
Abstract
Background:
The majority of therapies have generally targeted fasting glucose control, and current mealtime insulin therapies have longer time action profiles than that of endogenously secreted insulin. The primary purpose of this study was to assess both glucose time-in-range (TIR: 70–180 mg/dL) and postprandial glucose excursions (PPGE) in 1–4 h using a real-time continuous glucose monitor (CGM) with Technosphere insulin (TI) versus insulin aspart in patients with type 1 diabetes (T1DM) on multiple daily injections (MDI).
Research Design and Methods:
This pilot, investigator-led, collaborative, open-label, multicenter, clinical research trial enrolled 60 patients with T1DM with HbA1c levels ≥6.5% and ≤10%. Individuals were randomized to treatment with titrated TI (n = 26) or titrated insulin aspart (n = 34), stratified by baseline HbA1c levels (≤8% or >8%). All were required to wear a real-time CGM throughout the trial. All patients in the TI group were advised to take supplemental inhalations at 1 and 2 h after meals if indicated based on postprandial glucose (PPG) values. The coprimary outcomes were assessed both in the full intent-to-treat population and in those individuals randomized to TI who were compliant with supplemental doses ≥90% of the time (n = 15). The CGM data were analyzed using linear regression models.
Results:
Overall, those treated with TI versus aspart achieved comparable TIR, but less time spent in hypoglycemia (<60 and <50 mg/dL, both P < 0.05). In the TI-compliant group (n = 15), TIR was significantly greater (62.5% ± 2.6% vs. 53.8% ± 1.7%, P = 0.009) and time in hyperglycemia >180 mg/dL was lower (34.2% ± 2.7% vs. 41.0% ± 1.7%, P = 0.045) as compared with the aspart group. PPG was also significantly lower in the TI cohort at 60 and 90 min postmeal, and PPGE were lower in the TI-compliant group as compared with the aspart group over 1–4-h postmeal (P < 0.05). In addition, there was weight gain in the aspart group compared with weight loss in the TI group (P = 0.006) despite higher prandial TI insulin dose.
Conclusions:
We conclude that using TI appropriately at mealtimes with supplemental dosing improves prandial glucose (TIR and 1–4 h) control without any increase in time in hypoglycemia or weight gain in patients with T1DM on MDI. The study results support a larger study using a treat-to-target design to confirm these findings.
Clinical trial reg. no. NCT03143816,
Introduction
T
Technosphere Insulin (TI, Afrezza®; MannKind Corporation, Westlake Village, CA) is a dry-powder formulation of recombinant human insulin adsorbed onto Technosphere microparticles for oral inhalation. 7 Furmaryl diketopiperazine, a biologically inert excipient, forms the Technosphere particle matrix. 8,9 TI has a faster onset of action (∼12 min) and shorter duration of action (∼2 h) compared with the currently available RAIAs (aspart, lispro, or glulisine) with a peak effect of 35–45 min due in great part to its rapid absorption from the lung. 10 –12
An initial study using TI demonstrated noninferiority in glucose control when compared with insulin aspart in patients with T1DM using MDI. 13 This registration study also documented fewer hypoglycemic events with lesser weight gain in subjects with T1DM. 13 Another small pilot feasibility single-arm study (using additional inhalations after meals) showed improvement of HbA1c in 6 weeks using TI. 14 However, to the best of our knowledge, no randomized clinical trials have been conducted to assess the role of additional postprandial inhalations (“treat to target design”) utilizing continuous glucose monitoring (CGM) on overall glucose control, including time-in-range (TIR), prandial glucose excursions, and time in hypoglycemia. We performed this 4-week pilot investigator-led, collaborative open-label multicenter randomized clinical trial, to evaluate the effect of TI versus subcutaneous RAIA insulin (aspart) on PPG control assessed by TIR and PPGE as measured by real-time CGM.
Research Design and Methods
This study was a pilot, randomized, multicenter (five centers in the United States), 4-week active treatment trial. Adults (≥18 and ≤70 years) with T1DM for at least 6 months with HbA1c 6.5%–10.0% were enrolled between June 2017 and December 2017. Major inclusion criteria included: nonsmoking adults, body mass index (BMI) ≤35 kg/m2, forced expiratory volume in 1 s (FEV1) ≥70% predicted, on MDI, stable insulin dose ≥3 months, and using insulin degludec or glargine as basal insulin. Major exclusion criteria included: pregnancy, any pulmonary disease, severe hypoglycemia that required assistance in the last 3 months, currently smoking or marijuana use, using insulin detemir or Neutral Protamine Hagedorn (NPH) as basal insulin, and a need for >18 U of prandial insulin per meal (Table 1).
BMI, body mass index; CGM, continuous glucose monitor; GLP-1, glucagon-like-peptide-1; NPH, neutral protamine hagedorn.
At the screening visit, all patients had an Electrocardiogram (EKG), physical exam, complete metabolic panel, and spirometry tests. Spirometry (FEV1 and FVC) was performed at baseline, and at weeks 2 and 4 during the treatment period in both groups. Safety and adverse events were assessed. Subjects who had a decrease of ≥20% of FEV1 at any of the follow-up study visits were withdrawn (none of the study participants met these criteria).
There were a total of seven clinic/phone visits during the study period (Fig. 1). Patients had a screening visit followed by a randomization clinic visit within 1 week. Other visits included: two additional clinic visits at weeks 2 and 4 after randomization, and four phone visits at weeks 1, 3, and 5; and 1 week following the completion of the study. This study was approved by appropriate Institutional Review Boards and monitored by an independent contract research organization. All patients provided written informed consent.
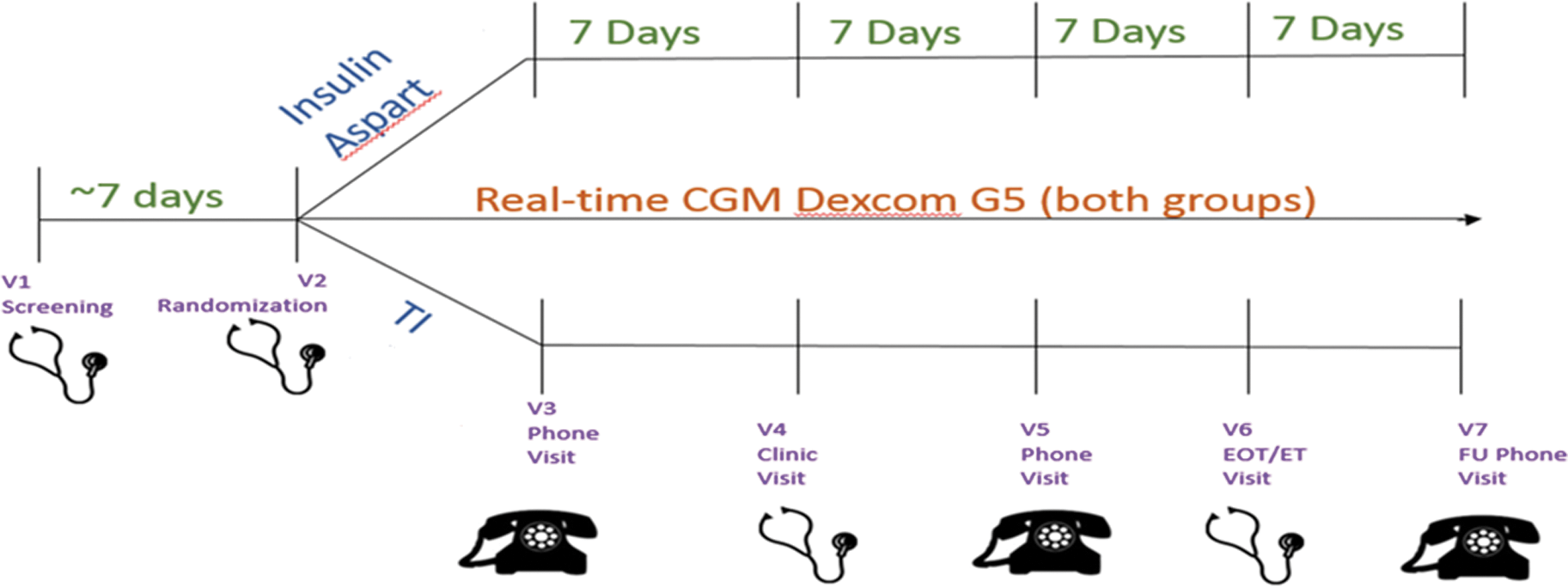
Study design.
Patients were randomized 1:1 to TI or insulin aspart group using a blocked design, stratified by screening HbA1c (≤8% or >8%). All patients used Dexcom G5® (San Diego, CA) real-time CGM during the study period. Patients randomized to aspart continued the same bolus regimen as used before randomization. If patients were using any other RAIA (other than aspart), they were switched to aspart on the same dose at the randomization visit. Patients in the aspart group were also allowed to change their premeal bolus dose and take postprandial and other correction doses as deemed clinically necessary.
Patients randomized to TI were provided with an insulin dose conversion table (Table 2). For example, up to 4 U of injectable RAIA was converted to 4 U of TI. Patients taking 5–8 U of RAIA were advised to uptitrate to 8 U of TI. Patients in the TI group were also advised to take additional inhalations at 1 and 2 h postprandially as indicated based on PPG values (Table 2). At 1 h after the meal, patients were instructed to take an additional 4 U of TI if PPG 151–200 mg/dL or 8 U if PPG was ≥201 mg/dL. If PPG was ≥201 mg/dL at 2 h, patients were instructed to take 4 additional units of TI (Table 2). During the study, patients were recommended not to change their basal insulin dose. After completion of the 4-week study, patients reverted to their standard diabetes care.
Two-hour correction used only if blood glucose is ≥201 mg/dL and has not decreased by ≥50 mg/dL between 1 and 2 h.
The primary efficacy endpoints were TIR for glucose and PPGE in 1–4 h from the CGM data. The secondary efficacy endpoints included: change in HbA1c, under the curve (AUC) for PPG, hypoglycemia (defined as time below range: <70, <60, and <50 mg/dL), hyperglycemia (defined as time above range: >180 mg/dL), and glucose variability indices (standard deviation [SD] and coefficient of variation).
PPGE was defined as the difference between the highest CGM glucose level 1 to 4 h after a meal and the premeal CGM glucose level. 15 Other glucose measurements from CGM data included: PPG, mean sensor glucose (mg/dL), AUC (min × mg/dL), and TIR as a percent of a 24-h day. In addition to the planned intention-to-treat comparison between the aspart and TI groups, a comparison of compliant versus noncompliant patients in the TI group was included in a posthoc per-protocol analysis, as it was noted that some study participants were not compliant with the postprandial dosing protocol. Compliance with TI use was based on using TI per protocol at 1- and 2-h postmeal based on PPG values. Patients were defined as compliant if ±90% of postmeal TI dosages were taken per protocol, with at least one of the postmeal inhalations taken if indicated per meal. The purpose of this posthoc analysis was to generate hypotheses and plan for a future, larger clinical trial.
Baseline characteristics of the study cohort were compared by randomization group using a student's t-test, and CGM data were analyzed by study group using linear regression models. CGM data were aggregated per study week, to control for any changes in efficacy or compliance over time. Change in insulin bolus dose was examined in both the TI group and the aspart group; however, acknowledging that dosing between TI and aspart is not equivalent, 16 these comparisons were to determine the change in bolus dosing over the course of the study.
Results
Sixty patients were randomized to TI (n = 26) and insulin aspart (n = 34). Four patients in the TI group were excluded from the final analysis (two dropped out the study due to non-side-effects-related reasons, and one had no CGM data and the other had incomplete CGM data (with the first 2 weeks of the study data missing). As shown in Table 3, baseline characteristics, including age, diabetes duration, gender, HbA1c, BMI, blood pressure, daily total basal dose, or daily total bolus dose were similar in the two groups. The baseline or end-of-the-study FEV1 did not differ by treatment group. There were no reported episodes of severe hypoglycemia in either group during the study, although four participants (all in the aspart group) reported hypoglycemia that patients were able to treat themselves. Three participants in the TI group reported mild cough, and one additional participant in the TI group reported having difficulty inhaling the TI initially, but this was resolved by drinking water (as reported by the patient).
Data are mean ± SD. Baseline characteristics were similar.
BP, blood pressure; FEV1, forced expiratory volume in 1 s; SD, standard deviation.
In univariate comparisons of daily insulin dose (total basal, total bolus, premeal bolus, postprandial bolus, and correction doses) by treatment group (Table 4), the TI group reported a significantly higher total daily bolus dose when compared with the aspart group (mean ± SD 38.5 ± 17.2 vs. 20.6 ± 7.8 U per day, respectively, P < 0.0001). In linear regression mixed models, daily bolus dose did not differ by study week (P-value for week by treatment group interaction, P = 0.12). Patients in the TI and aspart groups took a similar dose of premeal insulin (22.7 ± 12 vs. 19.0 ± 7.2 U, respectively, P = 0.17, Fig. 2). Overall patients in the TI group took TI at 1- and 2-h postprandial 27% of the time, totaling 11.4 ± 8.2 U of postprandial supplemental bolus doses per day. Detailed information about the insulin dosing in the TI group, including the average 1- and 2-h post-prandial (PP) dose taken per person, the percentage of time when additional doses were indicated and taken as indicated, and the average PP dose used when taken is shown in Supplementary Table S1. Meal-specific bolus doses taken by the aspart group are also shown in Supplementary Table S1. The patients in the aspart group took additional bolus doses of 1.6 ± 1.8 U per day. The TI group also reported taking additional doses of 4.4 ± 5.2 U per day, significantly higher than the additional doses reported in the aspart group (Fig. 2, P = 0.01). Despite higher bolus insulin doses reported in the TI group, we observed slight but not significant weight loss in the TI group versus significant weight gain in the aspart group (weight change, TI group: −0.22 ± 1.3 kg versus aspart group: +0.76 ± 1.3 kg, P = 0.006), suggesting that the increased TI bolus insulin dose did not lead to weight gain in the TI group.
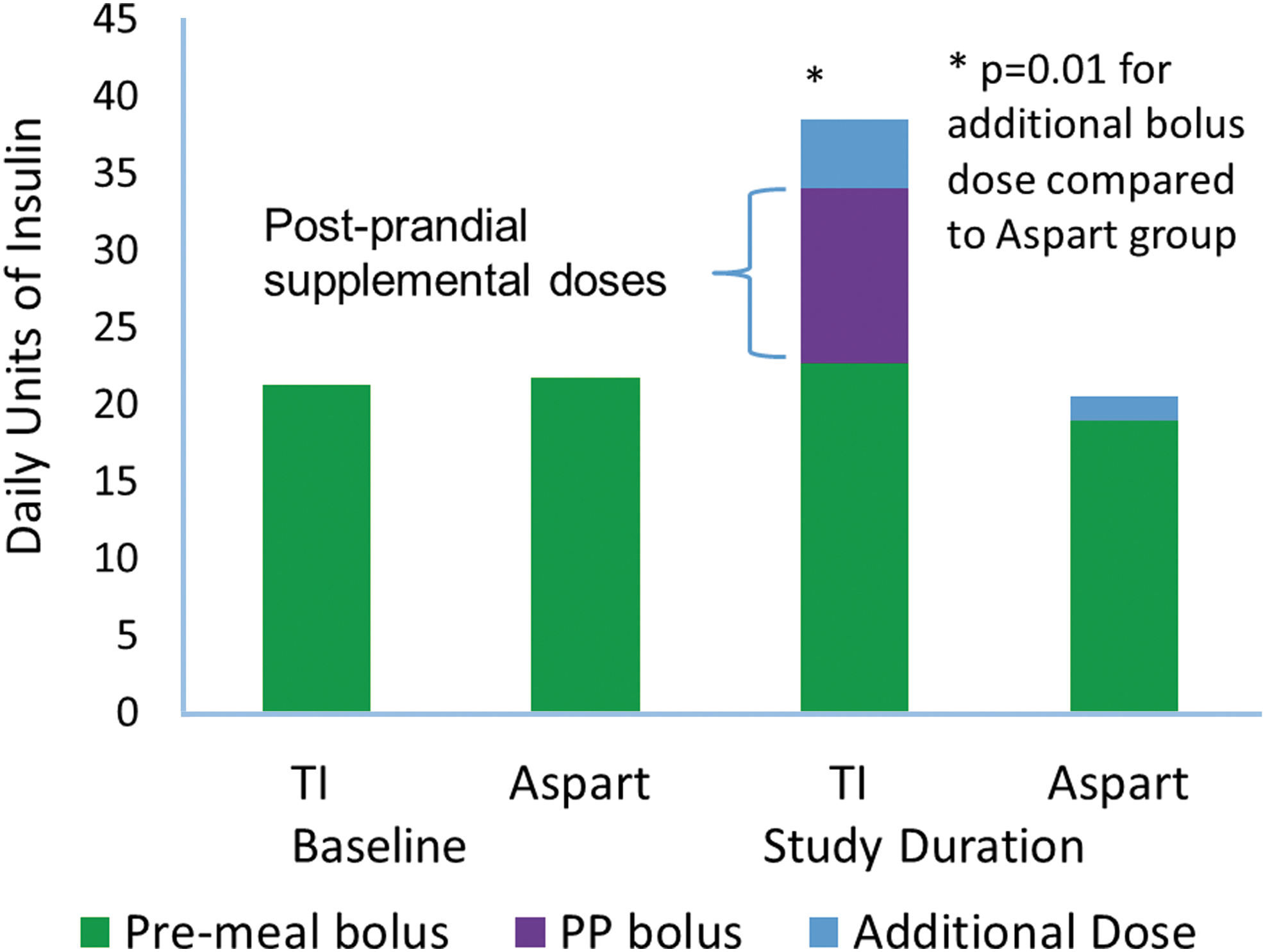
Mean premeal and postprandial bolus dose, comparison of insulin aspart and TI groups. In linear regression models with repeated measures, adjusted for age, sex, study site, study week, and treatment group, the TI group used a similar premeal bolus, but a significantly larger additional bolus dose when compared with the aspart group. In addition, the TI group took planned postprandial supplemental doses per protocol (PP bolus). Average postprandial bolus was significantly higher in the TI group. PP, post-prandial; TI, Technosphere Insulin.
Mean ± SD, unadjusted.
LS mean ± SE, adjusted for age, sex, study site, study week, screening HbA1c, and total daily insulin dose.
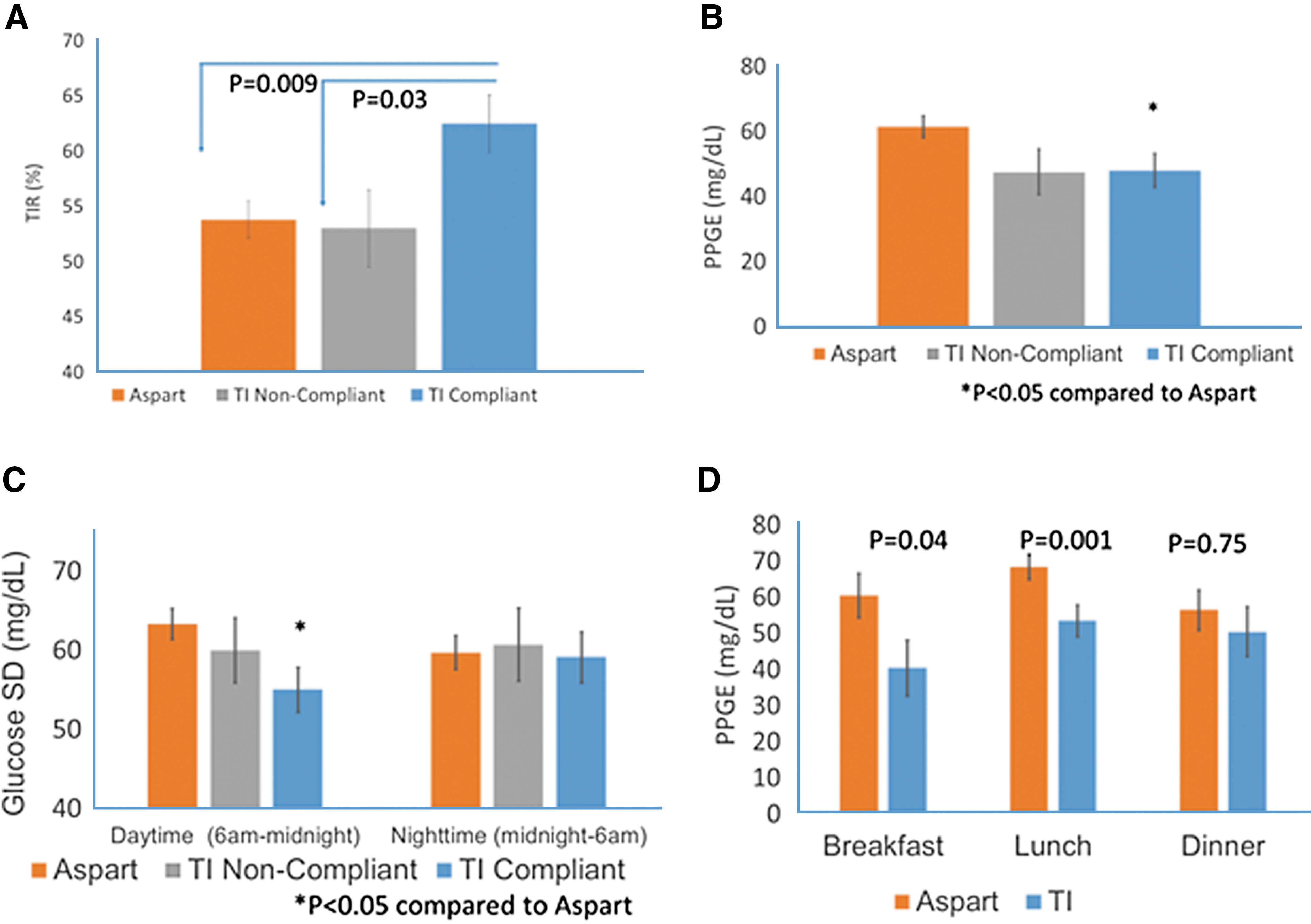
Twenty-two patients in the TI group and 34 patients in the aspart group were included in data analysis for CGM data, using linear regression models with repeated measures adjusted for age, sex, study site, study week, screening HbA1c, and total insulin dose. Glucose SD and percentage of time spent in hypoglycemia (<60 and <50 mg/dL) were significantly lower in the TI group compared with the aspart group (Table 4). Mean sensor glucose, percentage of time in hypoglycemia <70 mg/dL, and percentage of time in hyperglycemia were all numerically lower in the TI group but the differences were not statistically significant. TIR was numerically higher but also not statistically different in the TI group (Table 4). Out of 22 patients in the TI group, 15 (68%) were compliant and 7 were noncompliant, with average compliance in the whole group of 91% ± 11%. Patients in the TI-compliant group had significantly higher TIR, lower glucose SD, and less time in hyperglycemia than patients in the aspart group (Fig. 3A and Table 5, respectively). Patients in the TI-noncompliant group had significantly higher time spent in hyperglycemia (>180 mg/dL) and spent less TIR when compared with compliant patients in the TI group (Table 5).
Comparison of insulin aspart and TI groups for TIR, postprandial glucose excursions, and SD.
LS means ± SE, adjusted for age, sex, and study site.
P < 0.05 compared with Standard Treatment Group.
P < 0.05 TI-noncompliant compared with TI-compliant Group.
LS means ± SE, adjusted for age, sex, study site, and total insulin dose.
PPGE were significantly lower in the TI-compliant group than the aspart group (Fig. 3B). PPGE was significantly lower in the TI-compliant group compared with the aspart group at breakfast and lunch but not at dinner (Fig. 3D).
CGM glucose SD during daytime (6 AM to midnight) was significantly lower in the TI-compliant group compared with the aspart group (Fig. 3C). However, there was no difference between groups for the CGM glucose SD during nighttime (Midnight to 6 AM).
The AUC for 2-h PPG was significantly lower in the TI-compliant group than the aspart group and the TI-noncompliant group (Fig. 4A). As shown in Figure 4B, when examined by time of day, TIR was significantly higher in the TI than the aspart group during the daytime (6am–midnight) but not different at night (midnight–6am).
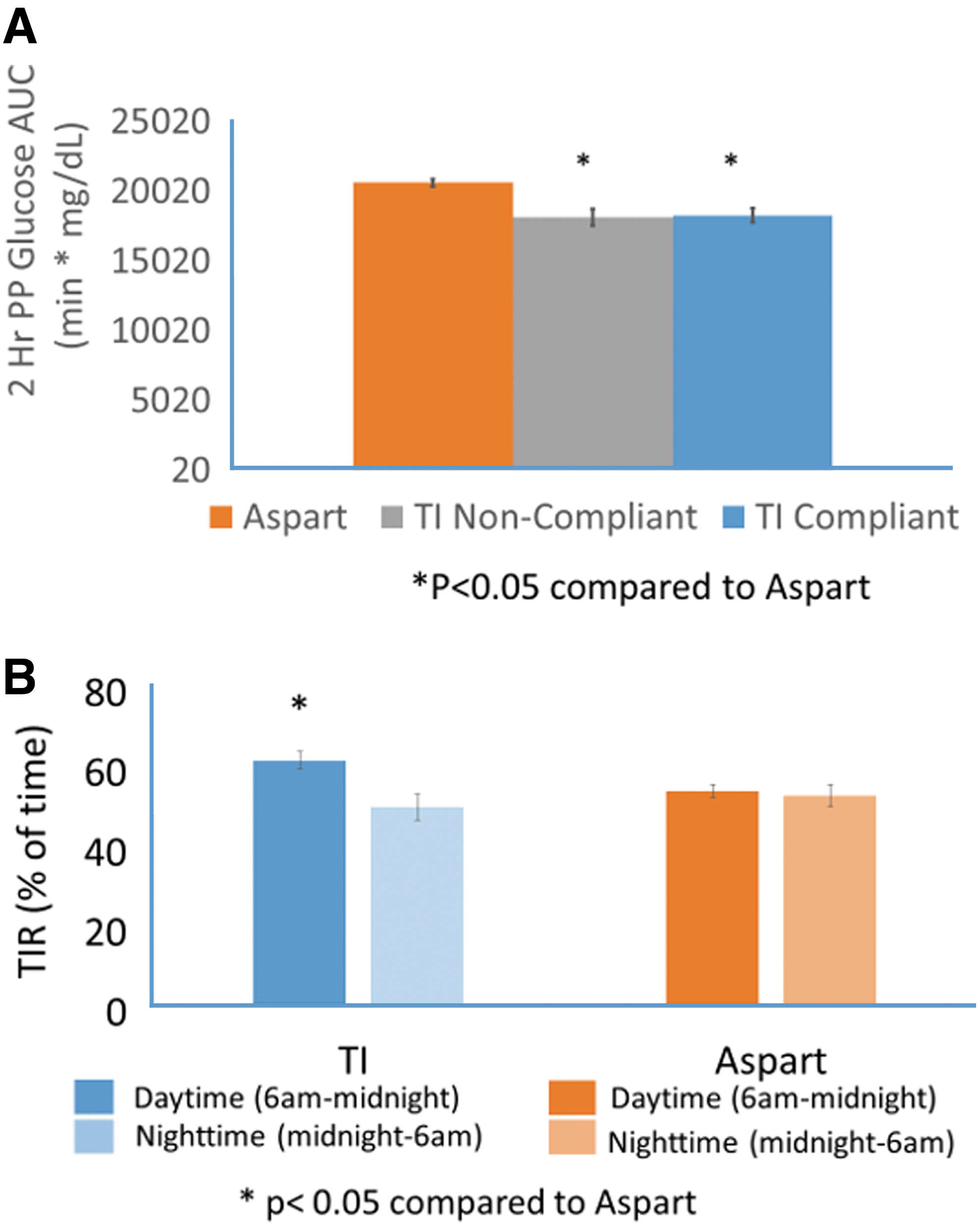
2-h Postprandial AUC and TIR by time of day, comparison of insulin aspart and TI groups.
As shown in Figure 5, PPG values premeal did not differ between the TI group overall and the aspart group, but at 60 and 90 min after meals PPG values were significantly lower in the TI than the aspart group. At 2 h PPG values were also numerically lower but this trend was not statistically significant. Similarly, no significant differences at 150, 180, 210, and 240 min postmeal PPG were observed. However, when comparing the aspart group and the TI-compliant group, PPG was significantly lower in the TI-compliant group compared with the aspart group at 60, 90, and 120 min after meals (Fig. 5). There was no difference in premeal glucose level between the TI-compliant and aspart groups, but the TI-noncompliant group had higher premeal PPG levels than the TI-compliant group (Fig. 5).
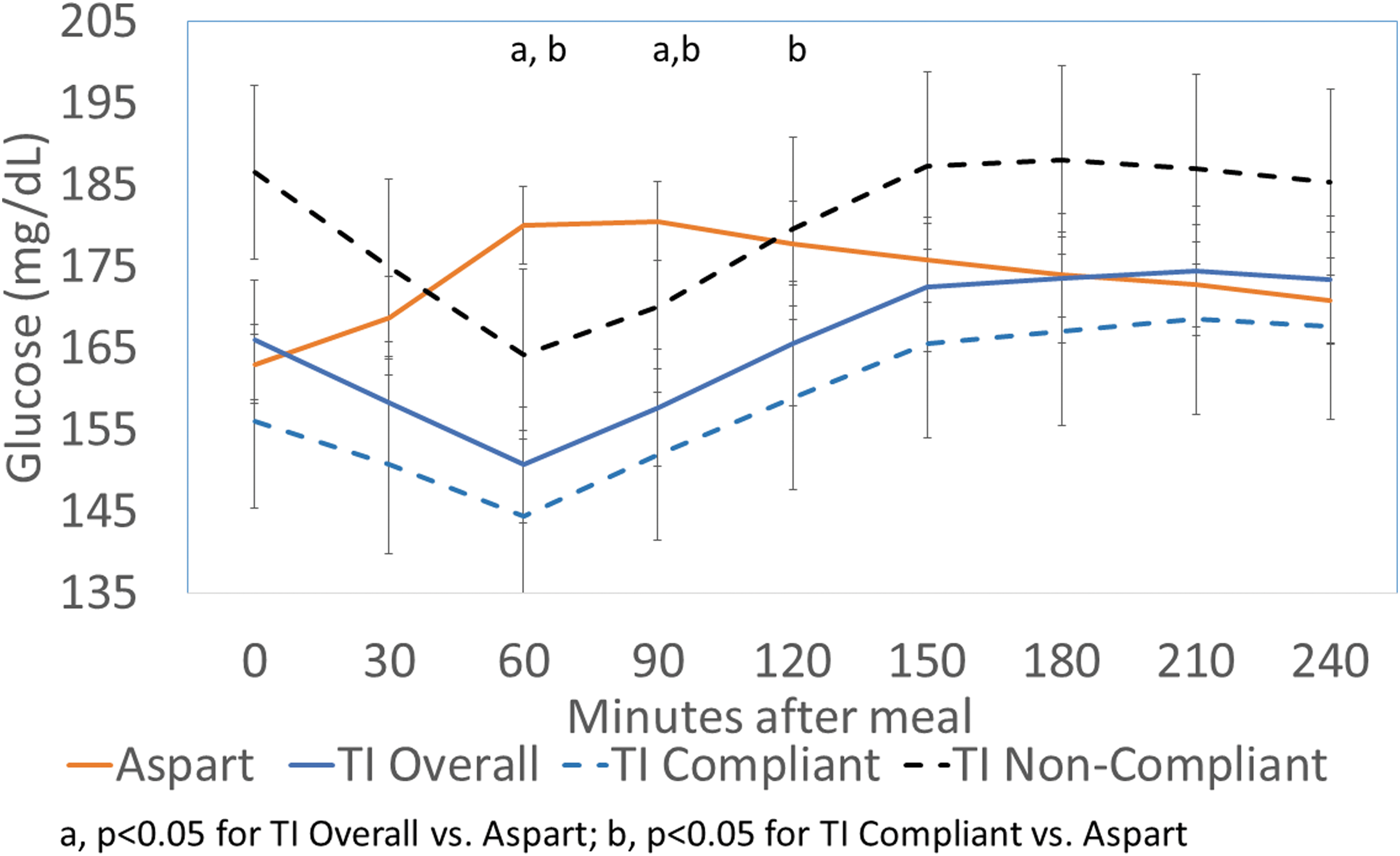
Mean CGM glucose, comparison of insulin aspart and TI groups. Mean postprandial CGM glucose by treatment group and compliance. PPG values were significantly lower at 60 and 90 min in the TI group compared with the aspart group. PPG values were significantly lower at 60, 90, and 120 min after meals in the TI-compliant group compared with the aspart group.
While there was no difference in HbA1c by the study group at either screening or at the study end, participants in the aspart group had a significantly greater decrease in HbA1c than those in the TI group (Table 4) between screening and the end of the study (4 weeks). This may be due to slightly higher baseline HbA1c values in the aspart group, as the mean 24-h glucose was similar in the two groups.
Discussion
The STAT study, to the best of our knowledge, is the first to demonstrate that conversion to use of TI achieved significantly greater improvement in postprandial glucose, increased daytime TIR, decreased PPGE and hypoglycemia, and lesser overall and daytime glucose variability, although these improvements were modest. Furthermore, when used as instructed per protocol, the use of TI also increased 24-h TIR. While nighttime glucose SD were similar in both cohorts, this observation is not surprising given the short duration of action of TI.
PPGE was significantly improved in the TI group compared with the aspart group at breakfast and lunch in our study. However, no difference was observed at dinner in this pilot investigation. The potential reasons for this observation at dinnertime include the fear of hypoglycemia overnight–an experience that might be anticipated with an insulin with longer duration of action. However, as the vast majority of T1DM patients currently use subcutaneous RAIA, many may be reticent to use postprandial corrections later in the day. 17,18 As TI has a shorter duration and a faster action profile compared with currently available mealtime injectable insulins, this may offer an advantage to both minimize the risk of nocturnal hypoglycemia and increase the use of supplemental or corrective doses before bedtime. 11 Our study suggests that patients using TI may benefit from additional education and reassurance to both understand the time action profile and appropriately take advantage of the ultra-rapid action of TI after meals.
In the TI group, about a third of patients were not compliant with the study protocol for non-side-effects-related reasons. Despite significant education of the time action profile of TI as compared with aspart, patients in this study were naive to TI and this may have resulted in a reluctance to use the recommended doses. Similarly, while both aspart and TI are dosed in units, TI starting doses are currently advised to be ∼1.5 times of the usual subcutaneous doses. 16 The recently updated TI product label has a starting dose conversion chart and patients are recommended to titrate the dose after initiation, 12 but patients naive to TI therapy may understandably be hesitant to take larger doses due to the risk of hypoglycemia and nonfamiliarity. A comparison of glucose response, measured by glucose infusion rate (GIR) showed that 12 U of TI had a similar but faster peak compared with 8 U of insulin lispro. 16 Equivalent TI units are generally 1.5 to 2.0 times the injectable insulin units to reach a similar potency in clinical practice. 19,20 Bolus doses in the TI group increased about two-fold in this study, consistent with the expected dose conversion ratio based on GIR data.
While these data support that TI significantly improve both TIR and PPGE, the current study also has limitations. First, despite stratification of HbA1c, patients in the aspart group had slightly, although not significantly, higher HbA1c than the TI group. This may explain the decrease in HbA1c in a short period of time (4 weeks) in the aspart group as compared with TI-treated individuals. Second, this pilot study did not have a run-in phase to optimize insulin dosing before randomization, and in addition to the study's short duration, may have limited the magnitude of differences between groups. Third, patients not used to having worn CGM in the past might have had an independent impact of CGM that is separate from the effect of TI or aspart. Fourth, this pilot study had a relatively small sample size, which may have resulted in the study being underpowered to observe some actual differences. Lastly, the high percentage of TI insulin administered postprandially suggests that higher doses of TI should have been given preprandially. While the TI algorithm used in this study led to the modest improvements (vs. aspart) described above, further studies are needed to replicate these findings and to provide guidance for more effective dosing of TI.
Conclusions
In summary, when dosed as instructed, TI significantly improved postprandial glucose without increasing hypoglycemia or weight gain as well as all day glucose TIR. Furthermore, TI decreased daytime glucose variability and reduced time spent in hypoglycemia. The faster onset of action and shorter duration profile of TI, when compared with RAIAs, may provide a flexible approach for patients to optimize postprandial glucose control without an increased risk of hypoglycemia. A larger study in insulin-requiring patients with diabetes with a treat-to-target design would provide the opportunity to confirm these findings.
Footnotes
Acknowledgment
This study was funded by MannKind Corporation.
Author Disclosure Statement
H.K.A. received a research grant from MannKind Corporation through the University of Colorado related to this study. S.K.G. received research grants from MannKind Corporation, Eli Lilly, Novo Nordisk, Merck, Lexicon, Medtronic, Dario, NCI, T1D Exchange, NIDDK, JDRF, Animas, Dexcom, and Sanofi through University Colorado; received consulting fees for advisory boards from MannKind, Dexcom, Eli Lilly, Novo Nordisk, Sanofi, Roche, Merck, Lexicon, and Medtronic. T.S.B. received research grant from Abbott, Ambra, Ascensia, BD, Boehringer Ingelheim, Calibra Medical, Companion Medical, Dance Biopharm, Dexcom, Eli Lilly, Glooko, Glysens, Kowa, Lexicon, MannKind, Medtronic, Novo Nordisk, Sanofi, Senseonics, Taidoc, Versartis, and Xeris; received consulting honoraria from Abbott, Astra Zeneca, Ascensia, BD, Calibra, Capillary Biomedical, Eli Lilly, Intarcia, Medtronic, Novo Nordisk, and Sanofi; and received speaking honoraria from Abbott, Eli Lilly, Medtronic, Novo Nordisk, and Sanofi. L.J.K. received research grants from Sanofi, Gan and Lee, Oramed, Lilly, Novo Nordisk, Janssen, MannKind, Dexcom, Medtronic, Senseonics, Abbott, Pfizer, and Mylan. A.P. received research support from Astra Zeneca, Dexcom, and MannKind, speaker's bureau from Novo Nordisk; participated on advisory boards for Abbott Diabetes Care, Becton Dickinson, Boehringer Ingelheim, Eli Lilly and Company, Lexicon, Livongo, Medscape, Merck, Novo Nordisk, OptumHealth, Sanofi, and Science 37. B.W.B. received research grant by Atlanta Diabetes Associates from Abbott, Becton Dickinson, Dexcom, GSK, Diasome, Jannsen, Lexicon, Lilly/Boehringer Ingelheim, MannKind, Medtronic, NIH, Novo Nordisk, Sanofi, and Senseonics; consultant fee from Adocia, Intarcia, Janssen, Medtronic, MannKind, Novo Nordisk, Sanofi; speaker's bureau from Astra Zeneca, Lily/Boehringer Ingelheim, Jannsen, Medtronic, Novo Nordisk, and Sanofi; and has stocks of Aseko. A.R. and J.S.B. do not have any conflict of interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.