both intentionally and unintentionally in studies of mixed diabetes populations, 44 with forgetfulness emerging as a key theme in a qualitative analysis. 42
Association between missed doses and clinical outcomes
Eleven studies (n = 13 publications) reported on the association between missed insulin doses and clinical outcomes; key findings are given in Table 3. Missed insulin doses were consistently reported to be associated with higher HbA1c levels in people with T1D. 27,29,33,37,38,45,46 Similarly, in the GAPP2 study in people with T2D, HCPs indicated that missed insulin doses were associated with negative clinical effects, reporting that ∼3 to 4 missed basal insulin doses per month significantly impacted glycemic control. 19 –21 Although data are more limited, it was suggested by two studies that missed insulin doses may be negatively associated with health-related quality of life (QoL) in adolescents with T1D 37 and adults with T2D. 40
Key Findings on the Impact of Missed Insulin Doses on Clinical Outcomes
BG, blood glucose; DTR-QOL, diabetes therapy-related quality of life; HbA1c, glycated hemoglobin; HCP, health care professional; HRQoL, health-related quality of life; MMAS-8, 8-item Morisky Medication Adherence Scale; PwD, people with diabetes.
Mistimed doses
Key findings from the 10 studies that reported mistiming of insulin doses are described in Table 4. Three studies evaluated the delayed administration of bolus insulin specifically and demonstrated that ∼25% to 30% of PwD (T1D or T2D) administer insulin boluses during or after meals contrary to guideline recommendations. 48,49,51 In the GAPP2 study, mistiming of basal insulin in people with T2D was defined as administration ±2 h from the prescribed time. The rate of basal dose mistiming ranged from 20% to 26% in the previous 30 days across the United Kingdom, global, and Canadian cohorts. 20 –22 Similar rates of mistimed basal doses (>2 h outside agreed dose time) were reported among people with T1D in a Japanese study although rates were somewhat higher in people with T2D (Table 4). 50 Although rates of mistimed insulin dosing were not specifically reported in the GAPP1 study, both PwD and physicians indicated that dose timing was a key difficulty with respect to insulin self-management (Table 4). 16,18
Key Findings From Studies Reporting Mistiming of Insulin Doses
HCP, health care professional; PwD, people with diabetes.
Association between mistimed doses and clinical outcomes
Five studies (n = 7 publications) also provided some insights regarding the association of mistimed dosing with clinical outcomes (Table 5). For example, rates of hypoglycemia were higher among PwD who dosed bolus insulin postprandially compared with those who dosed during or premeal. 48,49,51 In addition, glycemic control was reported to be better among PwD who dosed bolus insulin regularly and administered their dose premeal. 46,49 Findings from the GAPP2 study also demonstrated the importance of dosing insulin at the correct time with respect to clinical outcomes, HCPs estimated that 5.7–6.2 mistimed basal doses were associated with a significant impact on glycemic control over the previous 30 days (Table 5). 19 –21
Key Findings on the Impact of Mistimed Insulin Doses on Clinical Outcomes
HbA1c, glycated hemoglobin; HCP, health care professional; MMAS-8, 8-item Morisky Medication Adherence Scale; PwD, people with diabetes.
Reasons for suboptimal insulin use
Of the included studies, 14 (n = 19 publications) reported on reasons for missed and mistimed insulin doses (Table 6). Reasons were multifactorial and commonly included forgetfulness, 16,18,25,27,41,42 disruption to usual routines including traveling, 16,18,41 or that insulin interfered with the performance of usual daily activities. 16,17,24,44 PwD also reported missing or mistiming doses to avoid hypoglycemia or because their usual eating patterns had been disrupted. 17,19 –21,27,41 Participants in the GAPP1 survey noted that regimen complexity was one of the reasons for insulin omission/nonadherence and that it was challenging to take insulin at the same time each day. 16,18 Other factors commonly associated with suboptimal insulin use were being embarrassed or uncomfortable administering doses in public or social situations or that injections were too painful. 16,18,20,21,24,44 Two studies suggested that some PwD missed doses because they were feeling better and they considered injections unnecessary. 41,43 There was also evidence that diabetes-related distress, stress, and depression may increase suboptimal behaviors (Table 6). 28,31,36
Key Findings From Studies Reporting Reasons for Suboptimal Insulin Use
Same patient cohort as Rubin et al. 23 but additional data reported in the publication.
Appears to be same patient cohort as Peyrot et al. 16 but some differences in the data reported.
PHQ, Patient Health Questionnaire; PwD, people with diabetes.
Discussion
This review identified and described 30 unique studies that reported on missed and mistimed insulin dosing in people with T1D or T2D. Findings from the studies described herein indicate that these suboptimal insulin dosing behaviors are not uncommon and suggest that despite advances in insulin therapy over the past several decades, PwD continue to struggle with the complexities of insulin self-management. It is likely that the prevalence of missed and mistimed insulin dosing is even higher than that reported in the included studies. Surveys often found discrepancies between the observations of HCPs and that of their PwDs, with higher rates of missed or mistimed doses being reported by HCPs. 16,22 Indeed, HCPs surveyed in the GAPP2 study believed that ∼30% of PwD underreport the number of basal insulin doses that they miss. 22 That PwD are often reluctant to discuss self-care with their physician and frequently misrepresent or withhold important information on diet, exercise, blood glucose monitoring, and medication taking is well known. 53 Possible reasons for such reluctance may include fear of being judged, because they do not want to disappoint or “annoy” their physician, or because they do not understand medical recommendations. 53
The studies identified herein suggest that suboptimal insulin use may be associated with some PwD not achieving glycemic targets. Several analyses reported that insulin dose omission or mistiming of doses were associated with higher levels of HbA1c. 27,29,33,37,38,40,45,46,49,52 PwD appear to be aware of the detrimental impact of suboptimal dosing; 65% of European GAPP2 participants recognized that missing basal insulin doses would negatively affect their health. 19 Furthermore, a substantial proportion of PwD indicated that they felt worried or guilty about missing doses. 19,20,22 HCPs also clearly recognize the issues, with participants in GAPP2 estimating that 3.6–4.3 missed and 5.7–6.2 mistimed basal insulin doses in the previous month might have a negative effect on glycemic control. 19 –21 Given that the potential adverse consequences of missing or mistiming insulin are well understood, why are such behaviors so prevalent?
Several of the included studies reported on the reasons for suboptimal insulin use. Various factors were identified as being associated with missed or mistimed doses and were both unintentional (forgetting for various reasons) and intentional (deliberately not taking insulin as directed). Forgetfulness can be caused by disruptions in daily routines and interference by social situations. 16,18,27,41,42 Insulin use requires countless decisions each day regarding lifestyle behaviors and medication, and these complexities of self-management can represent a significant barrier to consistency of dosing. For example, in the GAPP1 study, major difficulties associated with insulin management identified by PwD and physicians included having to take insulin at the same time each day, adjusting insulin doses, changing the timing of insulin dosing to meet daily needs, and following HCP instructions. 16 As such, PwD perceive that insulin treatment interferes significantly with their ability to perform activities of daily living 24 and feel that treatment regimens prevent them from living a normal life. 16 It must also be acknowledged that there may also be occasions when a deviation from the specified dosing is fully justifiable and clinically appropriate (e.g., in the setting of low blood glucose levels). Under these circumstances, for example, a dose should not be considered missed or mistimed. However, the current studies did not specifically report on this issue.
Another reason consistently shown to be associated with suboptimal insulin use is fear of hypoglycemia. 54 People with T1D and T2D report omitting insulin doses to reduce the risk of hypoglycemia, because their eating patterns are “not as usual,” or because they skipped a meal. 19 –21,27,41 There is also evidence that given the relentlessness of diabetes self-management and the associated burden of insulin regimens, many PwD experience diabetes-related distress and diabetes burnout wherein they may disengage from self-care tasks. 55 For example, Hessler et al. 31 found that diabetes-related distress was significantly associated with the frequency of missed bolus insulin doses. PwD sometimes describe feeling “defeated” by the challenges of disease self-management and anxious about failing to complete self-care tasks adequately. 56 Studies in this review suggest that feeling overwhelmed by diabetes management may be associated with insulin omission/nonadherence. For example, in their cross-sectional study, Olamoyegun et al. 44 reported that being “tired of injections” was one of the seven major reasons for insulin omission; and in a qualitative analysis, Brod et al. 42 identified that PwD with a history of forgetting to dose insulin frequently felt tired and complacent with respect to disease management.
Despite acknowledging the clinical relevance of suboptimal insulin dosing, 32% and 29% of HCPs in the GAPP2 study did not routinely discuss these behaviors with their PwDs on basal insulin or basal-bolus insulin regimens, respectively. 20 HCPs often indicate that there is a lack of time to support or fully understand the concerns of their PwDs and to take an individually tailored approach to treatment. 57 Indeed, even in the best-case scenarios, the number of clinic visits per year is insufficient for the majority of PwD. 58 Furthermore, ready access to accurate and reliable clinical data can be lacking for HCPs because PwD-recorded information through more traditional methods is sometimes incomplete or incorrect, 59,60 and there can be difficulties in sharing such information in a timely manner with the health care team.
A PwD-centered approach to enhance engagement with diabetes self-care is an important theme in clinical practice recommendations. 61,62 Empowering PwD to gain control over decisions affecting their health by providing them with the means to easily organize and execute the courses of action required for disease management is key for successful self-care.
Clearly, there is a need for innovative approaches to disease management that help both PwD and physicians optimize the use of insulin therapy and fine-tune dosing such that target HbA1c and glucose time-in-range metrics can be achieved. 63,64 In the management of diabetes, it is important to move away from historical data review and response to an ever-changing clinical situation and move toward dynamic, (near) real-time behavioral changes. Digital health tools, such as continuous glucose monitoring, mobile applications, smart insulin pens, and connection-enabled pen caps/clips and their connection into integrated platforms, are just one of several solutions now being used in clinical practice to facilitate better management. 58
Approaches to diabetes management that potentially place control back in the hands of the PwD through close self-monitoring and provision of real-time observations could improve their ability to fine-tune insulin dosing and so avoid detrimental short- and long-term consequences. The PwD-HCP relationship is acknowledged to be a key contributor to treatment success and effective communication at key points in the disease journey can improve the QoL of PwD and clinical outcomes. 65 –68 This relationship and communication between HCP and physician may perhaps be enhanced if based on the objective data that could be provided by digital health tools. 69
The current review was conducted according to a reproducible search protocol that reduced the impact of review author bias to ensure transparency and accountability and maximize the changes of accurate data extraction. However, the search was largely pragmatic, and it is possible that other studies of relevance may have been published. Furthermore, the search was restricted to articles in the English language; other relevant studies could have been published in other languages. Search results were reviewed according to a two-stage approach wherein the decision to include/exclude a publication was initially based on review of the title and abstract. As such, it is possible that potentially relevant studies could have been excluded at this stage because of lack of detail in the title/abstract. Inconsistencies in the description of real-world evidence in the literature and the range of terminologies used for this across studies also made the decision to include challenging in some cases. Finally, although the cut-off date of the current search was February 2020, the field is continually evolving, with new studies published all the time. Studies published since our cut-off data include one that reported racial/ethnic differences in insulin dosing behaviors in emerging adults 70 and another that demonstrated missed insulin doses in 27% of people with T1D during COVID-19 lockdown who also experienced an increase in HbA1c levels compared with pre-lockdown. 71
Several limitations were also observed with respect to the evidence base. Cross-study comparisons are hindered by differences in the designs, reporting methodologies, and populations. For example, similar questions were phrased inconsistently across surveys, making it difficult to be certain that the behavior described in one was comparable with another. In addition, studies reported rates of insulin omission or mistiming in various ways. In surveys, participants were often recruited from preexisting research panels, and therefore might not be representative of the general diabetes population. Some questionnaires could have been administered online at a time when Internet access was not as widely available, perhaps leading to an over-representation of younger patients. It is also likely that any reported insulin dosing irregularities are underestimated, because surveys were mostly self-completed, which could potentially lead to incorrect classifications. Furthermore, recall and social bias could have led to underestimations of suboptimal insulin use, given that this may be perceived as potentially inappropriate medication-taking behavior. Because underreporting is highly likely across studies, the finding that reported behaviors were as widespread and prevalent as they were, is a cause for concern. It should also be noted that study designs did not allow causation to be inferred with respect to the impact of missed or mistimed dosing on clinical outcomes or with respect to the reasons for suboptimal dosing. Furthermore, the reasons for missing or mistiming doses may differ depending on how PwD administer their insulin (e.g., by insulin pump), but the included studies do not provide any further insight regarding this.
Finally, this search was originally undertaken based on a broader protocol that included the following additional concepts of interest: incorrect doses, over- and underdosing, and miscalculated doses (data on which can also be captured by digital health technology). Limited data were identified on these aspects of suboptimal insulin use, and the precise nature of the dosing errors was not always captured in detail. As such, the authors have made the decision not to report these in the current review and instead have added them as exclusions in the PRISMA diagram.
Conclusions
This systematic literature review demonstrated that suboptimal insulin use, including missed and mistimed doses, is widespread among people with T1D and T2D and that these behaviors may be negatively associated with clinical outcomes. These observations suggest that some individuals are continuing to struggle with the complexities of diabetes management and the specific challenges of insulin therapy. Approaches that facilitate better disease management are clearly needed, particularly those that empower and enable PwD and that improve the PwD-HCP relationship and communication through provision of objective data. Digital health tools may represent one such solution. Although their usefulness is still under investigation, it will be interesting to see what role these new technologies will play in the future of diabetes care.
Footnotes
Authors' Contributions
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work, and have given their approval for this version to be published.
Acknowledgments
The authors thank Mick Arber (York Health Economic Consortium [YHEC]) for assistance with the literature search and Alison Terry of KMHO Ltd. for assistance with editing the article.
Author Disclosure Statement
S.R. and T.K.-M. received funding from Lilly to conduct the study. B.L. and R.S.N. are employees of Eli Lilly and Company. T.B. reports grants from NIH-NIDDK, grants from EU-EC-IMI, grants and personal fees from Novo Nordisk, personal fees from Eli Lilly, grants and personal fees from Sanofi, personal fees from AstraZeneca, grants and personal fees from Medtronic, grants and personal fees from Abbott, personal fees from Roche, grants from Zealand, personal fees from Indigo Diabetes, and personal fees and other from DreaMed Diabetes, outside the submitted work. T.B. was funded in part by the National Institutes of Health—NIDDK grant no. UC4DK108611, by the European Commission/IMI INNODIA Grant No. 664535, by the Slovenian National Research Agency Grants No. J3–6798, V3–1505 and P3–0343, and by the University Medical Centre Ljubljana Research and Development Grant no. 20110359.
Funding Information
The study was funded by Eli Lilly and Company (Indianapolis, IN).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.