
Abstract
Telemedicine is a promising strategy that utilizes telecommunication to provide health care in remote areas, facilitating beneficial interaction between the health care provider and people in rural areas and making affordable and accessible medical care available to remote, inaccessible areas of the world. This article provides an overview of some of the ways telemedicine is improving diabetes care outcomes at the community level. Telemedicine can play a number of roles in moving quality diabetes care forward. It is currently being used to create awareness among urban and rural population about the risk factors and prevention of diabetes; to facilitate patient monitoring; for remote diabetic retinopathy screening; and in diabetes prevention at the primary, secondary, and tertiary level. We also highlight the use of automated artificial intelligence software combined with telemedicine to conduct efficient real-time screening of complications such as diabetic retinopathy in remote areas where such facilities are currently unavailable.
Introduction
The global prevalence of diabetes continues to increase with an estimated 425 million people currently affected, and this number is estimated to escalate to 629 million by the year 2045. 1 Over 90% of all affected individuals have type 2 diabetes. Four out of five people with diabetes live in low- and middle-income countries (LMIC), approximately half of whom remain undiagnosed according to the International Diabetes Federation. 1
India ranks second after China in the global diabetes epidemic and is expected to surpass China in the next few years. 1 India also has a large rural population (>70%) and the prevalence of diabetes in rural areas is rising rapidly. Tackling rural diabetes has its own challenges, including poverty, illiteracy, lack of accessibility, and nonavailability of essential drugs and specialized care. 2,3 Moreover, the ratio of undiagnosed to diagnosed diabetes is higher. 4
The increasing prevalence of diabetes in low-income countries is of great concern because of high morbidity and mortality and the costs associated with the treatment of complications of diabetes. 5 Among individuals with self-reported diabetes in rural areas of India, for example, good glycemic control, defined as glycated hemoglobin (HbA1c) <7%, was observed in only 30.8% of the 15.4% of people who reported having checked their HbA1c during the past year. 6 Thus, in rural areas, diabetes remains a neglected disorder. 7
Models of care that are tailored to resource-constrained countries are needed, especially in remote rural areas, to provide better access to screening for diabetes and its associated complications as well as offer better management. Several technology-based approaches to reach out to remote and underserved communities and monitor their health at their door step are now being explored.
Recent advances in information technology and widespread availability of the mobile phone present unique opportunities for prevention, control, and management of chronic diseases like diabetes. 8 These approaches include telemedicine, mobile technology, and use of the internet. However, there is need for developing comprehensive interventions and integrating available technologies to be able to provide comprehensive care for diabetes. This article provides an overview of the role of telemedicine technologies in improving diabetes care and how we have used it in India.
Telemedicine and Diabetes Care
Telemedicine is increasingly being utilized in the field of diabetology to improve access to health care, quality of care, and clinical/psychosocial outcomes in people with diabetes. As many aspects of our lives have become automated and addressed online, so will routine medical care of chronic diseases. 9
Mobile health refers to the use of mobile communication technologies to promote health by supporting health data collection, delivery of health care information, and/or patient observation, provision of care, 10 and disease prevention. 11 Although access to this technology has rapidly expanded in developing countries, 12 its potential benefits in improving health care are still underutilized. Mobile phone messaging applications, including text messaging or short message service (SMS) and multimedia message service, could offer a convenient and cost-effective way to support desirable health behaviors for preventive health care by providing educational and motivational advice. 12 Several studies have assessed the feasibility of mobile technology to prevent and manage type 2 diabetes. 13 –18
Role of telemedicine in creating awareness
A large-scale, community-based diabetes awareness and prevention program, prevention awareness counseling, and evaluation (PACE) was initiated to improve awareness about diabetes. 14 PACE included four components: (1) a free public awareness campaign with lectures and interactive programs; (2) 164 “PACE Education Counters” opened at various bookshops, shopping complexes, food chain stores, and family physician clinics in Chennai (southeastern India), which provided free diabetes educational materials; (3) mass media programs, including a documentary film/radio program on diabetes and diabetes prevention and management messages provided through newspaper articles, cinema theater advertisements, and text messaging on mobile phones; and (4) training for general practitioners in diabetes management and prevention strategies.
Through the PACE diabetes project, a total of 774 screening and education camps were conducted all over Chennai and 76,645 individuals were screened for diabetes. Among those screened, 17% had known diabetes, 4% had newly diagnosed diabetes, and 7.5% had prediabetes. In addition, 150,000 SMS messages were sent to subscribers on prevention of diabetes to general population and management of diabetes throughout the state of Tamil Nadu (southern tip of India). Assessments conducted after the PACE project (in 2007) showed improvements in diabetes awareness and knowledge compared with results of the earlier CURES survey conducted in 2001–2002. 19 This project is an example of how telemedicine can increase awareness of diabetes. 14,19
Further evidence of telemedicine efficacy comes from a prospective, parallel-group, randomized controlled trial involving Asian Indian men with impaired glucose tolerance. Conducted at 10 sites, the study assessed whether mobile phone messaging that encouraged lifestyle change could reduce incident type 2 diabetes. 18 This study reported that the cumulative incidence of type 2 diabetes was lower in the intervention group who received mobile phone messages (18%) than in controls (27%). Investigators concluded that mobile phone messaging is an effective and acceptable method to deliver advice and support toward lifestyle modification to prevent type 2 diabetes, in men at high risk.
Role of telemedicine in self-monitoring of blood glucose
The increased burden of diabetes has prompted increasing efforts to develop mobile technologies for monitoring of blood glucose among individuals with diabetes. During the past decade, much progress has been made in utilizing technology to monitor blood glucose levels. Glycemic control in individuals with diabetes can be measured by various means, including laboratory-based glucose monitoring, HbA1c, self-monitoring of blood glucose (SMBG), and continuous glucose monitoring system, using ambulatory glucose profiles for data interpretation and analysis.
SMBG is a valuable tool for decision-making for both patients and clinicians. 20 Regular SMBG has been shown to improve HbA1c and reduce the fear of both hyperglycemia and hypoglycemia in individuals with type 1 and type 2 diabetes. 21,22 A wide range of blood glucose meters are available that are portable, inexpensive, accurate, and reliable. One of the barriers to frequent and regular SMBG is patients' inability to make decisions based on the results. However, this issue could be addressed by the use of telemedicine technology. The increasing use of smartphones and availability of mobile applications for management of diabetes present a possible method to transmit the SMBG test results to a health care provider electronically through emails, SMS, or Internet portal.
The Structured Testing Program (STeP) study evaluated how a structured patient/physician SMBG intervention influenced the timing, frequency, and effectiveness of primary care physicians' treatment changes among 483 poorly controlled, insulin-naive type 2 diabetes patients over a year. 23 On assessing the impact of structured SMBG on physician treatment modification recommendations (TMRs), it was reported that patients who received at least one TMR demonstrated a greater reduction in HbA1c (−1.2%) than the active control group (−0.8%). The STeP study investigators concluded that a collaborative use of structured SMBG data leads to earlier, more frequent, and more effective TMRs.
Quinn et al. 24,25 have studied mobile-based health applications and improvements in glycemic control. A study conducted in 2008, 24 among 28 patients with type 2 diabetes, showed that the intervention group, which received cell phone-based software, achieved statistically significant improvements in HbA1c compared to the patients in the control group. Another study conducted by the same group reported that, including mobile application coaching and patient/provider web portals to community primary care reduced HbA1c levels in patients with type 2 diabetes compared with those on standard diabetes management. 25
In the recent 6-month, prospective, multicenter, single-arm study by Mora et al., 26 participants used a novel SMBG system (Accu-Chek® Connect diabetes management system; Roche Diabetes Care, Indianapolis, IN) that automatically transmits blood glucose data from the meter to a smartphone app and then to secure personal and health care professional portals. 26 The health care portal automatically organizes the glucose data, identifying patients who are at risk for acute glycemic events, which enables clinicians to triage patients according to the greatest need. Results from the study showed a strong association between use of the system and improved glycemic control, increased patient satisfaction, and reduced distress among individuals with insulin-treated diabetes.
Thus, utilizing mobile technology to review blood glucose data could provide an opportunity to reduce glycemic variability and complications associated with diabetes. 27 Moreover, new technologies are being explored, which eliminate the need for a blood glucose meter, allowing patients to use their smartphone and test strips to obtain a test result and then provide their result through a variety of digital modes to their clinician.
Real-time telemedicine
Real-time telemedicine is a promising strategy for improving access to care and care delivery in image-oriented fields like ophthalmology and radiology, where diagnostic decisions are often based on review of photographs/images that are captured by trained technicians. 28
India is home to over 72 million people with diabetes, 1 all of whom require annual retinal examination for early detection of diabetic retinopathy. However, access to screening is significantly limited. In India, the ophthalmologist-patient ratio in urban India is 1:25,000, but in rural India, it is ∼1:250,000. 29 Reports have shown that 35%–80% of people with diabetes do not follow the eye care recommendations. 30
Diabetic retinopathy produces no visual or ocular symptoms until the advanced stages of retinopathy are reached. The value of screening is well established, as early detection of diabetic retinopathy helps in timely treatment with modalities that can decrease the risk of severe visual impairment. 31
Inadequate number of trained optometrists/retina specialists and the high cost of the conventional fundus cameras are major challenges to providing regular screening of the large number of people with diabetes in India. 32 The inequitable distribution of ophthalmologists/eye hospitals across the country further widens the gap between demand and availability of eye care to people with diabetes in rural areas and places a major burden on the health care system of India. Studies have shown that digital retinal color photography (either mydriatic or nonmydriatic) is a practical alternative for regular screening of people with diabetes for retinopathy. 33,34
Teleophthalmology is, thus, a promising solution for enabling secure transmission of information and transfer of digital retinal images for diagnosis and decision-making by an ophthalmologist or retinal specialist and timely referral for treatment of diabetic retinopathy when indicated (e.g., laser photocoagulation and intravitreal injections). 35,36
Guidelines and model for diabetic retinopathy telemedicine program
The American Telemedicine Association and Diabetic Retinopathy Telehealth Practice Recommendations Working Group 37 have provided guidelines and recommended that the equipment used for diabetic retinopathy telescreening must conform to the requisites of the local and federal bodies, which specify that the diagnostic accuracy of the fundus camera used for retinal imaging must be validated and the telemedicine technology must adhere to the standards of Digital Imaging and Communication in Medicine. 38
The four main components of diabetic retinopathy telemedicine screening are as follows: (1) retina image acquisition—at least one posterior pole image of each eye; (2) image review and evaluation by a trained retina specialist/grader; (3) supervision of patient care; and (4) data and retinal image storage and most importantly, timely referral to a retinal specialist when further treatment for diabetic retinopathy is indicated. 36
Digital retinal fundus photography imaging in teleophthalmology
Conventional stereoscopic fundus cameras remain the gold standard for retinal examinations. However, these cameras are expensive. Recently, digital retinal color photography with smaller cost-effective fundus cameras has been validated for diabetic retinopathy screening. A few examples include the Visuscout handheld camera and Remidio fundus on phone (FOP) camera, which is a smartphone-based imaging device. 39
The FOP camera provides good quality high-resolution retinal images and has been successfully used in teleophthalmology screening. 39 These sleek devices are easy to handle and require minimal training for technicians. They have helped reduce the economic burden on the health care system related to screening for diabetic retinopathy. Imaging through teleophthalmology services helps to detect not only diabetic retinopathy but also other important diabetic eye disorders like cataract, glaucoma, and age-related macular degeneration.
Teleophthalmology screening services are offered at Dr. Mohan's Diabetes Specialties Centre, which has a network of 45 diabetes centers across 10 states of India. In 2017, 16,226 individuals with diabetes were screened for diabetic retinopathy. The retinal images taken using Remidio FOP camera were transferred through local area networks and wide area networks to enable remote diabetic retinopathy grading by the ophthalmologists at the main hospital at Chennai (Fig. 1).
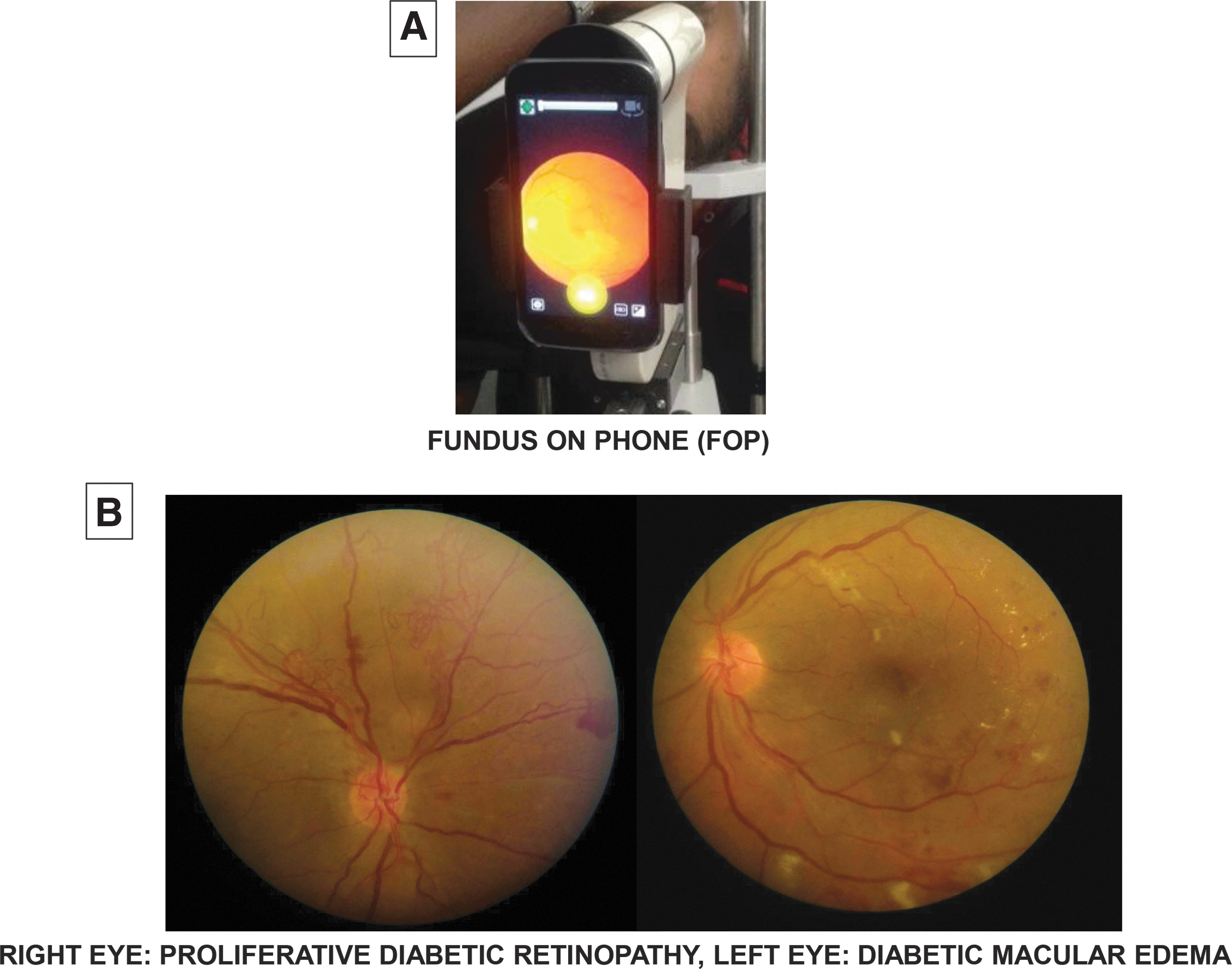
Smartphone-based fundus camera for teleophthalmology, for diabetic retinopathy screening. The figure shows the retinal photographs of a 40-year-old male with type 2 diabetes of 3-year duration seen at a remote village in southern Tamil Nadu. The patient had no ocular symptoms and a normal vision (6/6) in both eyes. The retinal photographs taken using Remidio FOP camera showed proliferative diabetic retinopathy in the right eye and severe diabetic macular edema in the left eye. After teleconsultation with the ophthalmologist at the base hospital at Chennai—400 km away—regarding his diabetic eye condition and after reviewing his retinal photographs, he was asked to undergo further investigations and treatment for sight-threatening diabetic retinopathy. Early timely detection of diabetic retinopathy by teleophthalmology thus helped this patient to safeguard his vision. FOP, fundus on phone.
Using the International Clinical Classification of Diabetic Retinopathy grading system, 40 diabetic retinopathy was detected in 3701 (22.8%) individuals, of which 1140 (7.02%) had sight-threatening diabetic retinopathy that required referral for further evaluation and treatment. The smartphone-based retinal imaging system, FOP, is reasonably sensitive and specific for diabetic retinopathy detection and, thus, is, useful as an effective screening tool for diabetic retinopathy. 39
Ophthalmoscopy versus teleophthalmology for diabetic retinopathy screening
Two important aspects which need to be considered for the sustainability of a rural outreach telescreening program are cost-effectiveness and patient satisfaction levels. Table 1 shows the differences between ophthalmologist assessment versus teleophthalmology-based assessment of diabetic retinopathy. Gomez-Ulla et al. performed a cost analysis for diabetic retinopathy screening by ophthalmoscopy versus teleophthalmology. 41 Results showed that although ophthalmoscopy was less expensive, compared to the higher initial investment for a teleophthalmology setup, the latter was found to be more beneficial for the people screened as discussed in Table 1.
Ophthalmoscopy Versus Telemedicine for Diabetic Retinopathy Screening
One of the possible limitations in a teleophthalmology program is that there is no face-to-face personal interaction with the doctor, with which many patients are most familiar. However, even in telemedicine, the patients do have virtual access to the medical specialist. Some studies have addressed this concern and report excellent patient satisfaction levels (94%) with teleophthalmology screening. 42,43
Artificial intelligence in diabetic retinopathy detection in telemedicine
The use of artificial intelligence (AI) to analyze retinal images and provide grading of diabetic retinopathy and referral recommendations accurately has generated great interest recently among physicians and other health care personnel. 44,45 AI is an appealing concept as it fits in with the current trend of teleophthalmology/telemedicine, and automation of retinal image analysis offers opportunities to expand the telescreening services to more remote areas. 46,47 AI-based diabetic retinopathy grading algorithms could potentially expedite early detection of diabetic retinopathy happening at the primary care level, and thus would be useful in reducing the burden to the health systems in screening large numbers of people with diabetes. 45,47 Only people who have sight threatening/referable diabetic retinopathy would need to be referred to the ophthalmologist/retina specialist. 45
Benefits of telemedicine in LMIC
The multiple benefits of telemedicine in LMIC are depicted in Figure 2. Telemedicine helps detect and manage chronic diseases such as diabetes in remote rural areas where such medical facilities are not available, accessible, and affordable. It provides individualized health information, facilitates clinical decision making, increases awareness on diabetes through education, provides easy accessibility to diabetes care at their doorsteps, and improves the quality of life of individuals with diabetes. If used effectively in remote rural areas, the telemedicine model can dramatically reduce the number of patients who need to travel to specialized centers in urban areas to get proper diagnosis and treatment, which would likely improve adherence rates.
Benefits of telemedicine.
In a 2006 study, Paul et al. conducted a survey to assess patient satisfaction levels and factors influencing satisfaction during teleophthalmology consultations in India. 43 A total of 348 adults responded to the survey. Some of the main reasons respondents reported for increased satisfaction with the diabetic retinopathy telescreening were reduced travel time, lower travel costs, and easier access to clinical support systems. 43 From a health care provider perspective, this program is cost-effective as it does not require the full-time services of highly qualified specialists. Several studies on cost-effectiveness have demonstrated that teleophthalmology holds great promise compared with traditional ophthalmologist examination. 48 –50 A systematic review of 16 studies of teleophthalmology screening for chronic eye diseases, which examined the cost-effectiveness of teleophthalmology compared with traditional ophthalmologist examination, after accounting for initial capital costs, concluded that teleophthalmology is cost saving, regardless of geographical setting and with evidence of acceptability among patients and providers. 48
Cost-effectiveness of teleophthalmology depends on the administrative costs of establishing and maintaining screening at regular intervals and on achieving sufficient coverage. 50 In addition, teleophthalmology, compared to conventional care, has been reported to be an accurate and reliable test for detecting diabetic retinopathy and macular edema. 51 Thus, telemedicine provides flexibility and real-time care with health care providers working in resource-constrained settings where, presently, this may be the only alternative.
Barriers and Challenges to Telemedicine
Although telemedicine clearly has a wide range of potential benefits, it also has some disadvantages/barriers. According to the World Health Organization, the biggest barrier to the implementation of telemedicine programs, globally, is the perception that the costs of setting up the telemedicine unit are too high (60% of responding countries consider this as a barrier). 52 For developing countries, high costs, underdeveloped infrastructure, and lack of technical expertise are just some challenges. 52 Legal issues surrounding patient privacy and confidentiality, competing health system priorities, and a perceived lack of demand are other barriers to large-scale implementation of telemedicine. 53
Some people worry about a potential breakdown in the relationship between health care provider and patient. In addition, organizational and bureaucratic difficulties are likely to be present due to lack of personal contact. A systematic review, which assessed 50 studies on telemedicine, concluded that evidence regarding the effectiveness or cost-effectiveness of telemedicine is still limited and that only a few telemedicine applications can be recommended for broader use. 54
Various potential technical and structural problems could also hinder the adoption of telemedicine programs. Lack of connectivity between stand-alone diabetes telemedicine systems and hospital electronic medical records, inadequate data encryption and security systems to fully ensure patient privacy, and inadequate decision support software are some of the issues currently facing telemedicine programs, all of which obviously, need to be addressed. 54
Conclusion
In low- and middle-income economies, innovative approaches, including telemedicine, mobile technology, internet, and websites, can be adapted to prevent and manage diabetes in the community. Using these technologies, clinicians can reach out to remote and underserved communities and serve patients at their doorstep.
Telemedicine is a valuable, cost-effective and reliable tool for screening people with diabetes for various complications, and it provides people in rural areas access to many virtual “super specialists” in the field of medicine. As such, it holds great promise for enhancing the quality of care, improved access to care in remote areas, and prevention and detection of noncommunicable diseases, including diabetes.
In summary, telemedicine bridges the gap between primary care and secondary/tertiary care. However, using this technology requires services of expert teams working collaboratively to provide care and follow-up. There is ample scope for telemedicine to improve diabetes care outcomes by reducing the rate of secondary complications in both developed and developing nations. Successful telemedicine-driven diabetic complication screening could reduce the risk of microvascular and macrovascular complications due to diabetes and, thereby, the health care burden.
One could anticipate that the use of automated AI software combined with telemedicine could enable efficient real-time screening of complication like retinopathy in people with diabetes, in remote areas where such facilities are currently not available.
Footnotes
Acknowledgments
The authors also wish to thank Christopher G. Parkin (CGParkin Communications, Inc., Henderson, NV) for editorial assistance. Roche Diabetes Care provided funding for the development of this article.
Author Disclosure Statement
R.P., R.R., and V.M. have no conflict of interests to disclose for this article.