
Abstract
Capsule Summary
First characterization of intrinsic and extrinsic atopic subtypes in CSU: Established first diagnostic framework for intrinsic (non-IgE-mediated) and extrinsic (IgE-mediated) atopic subtypes in CSU using comprehensive criteria (IgE levels, allergy history, clinical signs).
Atopy predicts superior omalizumab response: Both intrinsic (95.1%) and extrinsic (97.2%) atopic CSU patients showed significantly better response to omalizumab versus non-atopic patients (77.8%, p < 0.001).
Intrinsic atopy: A paradoxical responder Despite lacking IgE abnormalities, intrinsic atopic patients demonstrated near-identical high response rates to anti-IgE therapy, warranting mechanistic investigation.
INTRODUCTION
Chronic spontaneous urticaria (CSU) is a common condition marked by recurrent, itchy wheals and/or angioedema lasting over 6 weeks. 1 The latest nationwide epidemiological survey reports a prevalence of 1.29% in China, making CSU one of the most frequent dermatological diseases. 2 Its prolonged and unpredictable course significantly impacts patients’ quality of life and mental health. According to the international EAACI/GA2LEN/EuroGuiDerm/APAAACI urticaria guideline, 1 second-generation nonsedating H1 antihistamine is the first-line treatment for CSU. However, studies show that standard dose antihistamines achieve complete symptom control in less than half of patients, and even with up to four times the standard dose, 10–50% of patients remain poorly controlled.3,4 Due to its proven efficacy and safety in antihistamine-refractory CSU, omalizumab is now considered the optimal treatment option.5,6 Identifying clinical characteristics associated with different responses to omalizumab, or predicting treatment outcomes, is crucial for enhancing clinical management efficiency.
Atopy is a predisposition to immunological responses to allergens, leading to type 2 inflammation and immunoglobulin E (IgE) overproduction. 7 The relationship between atopy and CSU has not been fully appreciated. 8 Previous studies showed that the CSU patient population exhibits a more pronounced atopic background compared to the normal population, 9 and CSU patients with atopy have relatively unique clinical characteristics. 10 Although previous studies have suggested a potential association between atopy and the treatment response to omalizumab for CSU, the conclusions have not been consistent due to the different criteria used for assessing atopy in various studies and the relatively small sample sizes.11-13
Historically, the nomenclature of extrinsic versus intrinsic was first applied to asthma (AS) in 1947. In atopic diseases such as atopic dermatitis (AD) and AS, the concepts of intrinsic and extrinsic atopy have been extensively discussed and validated.14,15 It is currently believed that extrinsic atopy is mediated by IgE, leading to type 2 inflammation, while intrinsic atopy is mediated through non-IgE pathways to induce type 2 inflammation. Therefore, the distinction between the two primarily depends on whether allergen-specific IgE (sIgE) is detected and whether the total IgE (tIgE) level is elevated. 16 Clinical observations have revealed that atopy in patients with CSU also exhibits both intrinsic and extrinsic subtypes, the clinical associations of which with CSU have not yet been fully explored. Our study aimed to investigate the clinical value of identifying and differentiating atopic subtypes of CSU patients in predicting the treatment response to omalizumab, and to compare the clinical characteristics and relevant laboratory indicators between CSU patients with different atopic backgrounds.
MATERIALS AND METHODS
Patients
This was an investigator-initiated, single-center, retrospective, observational study conducted at the Urticaria Reference and Excellence Center (UCARE), reviewing and analyzing the patients with CSU who were treated with omalizumab from January 2023 to December 2024. CSU was diagnosed and assessed according to the international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline. 1 All patients included in the analysis had received at least three injections of omalizumab and had detailed symptom assessment records, allowing for clear identification of treatment response and onset of efficacy. Additionally, any omalizumab-related adverse effects experienced by the patients during the treatment period were accurately documented.
Confirmation of Atopy and Subtypes of Atopy
All patients included in the analysis underwent a comprehensive and meticulous evaluation to confirm atopy. This included detailed documentation of personal allergic history and family allergic history. Allergic history encompassed conditions such as allergic rhinitis, AS, allergic conjunctivitis, AD/eczema, and confirmed food allergies. Family allergic history focused on first-degree relatives, including parents, grandparents, siblings, and children. Additionally, all patients should have been tested for sIgE (including 29 common inhalant and food allergens) and tIgE levels. Atopic signs, as assessed and confirmed by a board-certified dermatologist, were also recorded. Atopic signs refer to characteristic skin manifestations that may indicate atopy, with detailed descriptions provided in Supplementary Table S1 and Supplementary Figure S1. These signs were primarily referenced from the diagnostic criteria for AD established by Hanifin and Rajka. 17
The criteria for determining atopy include the following five items (as shown in Supplementary Fig. S2): (a) positive sIgE to at least two allergens (grade 1 or above), or at least one allergen at grade 2 or above; (b) tIgE level >165 IU/mL; (c) a clear personal history of allergies; (d) a clear family history of allergies; and (e) presence of at least two atopic manifestations. If a patient meets at least two of these five criteria, they were confirmed to have atopy. Furthermore, patients with confirmed atopy were further classified as “extrinsic atopy” if they tested positive for either item 1 or 2. Conversely, patients with confirmed atopy but negative results for both items 1 and 2 were classified as “intrinsic atopy.” The classification of atopy into intrinsic and extrinsic subtypes was based on established criteria from previous studies.14-16,18,19
Omalizumab Treatment and Treatment Response Evaluation
All patients in the study had failed at least 4 weeks of second-generation antihistamine treatment (at standard or up to 4-fold doses) as per international urticaria guidelines before starting omalizumab therapy. 1 They received a standard dose of 300 mg of omalizumab every 4 weeks for at least 3 months, followed by a minimum 3-month follow-up, regardless of maintenance injections. At our center, all CSU patients were provided with a urticaria activity score (UAS) diary for daily self-assessment after proper training. During monthly follow-ups, the urticaria control test (UCT) and dermatology life quality index (DLQI) were also assessed. Response to omalizumab was evaluated using the UAS7 score in the first 16 weeks of treatment and categorized as: responders (complete: UAS7 = 0; good: UAS7 = 1–6), partial responders (UAS7 = 7–15), and nonresponders (UAS7 > 15). 20 For responders, the onset speed of omalizumab was determined by the time from the first injection to symptom control (UAS= 0 or 1, with sustained stability and UAS7 ≤ 6). Those achieving a complete or good response (UAS7 ≤ 6) within 1 month were classified as “fast responders,” while those achieving it after 1 month were “slow responders.”
Statistical Analysis
Statistical analyses were performed using SPSS software (version 26.0; IBM Corp, Armonk, NY, USA). Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed data are presented as mean ± standard deviation (SD) and analyzed using one-way analysis of variance (ANOVA) with post hoc Tukey tests for intergroup comparisons. Non-normally distributed data are expressed as median (interquartile range, IQR) and analyzed using the Kruskal–Wallis H test or Mann–Whitney U test, as appropriate. Categorical variables are reported as frequencies (percentages) and compared using Pearson’s χ2 test or Fisher’s exact test for small sample sizes. Pairwise comparisons were adjusted using the Bonferroni correction. To investigate the independent predictors of omalizumab response, multifactorial logistic regression analysis was performed on those variables with P < 0.10 in the univariate analysis. Odds ratios (ORs) and 95% confidence intervals (CIs) were reported. The threshold for statistical significance was set at P < 0.05 (two-tailed).
RESULTS
General and Atopic Features of the Patients
The study included 210 CSU patients (mean age 40.9 ± 14.4 years; 62.4% female) with a median disease duration of 28.9 months. Concomitant angioedema and chronic inducible urticaria (CIndU) occurred in 41.8% and 44.8%, respectively. Personal/family urticaria history was reported in 22.9%/19.0%. Baseline severity scores: UAS7 (27.1 ± 7.6), UCT (3.4 ± 3.1), and DLQI (18.3 ± 7.1). Atopy prevalence was 70.0% (extrinsic: 50.5%, intrinsic: 19.5%) (Table 1). Atopic features of the patients showed extrinsic atopic patients had the highest median tIgE (244.0 kU/L) versus overall baseline (83.6 kU/L). Elevated tIgE occurred in 33.3% of all patients (56.6% extrinsic). sIgE positivity (60% overall) was predominantly extrinsic. Only one nonatopic CSU patient had a positive sIgE result for dust mites, but lacked additional criteria to confirm atopy. Personal allergy history was highest in intrinsic (65.9%) and extrinsic (42.5%) groups versus nonatopic (11.1%), with familial allergies following similar trends (extrinsic: 47.2%, intrinsic: 43.9%, nonatopic: 6.3%). Atopic signs were prevalent in 53.3% of patients (extrinsic: 67.0%, intrinsic: 75.6%), but minimal in nonatopic patients (15.8%) (Table 2).
Demographic and Clinical Characterization of Patients
BMI, body mass index; CIndU, chronic induced urticaria; CSU, chronic spontaneous urticaria; DLQI, dermatology life quality index; UAS7, urticaria activity score over 7 days; UCT, urticaria control test.
Atopic Characteristics of the Patients with CSU
IgE, Immunoglobulin E; sIgE, specific Immunoglobulin E; tIgE, total Immunoglobulin E.
Characteristics of CSU with Diverse Atopic Backgrounds
Demographic and clinical characteristics (Table 3) revealed that nonatopic CSU patients were older (45.3 ± 15.5 years) versus extrinsic (39.0 ± 13.0) and intrinsic (39.3 ± 15.0) groups (P = 0.027). Extrinsic atopic patients had higher rates of past urticaria (33.0% vs nonatopic 15.8%, P = 0.044) and family urticaria history (21.7% vs nonatopic 6.3%, P = 0.003). Annular/semi-annular wheals were less frequent in nonatopic (5.7%) versus extrinsic (21.2%) and intrinsic (18.4%) groups (P = 0.044), while red plaques dominated in nonatopic patients (83.0% vs 55.6–50.0%, P < 0.001). Sex, BMI, disease duration, angioedema, and baseline scores (UAS7/UCT/DLQI) showed no intergroup differences. Combined CIndU subtypes had comparable frequencies.
Demographic and Clinical Characteristics of the Patients with Different Atopic Background
* Chi-squared test. ** One-way ANOVA. *** Kruskal–Wallis test.
a , b , c , dStatistical results between pairs are indicated by letters, with the same letters indicating no statistical difference between the two groups and different letters indicating a statistical difference between the two groups. Comparisons among multiple groups were corrected for significance by Bonferroni method.
Bold values indicate statistical significance (P < 0.05).
Laboratory Biomarkers Across Atopic Subgroups in CSU
Laboratory findings (Table 4) revealed higher IgG-anti-TM positivity in nonatopic CSU patients (20.8%) versus extrinsic (2.0%) and intrinsic atopic (9.5%) groups (P = 0.022), with significant extrinsic versus nonatopic differences. No significant variations were observed in autologous serum skin test (ASST) positivity, thyroid autoantibodies (anti-TG/TPO),
Clinical Laboratory Test Results of the Patients with Different Atopic Background
* Chi-squared test. ** Kruskal–Wallis test.
a,b,c,dStatistical results between pairs are indicated by letters, with the same letters indicating no statistical difference between the two groups and different letters indicating a statistical difference between the two groups. Comparisons among multiple groups were corrected for significance by Bonferroni method.
ASST, autologous serum skin test; IgG, Immunoglobulin G; TG, thyroglobulin; TPO, thyroid peroxidase; TM, thyroid microsome; ANA, antinuclear antibody; CRP, C-reactive protein; C3, Complement 3; C4, Complement 4; IQR, interquartile range; Eos, eosinophil; Bas, Basophil; Neu, neutrophil; Lym, lymphocyte; Mono, monocyte.
Bold values indicate statistical significance (P < 0.05).
Omalizumab Response and Safety Profiles Across Atopic Subtypes
The multivariate logistic regression analysis (Table 5) identified angioedema (OR = 16.19, CI: 1.81–144.67, P = 0.013) and positive ASST (OR = 16.44, CI: 1.85–146.36, P = 0.012) were independently associated with poor-response of omalizumab, only atopy (OR = 9.42, CI: 2.17–40.96, P = 0.003) was independently associated with well-response. As shown in Table 6, omalizumab response rates significantly differed across atopic subgroups (P < 0.001), with nonatopic patients showing lower efficacy (77.8%) versus extrinsic (97.2%) and intrinsic (95.1%) groups. Nonresponders were more prevalent in the nonatopic cohort (12.7%) than in the extrinsic (0.0%) and intrinsic atopic (2.4%) groups (P < 0.001). Nonatopic patients achieved rapid symptom relief within 24 hours more frequently (28.6%) than extrinsic (9.7%) and intrinsic atopic (20.5%) groups (P = 0.012), while responses within 1–7 days were less common in nonatopic patients (P = 0.054). Both extrinsic atopic patients (18.9%) and intrinsic atopic patients (22.0%) reported significantly higher overall side effect rates than nonatopic patients (4.8%) (P = 0.020). Flare-ups of urticaria were more frequent in atopic subgroups (extrinsic: 8.5%, intrinsic: 9.7%) compared to nonatopic patients (0, P = 0.049). Injection site reactions showed no intergroup differences.
Multivariate Logistic Regression Analyses of Patient Characteristics Associated with Well-Responders in Comparison to Poor-Responders of Omalizumab
Hosmer–Lemeshow: 0.246, Nagelkerke R square: 0.566.
Bold values indicate statistical significance (P < 0.05).
CI, confidence interval; OR, odds ratio; SD, standard deviation; Y/N, Yes versus No.
Omalizumab Response Characteristics of the Patients with Different Atopic Background
Chi-squared test.
a,b,c,dStatistical results between pairs are indicated by letters, with the same letters indicating no statistical difference between the two groups and different letters indicating a statistical difference between the two groups. Comparisons among multiple groups were corrected for significance by Bonferroni method.
Bold values indicate statistical significance (P < 0.05).
OMA, omalizumab.
Impact of Total IgE and Atopic Subtypes on Omalizumab Response
Omalizumab response rates varied by tIgE levels and atopic status (Fig. 1). Intrinsic atopic CSU patients showed the highest response (100%) in the tIgE >100 IU/ml subgroup, followed by extrinsic (97%) and nonatopic (90%) groups. For 40–100 IU/ml, both atopic subtypes achieved 100% response, versus 76.9% in nonatopic patients. In tIgE <40 IU/ml, nonatopic patients had the lowest efficacy (70%) compared with extrinsic (87.5%) and intrinsic (83.3%) cohorts. Regarding response speed (Fig. 2), >90% of responders were rapid overall. However, extrinsic atopic CSU patients exhibited slightly lower rapid response proportions across tIgE subgroups compared with intrinsic and nonatopic groups.

Omalizumab response rates categorized by atopic subtype and tIgE levels. Well-responders: patients achieving complete (UAS7 = 0) or good response (UAS7 = 1–6). Poor-responders: patients with partial (UAS7 = 7–15) or no response (UAS7 > 15). Response rates are stratified by tIgE thresholds (<40 IU/mL, 40–100 IU/mL, >100 IU/mL). tIgE, total Immunoglobulin E; UAS, urticaria activity score.
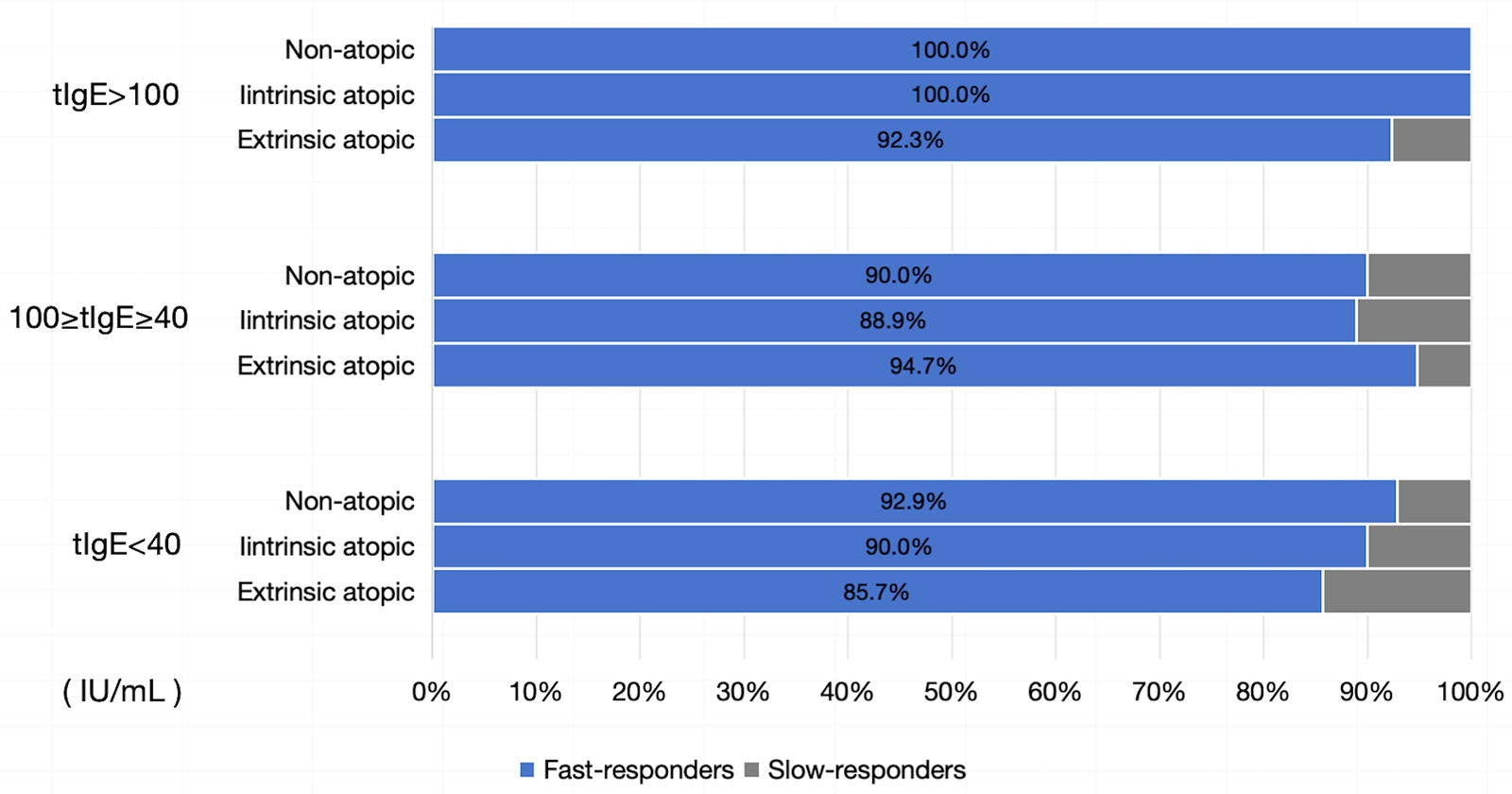
Speed of omalizumab response categorized by atopic subtype and tIgE levels. Fast responders: patients achieving complete/good response (UAS7 ≤ 6) within 1 month. Slow responders: patients requiring >1 month to achieve a response. tIgE: total immunoglobulin E. Subgroups are stratified by tIgE thresholds (<40 IU/mL, 40–100 IU/mL, >100 IU/mL).
DISCUSSION
The concept of atopy, introduced by Coca and Cooke in 1923, 21 lacks a universally accepted diagnostic criterion. While atopy is often defined by positive IgE tests in previous research, 22 many patients with typical allergic manifestations or a strong personal/family history of allergic diseases lack positive IgE results. 23 These intrinsic atopic patients are frequently overlooked. Although intrinsic atopy has been described in conditions like AD, 24 AS, 15 and allergic rhinitis, 23 its characterization in CSU remains unexplored. Our study is the first to identify and differentiate extrinsic and intrinsic atopy in CSU patients, focusing on their clinical characteristics and responses to omalizumab.
Previous studies on CSU primarily defined atopy based on allergen-specific IgE positivity, leading to variability in reported atopy prevalence.8,13,25,26 Our study prioritized a holistic evaluation of patients’ atopy by integrating multiple atopic features or clinical indicators, rather than isolating individual signs or biomarkers, to comprehensively characterize the influence of atopy on omalizumab responses. In our study, 70% of CSU patients exhibited atopy, with extrinsic atopy being predominant and intrinsic atopy comprising nearly 30%. Intrinsic atopic patients were predominantly female (68.3%), consistent with findings in intrinsic AD. 16 Atopic signs, often overlooked in CSU but well documented in AD, 27 were present in over half of our CSU cohort, highlighting their diagnostic value. Nonatopic CSU patients were significantly older than atopic patients, particularly those with extrinsic atopy, aligning with findings by Costa et al. 13 that atopy is a risk factor for earlier-onset CSU. Atopic CSU patients, especially those with extrinsic atopy, more frequently reported a personal and familial history of urticaria, suggesting that atopy is an important genetic predisposition for urticaria. 10
Clinically, CSU patients exhibit distinct wheal morphologies: annular/semi-annular, 28 red plaques/patches, and white plaques/patches. Most patients present with one dominant type or a mixed pattern. Interestingly, our study revealed divergent distributions across atopic subgroups: annular/semi-annular wheals were more common in extrinsic atopic CSU, while red plaques/patches predominated in nonatopic CSU. The clinical and mechanistic implications of these findings warrant further investigation.
A positive ASST often indicates autoreactivity in CSU patients, akin to atopy but considered its opposite. 29 This study found no difference in ASST positivity rates among CSU patients with different atopic subtypes, suggesting autoreactivity and atopy are independent traits. However, in terms of the response to omalizumab, we found that ASST positivity and atopy acted as completely opposite independent predictors. This intriguing phenomenon warrants further investigation. IgG-anti-TM positivity was significantly higher in nonatopic CSU patients than in extrinsic atopic CSU patients, indicating a potential autoimmune predisposition in nonatopic CSU. We did not find any differences in other clinical test parameters among CSU patients with different atopic subtypes, suggesting no significant differences in inflammatory activity across atopic subgroups.
Regarding the treatment response to omalizumab, the overall response rate of our patients reached 91.0%, which is consistent with previous findings based on Chinese populations.5,6,30 Interestingly, when analyzing the response in CSU patients with different atopic subtypes, we found that nonatopic CSU had a response rate of only 77.8%, significantly lower than endogenous CSU (95.1%) and extrinsic atopic CSU (97.2%). The nonresponders were predominantly nonatopic patients. The multivariate analysis also identified atopy as a significant independent predictor of a favorable response to omalizumab. This suggests that atopy is closely linked to omalizumab response. Previous studies on whether atopy affects omalizumab response have been controversial. Atopy is often associated with elevated tIgE, which has been shown to predict a better response to omalizumab. 31 Thus, it would make sense that atopic patients respond better. However, studies by Foti et al., 11 Costa et al., 13 and Asero et al. 32 found no such association. Upon further analysis, these studies used limited criteria to define atopy. For instance, Foti et al. relied on documented atopic history, while the others used only sIgE or skin prick test (SPT) results. These narrow definitions likely failed to identify all atopic patients, particularly those with intrinsic atopy, who were misclassified as nonatopic. This could explain why their findings did not support a correlation between atopy and improved omalizumab response. Another study suggested that patients with atopy had a better treatment response to omalizumab, but the definition of atopy in that study was also based solely on positive SPT/sIgE results. 33
Due to the absence of positive sIgE and normal total IgE levels, patients with intrinsic atopy are often mistakenly classified as nonatopic. 23 However, they typically have a clear atopic history or strong atopic signs, allowing us to identify them more accurately using our criteria. The favorable response in intrinsic atopic CSU, despite the absence of IgE elevation, suggests potential noncanonical mechanisms. Omalizumab may modulate IgE-independent pathways, such as reducing free IgE’s pro-inflammatory effects on mast cells or inhibiting FcεRI expression. Alternatively, intrinsic atopy may involve unrecognized IgE autoantibodies or localized IgE production not captured by systemic assays. Further mechanistic studies are warranted to explore these possibilities.
The overall onset speed of omalizumab response did not significantly differ among CSU patients with different atopic subtypes. However, a higher proportion of nonatopic patients responded within 24 hours compared to extrinsic atopic patients. This may be due to their lower total IgE levels, enabling faster blockade with the same omalizumab dose, as supported by the observation that intrinsic atopic patients also showed a higher 24-hour response rate.
Omalizumab is generally safe, with few patients experiencing injection site reactions, urticaria flare-up postinjection, or rare adverse effects like headache and fatigue. 34 Our study found that nonatopic CSU patients had fewer adverse reactions than atopic patients. Notably, all urticaria flare-ups postinjection occurred in atopic patients, with no difference between intrinsic and extrinsic atopy. Injection site reactions (mostly pruritic wheals or edema) were also more common in atopic patients, though not statistically significant, warranting further validation. This difference may be due to the murine antigenic components in omalizumab, 35 which could more readily trigger allergic responses in atopic individuals.
Previous studies show that CSU patients with low (<40 IU/mL) or high (>100 IU/mL) tIgE levels respond differently to omalizumab.36,37 Grouping patients by tIgE, we found that all atopic subtypes in the low tIgE group had reduced response rates, and most atopic patients with poor responses had tIgE <40 IU/mL. In contrast, when tIgE >100 IU/mL, nonatopic patients reached a 90% response rate. This suggests combining atopy status with tIgE levels may improve prediction of omalizumab response, but larger studies are needed for confirmation.
While our findings are robust, the single-center and retrospective design may introduce selection bias, particularly in patient recruitment and management protocols. Future multicenter studies are needed to validate these results across diverse populations.
In summary, this study, for the first time, describes the presence of both intrinsic and extrinsic atopy in CSU patients using a more comprehensive atopy assessment criterion. The findings showed that atopy is associated with clinical characteristics and omalizumab treatment responses in CSU patients. Both intrinsic and extrinsic atopic CSU patients demonstrated significantly better responses to omalizumab compared to nonatopic CSU patients. Intrinsic atopic CSU, a previously overlooked subgroup, warrants further investigation. We strongly advocate for larger-scale studies in the future to focus on this subtype, providing more evidence for the classification and treatment of the disease.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.