
Abstract
Capsule Summary
The study evaluates the clinical efficacy of Abrocitinib, a JAK inhibitor, in treating moderate-to-severe AD, highlighting its effectiveness in reducing inflammation and improving skin lesions through a biomarker-driven approach. Significant biomarkers such as S100A7, KRT16, and IL-33 are identified, showing correlations with disease severity and treatment response, which could aid in personalized treatment strategies for AD.
INTRODUCTION
Atopic dermatitis (AD) is known as a common chronic inflammatory skin condition with severe itching, often combined with other atopic conditions, including allergic asthma and allergic rhinitis. 1 The pathogenesis of AD typically involves immune dysfunction and epithelial barrier damage.2,3 While skin biopsies were commonly used in previous studies to detect biomarker changes in the skin, they risk wound pain, infection, and scarring. 4 Blood biomarkers are more easily collected and provide a more comprehensive representation of systemic inflammation than biopsy specimens. However, in patients with mild AD, systemic inflammation is often minimal, making significant blood biomarker detection challenging. 5
Tape-stripping is a minimally invasive technique of sampling the upper epidermis by repeatedly applying adhesive tape to the skin surface6,7 and is used to characterize pediatric and adult AD by analyzing transcriptomics, proteomics, lipidomics, and microbiomes.8B9 -12 Recently, tape-stripping has been employed to detect RNA and protein biomarkers from lesional and nonlesional skin of patients with AD, enabling tracking of disease severity and response to dupilumab therapy.8,13
Patients with AD can be classified into 2 groups—extrinsic and intrinsic AD—based on the presence of allergen-specific IgE and total serum IgE concentrations. Extrinsic AD accounts for approximately 63%−80% of all AD cases14,15 and is characterized by elevated serum IgE levels, the presence of ingested or inhaled allergens, and a personal or family history of atopic diseases, in contrast to intrinsic AD. Research has shown that patients with both subtypes respond equally well to dupilumab treatment. 16 To date, there have been no comparative studies on the serum inflammatory characteristics in extrinsic and intrinsic AD. Furthermore, it remains unclear whether abrocitinib is effective for both subtypes.
Abrocitinib specifically targets Janus kinase 1 (JAK1), making it a targeted approach to reducing the inflammation and immune dysregulation underlying AD. 17 In real-world settings, abrocitinib has demonstrated significant efficacy in patients with moderate-to-severe AD, resulting in rapid improvements in skin symptoms and overall quality of life. 18 Additionally, abrocitinib has demonstrated good safety profiles in both clinical trials and real-world studies. The majority of adverse events reported were mild to moderate in severity and rarely led to discontinuation of the drug. 19 Furthermore, abrocitinib has shown promising efficacy in patients who previously did not respond to other treatments, including biologics. 20 According to the Italian Delphi Consensus, abrocitinib shows good therapeutic outcomes in patients with AD affecting sensitive areas such as the face, neck, and hands. Moreover, abrocitinib exhibits satisfactory efficacy in treating various clinical phenotypes of AD, including nummular eczema, prurigo nodularis-like, and psoriasiform. 21
In this study, we focused on immune pathway- and severity-related biomarkers linked to AD. Biomarker profiles in the tape strips and serum of patients with AD were analyzed, and changes following abrocitinib treatment in patients with moderate-to-severe AD were observed. To better characterize the complexity of AD pathogenesis, we combined biomarkers from lesional and nonlesional skin, as well as serum. Comprehensive models have been developed to better reflect the systemic inflammation in AD and the targeted therapeutic effects of abrocitinib. These findings may contribute to the assessment of clinical severity and choice of personalized treatment.
MATERIALS AND METHODS
Study Population and Characteristics
We enrolled patients with AD between December 2021 and May 2023, following approval by the hospital ethics committee (KY2022149). All participants provided informed consent. Diagnosis of AD was based on Hanifin and Rajka’s criteria. 22 Patients with extrinsic and intrinsic AD were differentiated based on serum IgE levels: extrinsic AD was defined by levels exceeding 150 × 103 IU/L, while levels below this threshold indicated intrinsic AD.23,24 None of the patients had a history of other inflammatory skin diseases (eg, psoriasis or chronic spontaneous urticaria), autoimmune diseases (eg, rheumatoid arthritis), or systemic diseases. The exclusion criteria included active skin infections, use of biologics within the past 12 weeks, intake of oral steroids or immunosuppressants, phototherapy within the last 4 weeks, and application of topical corticosteroids within 2 weeks before sampling. Patients were also advised to avoid emollients and anti-inflammatory drugs at the sampling site the day before the next visit. Healthy volunteers showed no signs of atopic or chronic inflammatory disease.
Treatment
Patients with moderate-to-severe AD receive 4 weeks of oral abrocitinib, 100 mg once daily, after excluding any contraindications to JAK inhibitor use. Blood samples and tape strips were collected before and after the treatment. Eczema Area and Severity Index (EASI) and the scoring atopic dermatitis (SCORAD) scoring were performed concurrently.
Tape Strips and Blood Collection
Tape-stripping was performed on lesional and nonlesional skin using 10 consecutive D-squame tape strips (CuDerm, Dallas, TX). After 4 weeks of abrocitinib treatment, tape strips were collected again from the same sites to ensure unbiased sampling. For healthy controls, the forearm was chosen as the sampling site. Blood samples were collected from the patients and healthy controls, with serum separated and stored at −80°C. See Supplementary Methods for further details.
RNA Extraction and PCR Arrays
PCR arrays were performed on 20 preselected key AD-related genes as previously described. See Supplementary Methods for further details.
Serum Biomarker Analysis
Human Luminex Discovery Assay was used for analysis according to the manufacturer’s instructions. All Luminex assays were performed using a Luminex MAGPIX system (Luminex, Germany). See Supplementary Methods for further details.
Statistical Analyses
The statistical analysis was conducted using R software version 4.2.2. The muStat package was used to calculate the scores from the multivariate models. See Supplementary Methods for further details.
RESULTS
Study Participants
Fifty adults with mild-to-severe AD and 13 healthy individuals were enrolled in the study (Table 1). Among the patients with moderate-to-severe AD (n = 39), 21 received treatment with abrocitinib. Of these, 6 patients were lost to follow-up, while 15 patients ultimately completed the 4-week treatment. Tape strips and serum samples were collected from all participants at baseline and following the treatment.
Clinical Characteristics at Baseline
Age at the time of sample collection.
AD, atopic dermatitis; EASI, Eczema Area And Severity Index; EOS, eosinophils; IQR, interquartile range; NRS, Numerical Rating Scale; SCORAD, SCORing Atopic Dermatitis; SD, standard deviation.
Lesional and Nonlesional Skin Inflammations Captured by Tape Strips at Baseline
Compared with the healthy controls, the expression levels of Th1-related factors (interferon [IFN]-γ), Th2-related factors (IL-4R, IL-31, chemokine [C-C motif] ligand [CCL]17, CCL22, CCL27), FCER1A, matrix metalloproteinase (MMP)12, Th17/22-related factors (S100A7), and JAK-STAT signaling molecules (JAK1, TYK2) were found to be increased in both lesional and nonlesional tape-stripped skin (P < 0.05). JAK3 was elevated only in lesional skin (P < 0.05). Interleukin (IL)-33, JAK2, JAK3, and TYK2 exhibited higher expression levels in lesional skin than in nonlesional skin (P < 0.05) (Fig. 1). The lesions were classified into acute (n = 5), subacute (n = 22), and chronic (n = 23) stages based on the skin characteristics at the sampling sites. Biomarker analysis across different stages revealed that IL-33 expression was higher in acute and subacute lesions than in chronic lesions (P > 0.05) (Supplementary Fig. S1). No statistically significant differences were observed in the expression of other biomarkers, such as IL-4R and IL-13 (P > 0.05).

FCHs of biomarkers detected in lesional (LS) and nonlesional (NL) tape-stripped skin of AD and healthy controls (HC). +P < 0.1, *P < 0.05, **P < 0.01, ***P < 0.001. AD, atopic dermatitis; FCH, fold change.
Systemic Inflammation Persists in the Serum of Patients with AD
Associated inflammatory cytokines/chemokines were significantly increased in the serum of patients with AD at baseline compared with healthy controls. Biomarkers related to Th1 (IFN-γ, IL-18), Th2 (IL-4, IL-31, IL-33, CCL17), Th17/22 (IL-6, IL-17, IL-19), Treg (IL-10, CD25/sIL-2Rα), eosinophil migration (periostin, CCL26), and general inflammation (MMP12, CCL27) were significantly elevated (all P < 0.05, Fig. 2).

Radar plot comparing serum biomarkers between AD and healthy controls (HC). Spoke length represents the mean of serum biomarkers normalized by z-score. *P < 0.05, **P < 0.01, ***P < 0.001. AD, atopic dermatitis; Treg, T-regulatory cells.
Differential Expression of Skin and Serum Biomarkers in Patients with Intrinsic and Extrinsic AD
We matched 16 intrinsic to 16 extrinsic patients based on their EASI scores and compared the expression of skin and serum biomarkers between the 2 groups at baseline. Compared with the healthy controls, serum levels of biomarkers associated with Th1 (IFN-γ, IL-18), Th2 (IL-4, IL-13, IL-31, IL-33), Th17 (IL-6, IL-17, IL-19), Treg (IL-10, CD25/sIL-2Rα), general inflammation (MMP12, CCL27), eosinophil migration (periostin), and endothelial cell adhesion molecules (E-Selectin) were elevated in both intrinsic and extrinsic AD, with no statistically significant difference between the 2 groups (P > 0.05). However, CCL17 and CCL18 expression was higher in patients with extrinsic AD compared with that in patients with intrinsic AD (Fig. 3).

Comparison of biomarkers between intrinsic and extrinsic AD tape-stripped skin. +P < 0.1, *P < 0.05, **P < 0.01, ***P < 0.001. AD, atopic dermatitis; EAD, extrinsic atopic dermatitis; HC, healthy control; IAD, intrinsic atopic dermatitis; LS, lesional skin; NL, nonlesional skin.
Tape strips obtained from patients with lesional and nonlesional extrinsic AD showed a significant increase (P < 0.05) or a notable upward trend (P < 0.1) in the expression of the Th1-related (IFN-γ), Th2-related (IL-4R, IL-31, IL-33, CCL17), Th17/Th22-related (S100A7) factor, general inflammation factor (MMP12), and JAK-STAT molecules (JAK1, JAK2), in contrast to the healthy control group. The expression of FCER1A and CCL22 was elevated in the lesional and nonlesional skin of both groups, with extrinsic AD showing significantly higher expression levels than intrinsic AD (P < 0.05). Furthermore, when comparing intrinsic AD to extrinsic AD, a trend toward higher expression of the Th17/Th22-related factor (IL-19) was observed in lesional intrinsic AD (P < 0.1). Additionally, another Th17/Th22-related factor (S100A7) was significantly elevated in nonlesional intrinsic AD (P < 0.05) (Fig. 4).

Comparison of serum biomarkers between intrinsic and extrinsic. +P < 0.1, *P < 0.05, **P < 0.01, ***P < 0.001. AD, atopic dermatitis; EAD, extrinsic atopic dermatitis; HC, healthy control; IAD, intrinsic atopic dermatitis.
Inflammatory Biomarkers Correlate with Baseline AD Severity
At baseline, we observed positive correlations between clinical severity (SCORAD and EASI) and AD biomarkers in lesional and nonlesional skin and serum (Supplementary Table S1). In tape strips from lesional skin, EASI showed significant or near-significant correlations with IL-4R (R = 0.31, P = 0.03), Keratin (KRT) 16 (R = 0.3, P = 0.03), IFN-γ (R = 0.28, P = 0.05), and IL-33 (R = 0.26, P = 0.07). SCORAD correlated with a similar panel, including IL-4R (R = 0.32, P = 0.02), JAK2 (R = 0.29, P = 0.04), and JAK3 (R = 0.25, P = 0.08).
In nonlesional tape-stripped skin, IL-33 was inversely correlated with EASI (R = 0.29, P = 0.04) and SCORAD (R = −0.34, P = 0.01) while KRT16 showed a positive association with EASI in both lesional (R = 0.30, P = 0.03) and nonlesional skin (R = 0.28, P = 0.05). These biomarkers include CCL27 (R = −0.45, P < 0.01), TYK2 (R = −0.38, P = 0.01), IL-4R (R = −0.28, P = 0.05), and IFN-γ (R = −0.27, P = 0.06).
IL-33 had the highest correlation coefficient with EASI (R = 0.50, P < 0.01) compared with other serum biomarkers and was also positively correlated with the SCORAD (R = 0.37, P < 0.01). Other serum biomarkers highly correlated with EASI included CCL27 (R = 0.44, P < 0.01), CCL17 (R = 0.42, P < 0.01), IFN-γ (R = 0.42, P < 0.01), and CD25/sIL-2Rα (R = 0.40, P < 0.01). SCORAD was positively correlated with serum levels of CCL17 (R = 0.47, P < 0.01), CCL18 (R = 0.40, P < 0.01), and CCL27 (R = 0.37, P < 0.01) at varying levels.
Multivariate Correlation Models for Baseline AD Severity
We conducted a multivariate approach using μ-Scores, a computationally intensive algorithm, which revealed significantly higher correlations than those observed using the univariate approach. Representative multivariate biomarker combinations were correlated with clinical severity (measured using EASI) across different compartments (Fig. 5, Supplementary Table S2).
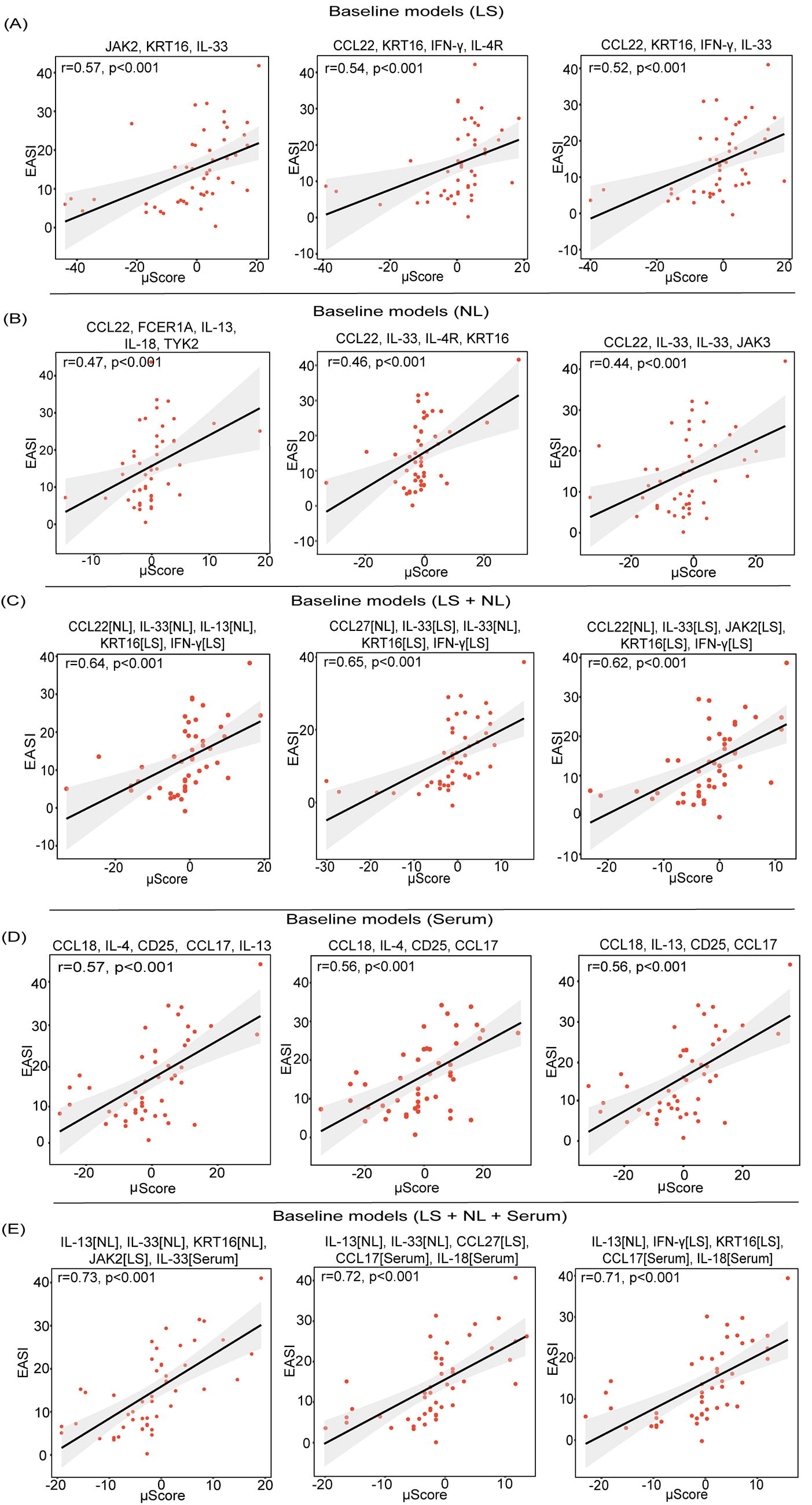
μScore models for the correlation of baseline biomarkers with EASI. Representative top biomarker combinations in lesional skin (LS)
Biomarker combinations in lesional skin showed a significantly higher correlation with EASI than with individual genes (Fig. 5A). The combination of Th2-related genes (IL-33, JAK2) and the epidermal hyperplasia-related genes (KRT16) showed the strongest correlation with EASI.
In nonlesional skin combinations of Th2-related biomarkers (IL-33, CCL22), were highly correlated with EASI (Fig. 5B). The correlation coefficients further increased when lesional and nonlesional biomarkers were integrated, with top combinations including lesional IFN-γ, IL-33, KRT16, and nonlesional CCL22 and IL-33 (Fig. 5C). When integrating serum, lesional, and nonlesional biomarkers, we achieved combinations that showed the strongest correlations with baseline EASI (R = 0.73, P < 0.001), which included nonlesional IL-13, IL-33, KRT16, lesional JAK2, and serum IL-33 (Fig. 5E).
Biomarkers Correlate with Early Abrocitinib Response
We calculated the correlation between improvements in disease severity and changes in biomarker profiles in lesional and nonlesional skin and serum. IL-33 showed a significant correlation with improvement in EASI in both lesional (R = 0.57, P = 0.03) and nonlesional skin (R = 0.46, P = 0.08). Reduced IL-4R expression in lesional skin (R = 0.48, P = 0.08) was positively correlated with EASI improvement. Alterations in JAK-STAT signaling molecules, specifically JAK3 (R = 0.55, P = 0.04) in lesional skin and TYK2 (R = 0.49, P = 0.07) in nonlesional skin, were similarly associated with SCORAD improvements. The strongest association between EASI and SCORAD improvement was observed for changes in IL-4 (R = 0.76, P < 0.01) and IL-6 (R = 0.67, P < 0.01) levels in the serum. Other Th2-related cytokines (IL-5, IL-31, IL-33, and IL-31), chemokines (CCL17 and CCL18), and Th17-related cytokines (IL-6 and IL-17) also showed significant correlations with EASI and SCORAD improvement (Supplementary Table S3).
Multivariate Correlation Models for Abrocitinib Treatment
The univariate correlation analysis showed that individual biomarkers from a single source were insufficient to reflect the treatment response to abrocitinib. Therefore, we modeled multivariate biomarker combinations to assess response to abrocitinib treatment (Supplementary Table S4, Fig. 6). For lesional skin, combinations containing IL-31 and IFN-γ were highly correlated with the degree of improvement in EASI, particularly the combination of IL-31, IFN-γ, IL-4R, and CCL22 (Fig. 6A). Additionally, combinations of Th2-associated biomarkers, such as IL-33, IL-4R, and CCL17, in nonlesional skin correlated with treatment response (R = 0.62, P < 0.05, Fig. 6B). The combination of serum IL-4, IL-31, and IL-18 exhibited the highest correlation with treatment response (R = 0.89, P < 0.05), followed by IL-4 and IL-17 (R = 0.88, P < 0.05, Fig. 6D).
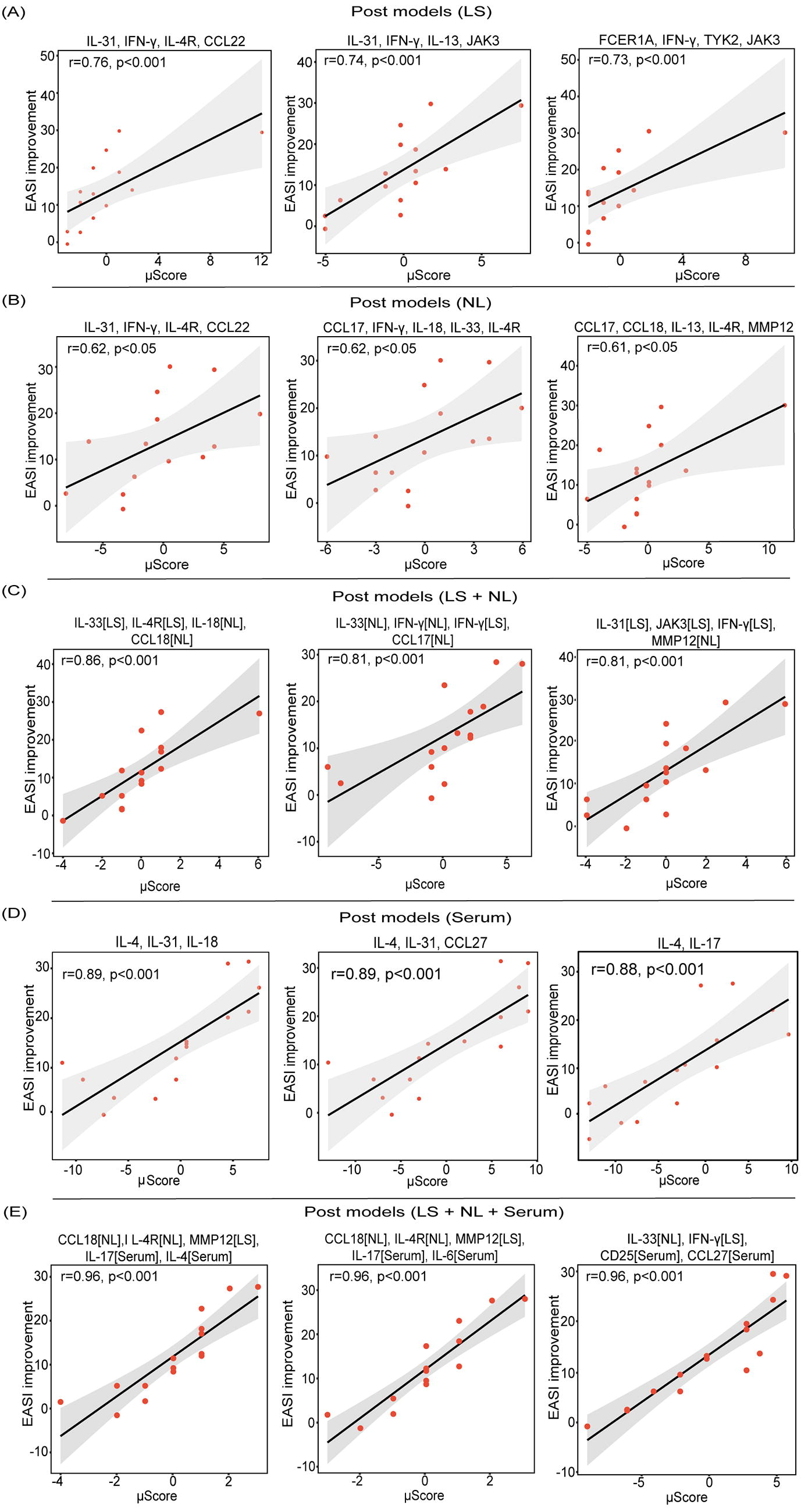
μScore models for the correlation of biomarker changes with clinical improvement (EASI). Representative top biomarker combinations in lesional skin (LS)
As observed at baseline, the combination of the lesional and nonlesional skin biomarkers enhanced the association with EASI improvement (Fig. 6C). Integrating biomarkers from all 3 sources yielded the highest correlation (R = 0.96, P < 0.01, Fig. 6E), reflecting the coordinated regulation of skin and blood in abrocitinib treatment in patients with AD.
DISCUSSION
Our study demonstrated that tape-stripping effectively monitored changes in the expression of key inflammatory biomarkers, including IFN-γ, IL-4R, IL-31, and IL-33, among others. Notably, certain biomarkers, such as FCER1A and S100A7, showed higher sensitivity in tape strips than in traditional biopsy for detecting nonlesional inflammation. S100a, known for its pro-inflammatory role in various inflammatory conditions, was significantly elevated in both acute and chronic AD lesions. 25 We observed significantly elevated S100A7 expression in the nonlesional skin of both intrinsic and extrinsic AD, with levels notably higher in intrinsic AD than in extrinsic AD. However, S100A7 expression in biopsied nonlesional skin did not differ significantly between intrinsic and extrinsic AD. Flow cytometry analysis revealed greater FcεRI expression in lesional extrinsic AD compared with that of intrinsic AD. 26 We detected high expression of FCER1A in both lesional and nonlesional skin of patients with extrinsic AD, a pattern not observed in biopsied tissues from the same patients. 27 This discrepancy may be attributed to the focus of the tape-stripping method on epidermal inflammation, which could be diluted in whole-layer biopsies. In summary, our study further confirmed the presence of a significant inflammatory burden in nonlesional AD skin.
Previous studies have shown that both extrinsic and intrinsic AD have similar Th2 inflammation activation in their lesions and that intrinsic AD shows higher immune activation. 27 In intrinsic AD, a high expression of Th17/Th22-related biomarkers (IL-19 and S100A7) was observed, consistent with prior findings. 27 Although phase 2 clinical trials revealed limited efficacy for biologics targeting IL-17 or IL-22 (eg, secukinumab, fezakinumab) in AD management, likely due to their inability to address Th2-mediated pathways.28,29 Notably, fezakinumab demonstrated significant efficacy in patients with severe AD (SCORAD ≥50), particularly among those with higher baseline IL-22 levels, indicating enhanced responsiveness in this phenotype. 30 These findings imply that therapeutic interventions targeting Th17/Th22 pathways may hold greater potential for patients with intrinsic AD subpopulations with specific biomarker profiles. Fezakinumab could serve as a potential second-line therapy for patients with severe AD characterized by high IL-22 expression. A combined clinical assessment incorporating biomarker profiling and phenotypic stratification is warranted.
Guttman-Yassky 31 observed that abrocitinib significantly downregulated the expression of Th22-related biomarkers, including S100A8, S100A9, S100A12, and also impacted Th2-related biomarkers such as CCL17 and CCL18. These changes were closely correlated with clinical symptoms, such as skin clearance and relief of itching. This suggests that targeting type 2 inflammatory cytokines remains the core of AD treatment, whether intrinsic AD or extrinsic AD. Extrinsic AD showed higher levels of FCER1A and CCL22 compared with those of intrinsic AD, with elevated CCL17 and CCL18 levels observed only in patients with extrinsic AD. Specific IgEs may trigger skin inflammation by activating mast cells and dendritic cells through FCER1A, whereas intrinsic AD often lacks a sensitizing source. 32 CCL17 has been widely associated with AD severity and treatment response.33-35 Additionally, CCL17 and CCL22, ligands for CCR4, are upregulated in AD lesions. 36 Significant increases in serum CCL17, CCL22, and lesional CCL18 levels have been observed in patients with AD exposed to sensitizers.32,37 The elevated expression of CCL17 and CCL22 may contribute to Th2 cell infiltration and skin inflammation in patients with extrinsic AD.
There was an increased expression of JAK1 in both lesional and nonlesional AD skin, with no significant difference between the 2. Elevated levels of JAK1 and TYK2 were observed in both lesional and nonlesional skin of patients with intrinsic and extrinsic AD, while JAK2 and JAK3 expression was only increased in the lesional skin of patients with extrinsic AD. These findings suggest that targeting JAK1 may be a more effective strategy for managing inflammation in both lesional and nonlesional skin, regardless of whether intrinsic or extrinsic AD. However, due to the limited sample size, we are unable to compare the differences in therapeutic efficacy between patients with intrinsic and extrinsic AD.
Previous studies have reported that serum IL-33 is a strong predictive biomarker for SCORAD. 38 Our data further demonstrated a significant correlation between IL-33 expression in lesional skin, nonlesional skin, and serum, with EASI at baseline and post-treatment improvement. IL-33 is a cytokine belonging to the IL-1 family and plays a key role in regulating TH2-type immunity and inflammatory responses. 39 Its expression is elevated in AD keratinocytes and is released following skin injury such as scratching or irritation. This release directly suppresses filaggrin expression and indirectly exacerbates epidermal barrier damage through Th1 and Th2 type inflammation.40,41 Our findings suggest that IL-33 is prominently present in acute and subacute AD lesions, indicating its crucial role in initiating skin inflammation; however, its impact may be limited in persistent skin inflammation. This is additionally backed by a phase 2 clinical trial that showed no statistically significant differences in primary or secondary endpoints between the AD treatment group and the placebo group after 16 weeks of anti-IL-33 monoclonal antibody therapy. 42
Barrier and immune dysregulation are well established in nonlesional AD 12 ; however, the expression of nonlesional biomarkers is rarely included in the assessment of AD severity. In this study, we employed multivariate μ-statistics to create comprehensive models of disease severity, incorporating inflammatory biomarkers from both lesion and nonlesional skin, as well as blood samples. We found that the correlation with EASI significantly increased when combining multiple skin- or serum-derived biomarkers, such as the JAK2, KRT16, IL-33 combination in lesional skin, the CCL22, FCER1A, IL-13, IL-18, TYK2 combination in nonlesional skin, and the CCL18, IL-4, CD25/sIL-2Rα, CCL17, IL-13 combination in serum. IL-4 and IL-13 are central molecules in type 2 inflammation and key factors in AD pathogenesis. Previous research has indicated that AD is primarily driven by IL-13-induced inflammation rather than IL-4. 43 The level of IL-13 in the serum has been linked to the severity of AD; however, the connection between IL-4 and disease severity has not been explored. 44 Our serum integration model proposes that IL-4 in the serum contributes to the progression of AD by interacting synergistically with IL-13, CCL17, CCL18, and CD25/sIL-2Rα, and is associated with disease severity.
The highest correlation coefficient with the EASI was achieved when combining JAK2 in lesional skin, IL-13 and IL-33 in nonlesional skin, and KRT16 and IL-33 in serum. Similar to the baseline modeling results, the combination of lesional and nonlesional biomarkers improved the correlation with EASI improvement after treatment. The combination of MMP12 in lesional skin, CCL18 and IL-4R in nonlesional skin, and IL-4 and IL-17 in serum showed the strongest correlation with the improvement in EASI. In the future, biomarker combinations derived from the skin or serum could be selected to assess AD severity and predict the response to abrocitinib treatment based on clinical needs.
Current AD treatment relies on empirical approaches due to the lack of reliable biomarkers for personalized therapy. The strategy integrating skin and serum biomarkers provides a novel strategy to guide clinical decisions. A comprehensive assessment of cutaneous and systemic inflammation enables patient stratification for more precise therapeutic strategies. Integration of biomarker models significantly enhanced their correlation with AD clinical scores, particularly when IL-33 was included in both lesional and nonlesional skin. Our multivariate analysis further confirms systemic inflammation in AD. This approach optimizes biological and small-molecule drug use by minimizing unnecessary exposure, reducing adverse effects, and improving safety and cost-effectiveness. Thus, the precision medicine approach integrating skin and serum biomarkers not only enhances abrocitinib efficacy, but also establishes a rigorous scientific foundation for future personalized treatment.
One of the limitations of this study is the relatively short follow-up period, which was designed to assess the early therapeutic responses of abrocitinib in patients with moderate-to-severe AD. Extending the treatment duration may lead to more persistent immunomodulatory effects, particularly the continued inhibition of the Th2/Th22 pathways could result in more significant changes in skin biomarkers. Additionally, although the minimally invasive nature of the tape-stripping method is beneficial for patients, its complex sampling procedure poses challenges to clinical and commercial adoption. Moreover, the participants in this study were from a limited cohort of Asian patients, which may have restricted the generalizability of the findings to a broader population. Future research should involve multiple international centers to include more geographic and ethnic diversity. Larger studies are needed to confirm these findings, especially in groups with different genetic and environmental factors.
CONCLUSION
Our study confirmed that tape-stripping can effectively identify key pathogenic biomarkers in the skin of patients with AD. Integrating skin and serum biomarkers enables more precise disease evaluation, improves individualized prediction of abrocitinib treatment outcomes, and advances precision medicine strategies.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.