
Abstract
Objective:
Sudomotor dysfunction may be an early detectable abnormality in diabetic small fiber neuropathy. The aim of this study was to evaluate the efficacy of Sudoscan™ (Impeto Medical, Paris, France) in detecting diabetic neuropathy (DN), in comparison with other standardized tests, in patients with diabetes mellitus (DM).
Subjects and Methods:
Sudoscan measures electrochemical skin conductance (ESC) of hands and feet through reverse iontophoresis. We evaluated 83 DM patients with and without DN and 210 healthy controls (HCs). Neuropathy Impairment Score—Lower Legs (NIS-LL), quantitative autonomic function testing (QAFT), and quantitative sensory testing (QST) were performed. Symptomatic pain was recorded using a visual analog scale. Receiver-operator characteristic (ROC) curves were calculated to evaluate the efficacy of Sudoscan in detecting DN compared with traditional modalities.
Results:
Diabetes patients with DN had significantly worse ESCs of feet and hands than DM patients without DN and HCs (respectively, 56.3±3 vs. 75.9±5.5 and 84.4±0.9 [P<0.0001] for feet and 51.9±2.4 vs. 67.5±4.3 and 73.1±0.8 [P<0.0001] for hands). Increasing NIS-LL scores were associated with decreasing ESC values. ESCs correlated significantly with clinical (NIS-LL), somatic (QST), and autonomic (QAFT) measures of neuropathy and with pain scores. ROC curve analysis showed significant results for both hands and feet ESC (area under the curve of 0.86 and 0.88, respectively; P<0.0001) with sensitivity of 78% and specificity of 92% for feet to detect DN.
Conclusions:
Sudoscan is a promising, sensitive tool to detect neuropathy in patients with DM. This is a very simple, easy-to-perform test that can be done in the clinical setting in 3–5 min.
Introduction
Changes in peripheral autonomic nervous system function are an early manifestation of distal small fiber neuropathy. 1 Sudomotor dysfunction is one of the earliest detectable neurophysiologic abnormalities in distal small fiber neuropathies. Sweat glands are innervated by small, unmyelinated sympathetic C nerve fibers that are responsible for the sweat response. Skin biopsies have confirmed that numbers of epidermal C-nerve fibers are reduced in patients with diabetes. 4 Furthermore, degeneration of small C-fibers innervating sweat glands has been observed in diabetes patients. Abnormalities in sudomotor function in diabetes patients were noted to correlate with the presence of autonomic neuropathy. 5 Thus, sudomotor function represents an attractive tool to evaluate the peripheral autonomic system in people with DM. 6 The various techniques of sudomotor function testing are variably sensitive and specific for the detection of distal small fiber neuropathy. 7 However, most have remained underutilized in clinical practice because of lack of availability, inconsistency of results, and technical demands of the tests, with some being tedious, cumbersome, and time consuming.
Sudoscan™ (Impeto Medical, Paris, France), a simple, noninvasive, easy-to-perform sudomotor test, was recently developed to allow the measurement of sweat gland function. 8 –10 This test is based on the electrochemical reaction between the chloride ions in sweat and stainless steel-based plate electrodes, on which the subject's hands and feet are placed. 11,12 A low-voltage current (<4 V) is applied through the electrodes, attracting chloride ions from the sweat glands (which are densely concentrated on the palms and soles). A measurement of conductance for the hands and feet is generated from the derivative current associated with the applied voltage. 13 The aim of this study was to evaluate Sudoscan as a tool for assessing neuropathy in patients with DM, to examine the efficacy in detecting diabetic neuropathy (DN) in comparison with other standardized tests and to evaluate its role in discriminating painful from nonpainful neuropathy.
Subjects and Methods
The study population consisted of 83 patients with type 1 or 2 DM with and without DPN, diagnosed using the current Toronto classification of DPN. 1 Diabetes patients were compared with a database of 210 healthy controls (HCs) provided by Impeto Medical. Test–retest reliability was performed in 112 HCs. The study was approved by the Institutional Review Board of Eastern Virginia Medical School.
Sudomotor testing, quantitative sensory testing (QST), and quantitative autonomic function testing (QAFT) were performed on each participant. Complete physical and neurological examinations were done by a highly trained and skilled clinician.
Neuropathy measurements
All subjects received a complete neurological examination comprising six components: the neurological symptom score, cranial nerve function, and an evaluation of muscle weakness, muscular atrophy, bilateral reflexes, and sensory function of upper and lower extremities. Motor, Sensory, and Total Neuropathy Impairment Score—Lower Legs (NIS-LL) values, originally developed by Dyck 14 and modified by us, 15 were calculated for all patients.
QST was used to evaluate peripheral sensory perception. We used our previously published methods and algorithms for measuring small fiber somatosensory function, including vibration perception, pressure perception, cold and warm thermal sensation detection thresholds, and cold- and heat-induced pain detection thresholds at the big toes. 15 –17 For each of these stimuli we applied the method of limits: four trials with an interstimulus interval randomly varying from 4 to 20 s (model TSA 2001/VSA 3000; Medoc Advanced Medical, Minneapolis, MN). Thresholds were calculated as the mean stimulus intensity level over all four responses. Results are reported as δ from baseline, which is the difference between baseline and detection threshold temperature.
Symptomatic pain was recorded using a visual analog scale (11-point numerical rating scale), and pain sensitivity was determined using the Norfolk Pain Scale ratings using mechanical and cold pain perception.
QAFT was performed, as previously described. 18 Power spectral analysis of heart rate variability was assessed using ANSAR (ANX 3.0 software; ANSAR Group, Inc., Philadelphia, PA). Time- and frequency-domain analyses were performed. Time-domain analysis provides a measure of the sympathetic and parasympathetic control of the heart beat (the R-R interval on an electrocardiogram) recorded with maneuvers including deep breathing, Valsalva, and standing from the sitting position, whereas frequency-domain analysis is performed under resting conditions. 18 Given their complementary nature both were used in this study. Specifically, total spectral power is the average low frequency plus high frequency for each phase during baseline, deep breathing, Valsalva, and postural stimulations. The sample difference of the beat-to-beat (NN) intervals measures heart rate variability and has been shown to be significantly impaired in both recently diagnosed and established diabetes patients compared with HCs in prior studies. 19 The total spectral power was calculated, as well as the SD of all normal R-R intervals, a measure of both sympathetic and parasympathetic action on heart rate variability, and the root-mean square of the difference of successive R-R intervals, a measure primarily of parasympathetic activity. Baroreflex-mediated sympathoexcitation contributes to the development and progression of many cardiovascular disorders; thus, the quantitative estimation of the arterial baroreceptor-heart rate reflex is now regarded as a synthetic index of neural regulation at the sinus atrial node. 20 Low-frequency power, measured during power spectral analysis, was used to quantify baroreflex function. 21,22
Sudomotor function assessment
Sudoscan is a new patented device designed to perform precise evaluation of sweat gland function based on sweat chloride concentrations through reverse iontophoresis and chronoamperometry.
8
–10
The apparatus consists of two sets of large-area stainless steel electrodes for the hands and feet that are connected to a computer for recording and data-management purposes; the electrodes are alternately used as an anode or cathode, and a direct current incremental voltage of ≤4 V is applied to the anode. Through reverse iontophoresis, the device generates voltage to the cathode and a current (intensity of around 0.2 mA) between the anode and cathode proportional to chloride concentration. At low voltages (<10 V), the stratum corneum is electrically insulating, and only sweat-gland ducts are conductive (Supplementary Fig. S1; Supplementary Data are available online at
Statistical analysis
Continuous data are presented as mean±SEM values. Analysis of variance was used to compare mean differences between the groups. If significance was observed, post hoc analysis was performed (Tukey–Kramer test). Correlation was determined using Spearman's rho rank tests. Association between ESC and biological determinants (age, gender, body mass index, presence of DM, presence of neuropathy, etc.) was tested using multiple linear regression analysis. We constructed receiver-operator characteristic (ROC) curves to evaluate the sensitivity and specificity of Sudoscan in detecting DN compared with traditional modalities. We used the NIS-LL total score as the gold standard measure of the degree of neuropathy based on the cutoff values extracted from a large group of healthy subjects. JMP Pro 10.0 software (SAS Institute, Inc., Cary, NC) was used for all statistical analyses. Significance was accepted at the P<0.05 level.
Results
Eighty-three patients with DM were included in the study and compared with a database of 210 HCs provided by Impeto Medical. Demographic characteristics of both groups are presented in Supplementary Table S1. Twenty patients had type 1 DM, and 63 patients had type 2 DM. Sixty patients had neuropathy with a total neuropathy score of >2. HCs were not age and gender matched with DM patients because this database was provided by the sponsor. However, ESC values of feet and hands were not influenced by either age or gender on a multiple linear regression model (see below).
Sudoscan was accepted by the subjects without complaints; none of the subjects experienced discomfort during the test, and no safety events were reported.
ESC values of both feet and hands were significantly better in HC and DM patients without DN compared with DM patients with DN (Fig. 1 and Supplementary Table S2).
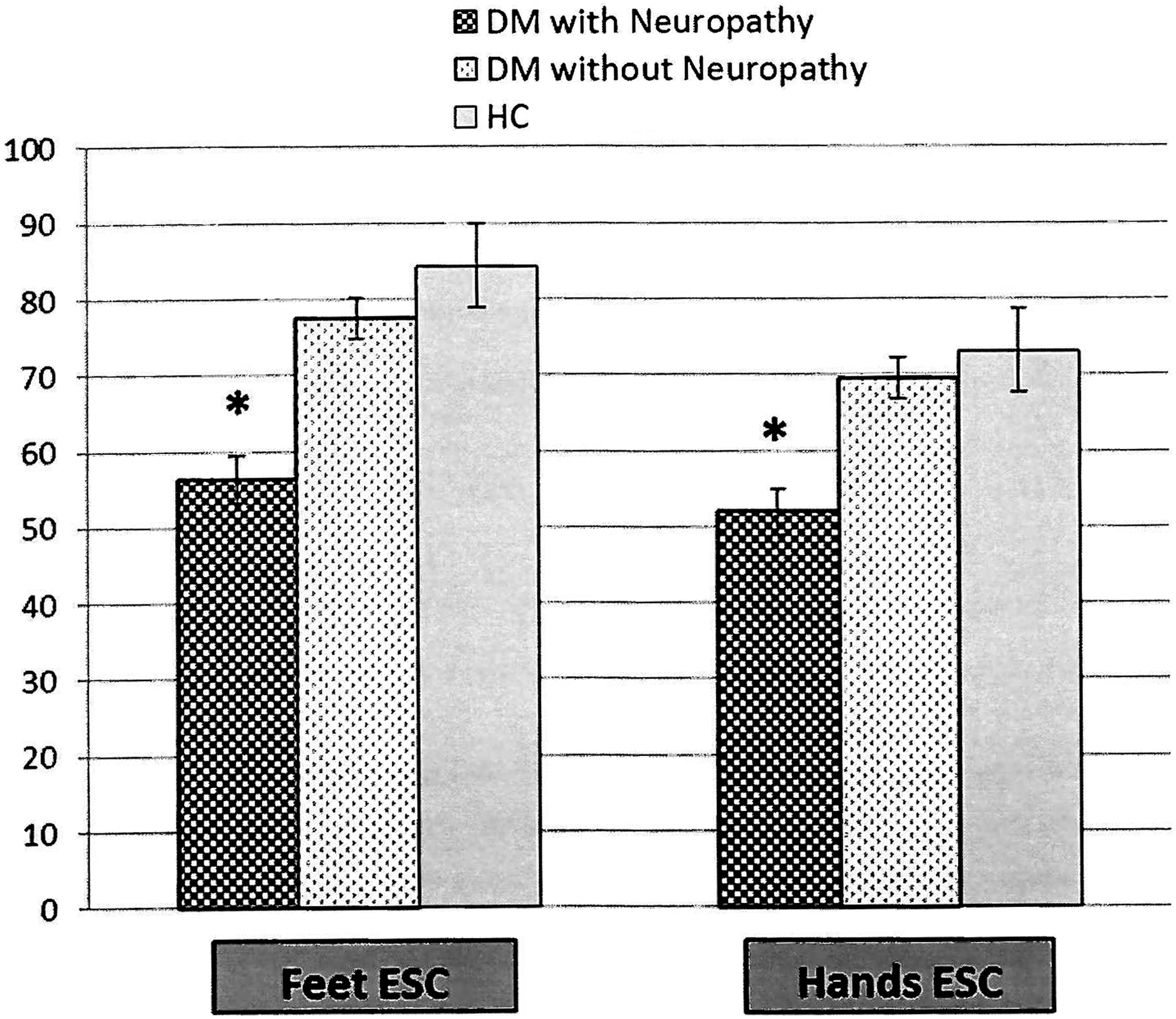
Feet and hands electrochemical skin conductance (ESC) in healthy control (HC) subjects and diabetes mellitus (DM) patients with and without diabetic neuropathy. Data are mean±SEM values. *P<0.0001 versus HC and DM without neuropathy (by analysis of variance with post hoc analysis).
DM patients with painful DN had significantly worse ESC of their feet than patients with nonpainful DN (52.8±3.6 vs. 68±6.6, P<0.05) (Supplementary Fig. S2).
Type 1 DM patients with neuropathy had feet and hands ESC values similar to those of type 2 DM patients with neuropathy (48.75±6.47 vs. 59.58±3.70 [P=not significant] for feet and 49.86±4.79 vs. 52.84±2.91 [P=not significant] for hands).
An association was detected between NIS-LL scores and ESC in the feet. Increasing NIS-LL scores were associated with decreasing ESC (Supplementary Fig. S3). An ESC of <60 μS was considered abnormal. Patients with abnormal feet ESC readings had significantly worse motor, sensory and total NIS-LL scores (Fig. 2).
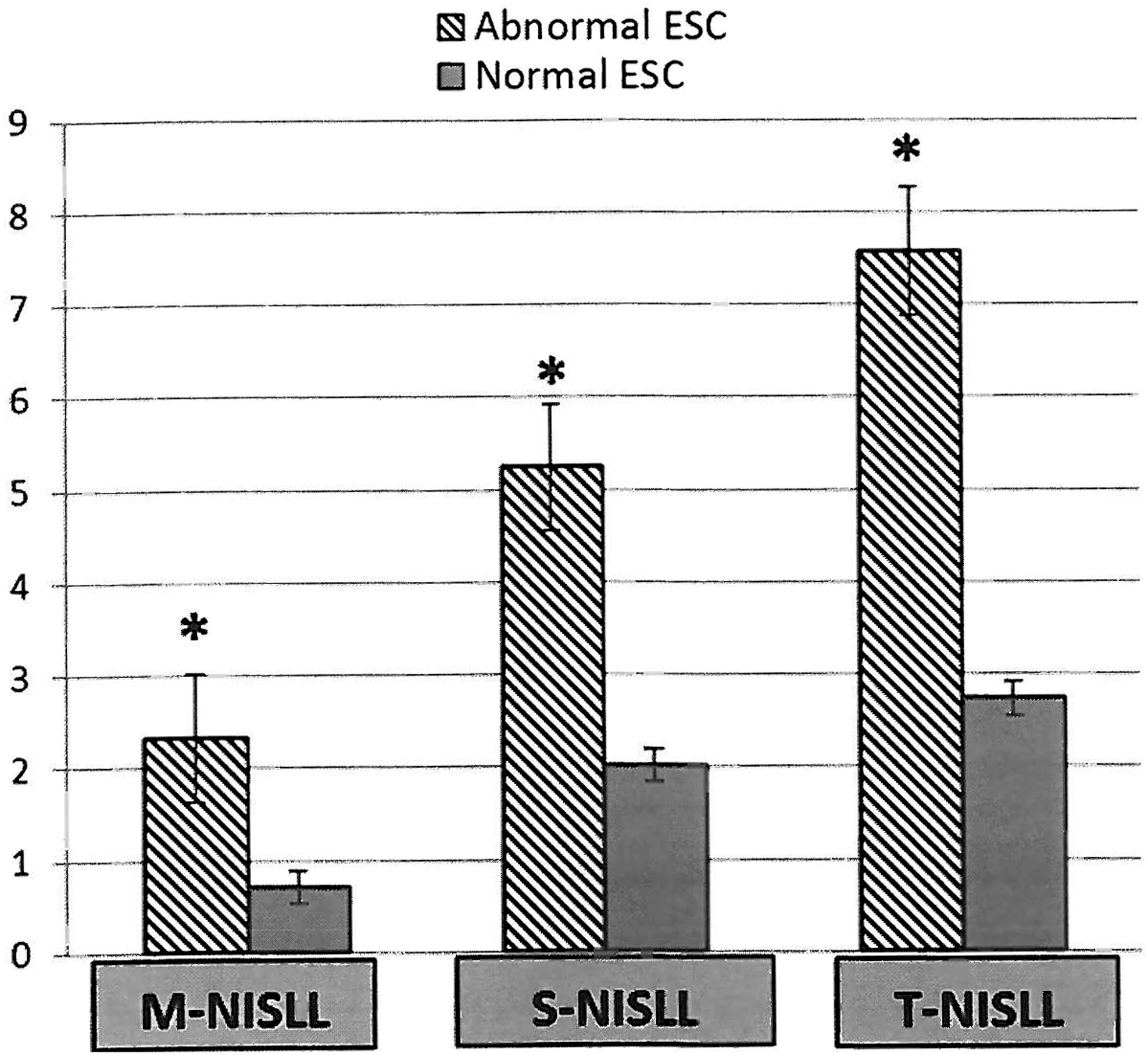
Motor, sensory, and total Neurologic Impairment Score—Lower Legs M-NISLL, S-NISLL, and T-NISLL, respectively; scores in patients with normal (≥60 μS) versus abnormal (<60 μS) electrochemical skin conductance (ESC) of the feet. Data are mean±SEM data. *P<0.0001 by analysis of variance.
ESCs correlated significantly with clinical (NIS-LL), somatic (QST), and autonomic (QAFT) measures of neuropathy and with pain scores (Table 1).
Data are log transformed.
CP, cold pain; CS, cold sensation; DB, deep breathing; DN, diabetic neuropathy; E/I ratio, expiration/inspiration ratio; ESC, electrochemical skin conductance; LFA, low-frequency band; NIS-LL, Neurologic Impairment Score—Lower Legs; QST, quantitative sensory testing; RFA, high-frequency band; sdNN, sample difference of the beat-to-beat (NN) variability; TSP, total spectral power; Val, Valsalva; WS, warm sensation.
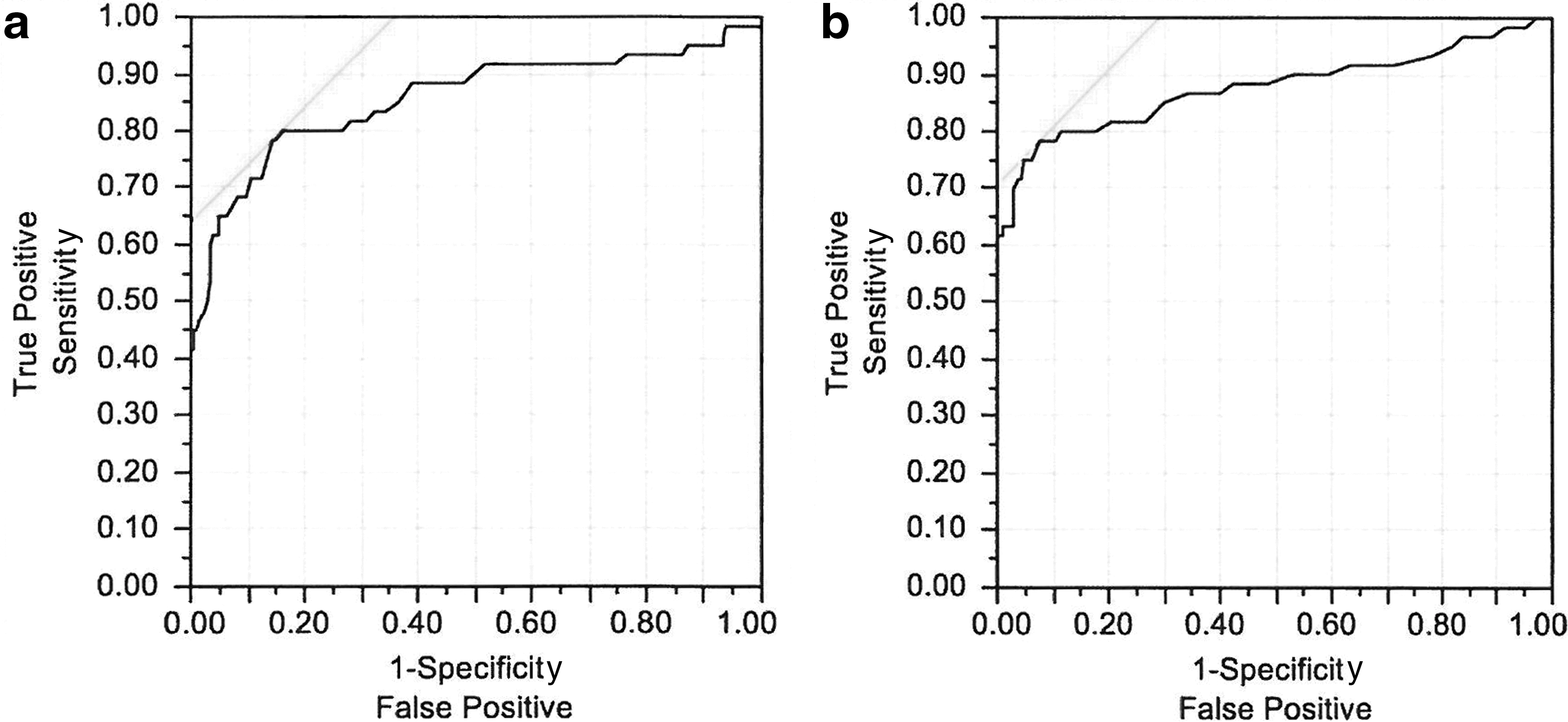
On multiple linear regression analysis, lower feet ESC was independently associated with higher NIS-LL total scores (P<0.001) and with the presence of neuropathy (P<0.05) but not with age, gender, or body mass index. ROC curve analysis, used to evaluate sensitivity and specificity of Sudoscan in detecting DN showed significant results for both hands and feet ESC (area under the curve of 0.86 and 0.88, respectively; P<0.0001) with sensitivity of 78% and specificity of 92% for feet. The NIS-LL total score showed an area under the curve of 0.8429 with sensitivity of 76% and specificity of 86% (Table 2 and Fig. 3).
Electrochemical skin conductance of
Criterion corresponding to the highest Youden index.
ESC, electrochemical skin conductance; +LR, positive likelihood ratio; –LR, negative likelihood ratio; NIS-LL, Neurologic Impairment Score—Lower Legs; +PV, positive predictive value; −PV, negative predictive value.
Test–retest reliability in 112 HCs was excellent for the feet with a correlation coefficient of 0.814 (P<0.0001) and a mean percentage change of 1.15% after the maximum O2 intake volume (VO2 max) test (Supplementary Fig. S4). Association between left and right side measurements of ESC in feet and hands in 210 HCs was excellent. The mean percentage difference between measurements on the right and left side was 0.8% for hands and 0.15% for feet, with correlation coefficients of 0.91 and 0.93, respectively (P<0.0001) (Supplementary Fig. S5).
Discussion
This study shows that: 1. ESC of hands and feet is decreased in patients with DN diagnosed using the current Toronto classification of DPN,
1
compared with HCs and DM patients without neuropathy. 2. Sudoscan results correlate significantly with clinical measures of neuropathy, somatic and autonomic function testing, and pain scores. 3. Sudoscan is a sensitive tool to detect neuropathy in patients with DM, with a sensitivity of 78% and a specificity of 92%, equivalent to or better than clinical neuropathy scores. 4. Feet ESC was significantly decreased in patients with painful DN compared with the value in patients with nonpainful neuropathy. 5. Test–retest reliability is excellent for the feet.
These results suggest that sudomotor function, evaluated through reverse iontophoresis (Sudoscan), is a reliable option when evaluating diabetes patients for the detection of small fiber neuropathy and peripheral autonomic neuropathy. Combined with a simple bedside test as the NIS-LL, Sudoscan may increase the effectiveness in detecting neuropathy. Dyck et al. 24 have shown significant inconsistencies on clinical neurological evaluations performed by different blinded physicians; the advantage of incorporating Sudoscan for the detection of neuropathy is that it eliminates the subjective component of the clinician error.
Several studies have evaluated the efficacy and reproducibility of Sudoscan in detecting DN during the past 2–3 years. Yajnik et al. 25 evaluated different neuropathy assessments on 265 diabetes patients and found that ESC measurements between the left and right side varied by 9.5% for hands and 6.0% for feet, compared with 14.2% for the vibration perception threshold test. Lower measures of ESC were significantly associated with increasing symptoms on the Michigan Neuropathy Scoring Instrument A, which evaluates the presence of small and large fiber neuropathy symptoms; increasing physical abnormalities on the Michigan Neuropathy Scoring Instrument B, which includes feet inspection, vibration perception, ankle reflexes, and monofilament perception; and increasing scores on the vibration perception threshold test, reflecting impaired vibration perception. Patients with an ESC of <40 μS were more than four times as likely as patients with an ESC of ≥40 μS to have two or more abnormal cardiac autonomic neuropathy tests with an odds ratio of 4.41 (95% confidence interval, 1.72–11.29). Of note is that 40 μS is a much lower value than what is defined as the normal cutoff value. Lower ESC was specifically associated with postural fall in blood pressure, a measure of sympathetic cardiac autonomic neuropathy. 25
Mayaudon et al. 8 measured sensitivity, specificity, and reproducibility of Sudoscan among 133 type 2 DM patients compared with 41 HCs. ESC showed a sensitivity of 75% and a specificity of 100%, with an area under the ROC curve of 0.88, similar to our current report. These researchers also showed low coefficients of variation between the left and right on both hands and feet measurements (15% and 7%, respectively). A similar study among 142 French diabetes patients showed that reduction in foot ESC measurements from 66±17 μS to 43±39 μS correlated with an increasing vibration perception threshold from <15V to >25V (P=0.001), regardless of blood glucose levels. 9 Another study on type 1 and type 2 DM patients from an outpatient clinic in Germany was conducted parallel to standard care. Fifty-two patients with type 1 DM and 115 patients with type 2 DM (69 receiving insulin) were observed for 1 year. Hand and foot conductances were lower in patients with type 2 DM compared with patients with type 1 DM at baseline. After 1 year, a slight decrease in hand and foot ESC was observed in patients with type 2 DM without insulin, whereas an increase was observed in patients receiving insulin (−3.8±9.7 vs. 1.0±9.7 μS [P=0.02] for the hands and −2.2±7.5 vs. 4.1±8.8 μS [P<0.001] for the feet). The question remains as to whether this improvement is related to better glycemic control or is an effect of insulin per se on nerve conduction or ion transport. Coefficient of correlation between measurements performed with two different devices was 0.85 for hands and 0.93 for feet (P<0.001). 23
Beyond its potential for diabetes screening, Sudoscan may play an important role in following patients' response to clinical intervention or investigational therapies. A large study was recently completed in Finland using Sudoscan to assess cardiometabolic disease risk status and its change in response to lifestyle intervention. Of 537 women and 113 men who underwent a cardiovascular risk evaluation and ESC measurement at baseline, those with the highest cardiovascular risk were invited to participate in a 12-month physical activity program. For the 154 women with the lowest fitness level at baseline, a statistically significant change in waist circumference, weight, body fat percentage, VO2 max, and hands and feet ESC was observed after 1 year. The increase in VO2 max and ESC were highest in subjects with the highest weekly activity level. Correlation between Sudoscan risk score and VO2 max was r=−0.57, P<0.0001 for women and r=−0.48, P<0.0001 for men. 26 Although larger studies that include more men are required to confirm these results, the outcome of this study suggests not only that lifestyle intervention using moderate physical activity can have a significant impact on cardiovascular risk, but also that a simple tool like Sudoscan can be used in interventional programs to assess and monitor changes in cardiovascular risk.
Our results are in accordance with those of others, as discussed above. Moreover, in our study we found a significant correlation between ESC and pain scores, with feet ESC being significantly decreased in patients with painful DN compared with patients with nonpainful neuropathy. Although the number of patients included was small, these observations warrant further study.
Several reliable and validated techniques of sudomotor function testing are currently available. 6 However, most are actually underutilized in the clinical setting. This is owing, in part, to requirements of very specialized equipment, complicated patient preparation, highly trained technicians for test performance and/or interpretation, and prolonged testing time. Sudoscan appears to address all these shortcomings. 7
In conclusion, Sudoscan is a promising, sensitive tool to detect neuropathy in patients with DM. Sudoscan testing is entirely painless, can be conducted in 3 min, and requires no special patient or equipment preparation. Test administration and result interpretation also demand no special training. It is objective, reproducible, and quantitative, requiring no patient cooperation. Further larger studies including different age groups and ethnic populations are needed to confirm these findings, as well as interventional studies to assess the utility of this tool as an objective measure of small fiber neuropathy and peripheral autonomic dysfunction. Sudoscan may become an invaluable tool for today's clinicians, whether the potential applications are screening for early diagnosis of DN, assessing response to different therapeutic interventions in diabetes subjects, or even as a predictive tool for the development of insulin resistance and diabetes.
Footnotes
Acknowledgments
This research study was supported by a grant from Impeto Medical.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.