
Abstract
Capsule Summary
First epidemiological evidence linking ambient temperature and humidity to facial aging.
Ambient temperature and humidity are associated with forehead hyperpigmentation and coarse wrinkles in Indian women.
Associations were robust to confounding by UVR and age.
INTRODUCTION
From 1850–1900 to 2010–2019, the likely ranges of total anthropogenic global surface temperature increase were 0.8–1.3°C, with an average of 1.07°C. 2 The Intergovernmental Panel on Climate Change in its latest assessment report (AR6) has stated in the strongest terms that this temperature increase will lead to an unavoidable increase in multiple climate and weather extremes, which will pose multiple risks to humanity.3–5 Indeed, there is growing evidence that global warming poses a major threat to human health.6,7 Importantly, human health is more severely affected by the combination of ambient temperature and relative humidity (RH) than by temperature alone.8,9 Therefore, slightly different types of heat indices (HIs) have been developed, to model the combined effect of ambient temperature plus RH.10,11 Increases in such HI have been found to be associated with increased mortality and morbidity. 12 Strongly affected health outcomes included infectious diseases, cardiovascular and respiratory diseases, and mental health problems.6,13 However, a less studied topic in epidemiology is the effect of extreme heat on human skin aging phenotypes.
Environmental factors may act in concert to promote the development of coarse wrinkles and pigmentary irregularities.14–16 Existing epidemiological evidence has reported the potential effects of ultraviolet radiation (UVR) and air pollution on skin aging phenotypes.17–21 UVR has been reported to be the most studied and most damaging environmental factor contributing to skin aging. 22 Recently, the skin aging exposome study by Krutmann et al 22 proposed ambient temperature as a novel exposomal factor inducing skin aging. However, epidemiological evidence to support this hypothesis is lacking. Mechanistic studies conducted in the past have proposed that heat contributes to the development of skin aging,22,23 and in this context, the term “thermal aging” was coined. 24 Thermal aging mainly refers to studies in which acute heat shock responses (>40°C skin temperature) were induced in human skin, for example, by short-term (90 minutes) exposure to heating pads at 43°C. Such treatments induced neovascularization and altered the composition of the extracellular matrix (reviewed in Krutmann et al 22 ) by mechanisms that probably involve the activation of transient receptor potential vanilloid (TRPV-3) receptors in skin cells.25–27 However, it is not known whether long-term (ie, several years of exposure to slightly elevated [up to 1°C]) ambient temperature, as is the case with global warming, can affect the development of skin aging signs such as coarse wrinkles and irregular pigmentation (age/pigment spots, lentigines) in the general population.
Studies on the combined effect of ambient temperature and RH on skin aging phenotypes are of particular interest to countries such as India, which has experienced an unprecedented increase in extreme heat episodes over the past few decades, 28 making heat 1 of the leading risk factors for mortality in India. 29 Classified as a tropical monsoon climate due to its poor infrastructure, high population exposure, and low adaptive capacity to cope with extreme heat, India’s population is highly vulnerable to the harmful combination of temperature and humidity. At the same time, India’s dangerously high levels of air pollution and UV index (UVI) put the population at even greater risk. Therefore, it is important to assess the potential health effects of prolonged high HI exposure in the Indian population. In the present epidemiological study, we aimed to investigate the effect of elevated HI in a 5-year mean exposure window on skin aging phenotypes in Indian women in a cross-sectional study design from 3 different geographical areas. The study regions considered in India are reported to be influenced by contrasting levels of HI, high levels of air pollution, and solar UVR, and therefore the choice of the Indian cohort seemed advantageous for the comparison of effects.
MATERIALS AND METHODS
Study Cohort
For this analysis, we used data from the ongoing climate, air pollution, and skin aging in Indian women (CASAI) cohort in India. The cohort started in 2018 and recruited 1510 Indian women aged 20–91 years between 2018 and 2019 from 3 metropolitan cities in India: Delhi, Mumbai, and Bengaluru. Only women with skin phototypes 3 and 4 were included. In each city, approximately 500 women were recruited through local clinical laboratories. The cities were selected based on their different levels of air pollution and different types of weather. Standard survey procedures and questionnaires were reviewed and approved by local authorities in India. In addition, the clinical examination was conducted in accordance with the recommendations for research involving human subjects adopted by the 18th World Medical Assembly, the Declaration of Helsinki, and subsequent revisions. 1 All participants gave voluntary written informed consent. The study was conducted in all 3 areas during the dry season.
Study Region
The cities represent different levels of air pollution and different types of weather. Delhi represents a highly polluted city. It has distinct seasonal patterns, such as hot summers, cold and dry winters and rainy seasons, and a short period of autumn and spring. The temperature varies from 46°C in summer to around 0°C in winter. Mumbai is moderately polluted and moderately hot with high humidity throughout the year with a distinct rainy season (JJAS). The temperature varies from 36°C in hot summers to 19°C in mild winters. Bengaluru is a less polluted city and due to its high altitude, Bengaluru usually enjoys a more moderate climate throughout the year with a distinct wet and dry season, although occasional heat waves can make the summer somewhat uncomfortable. Bengaluru receives rainfall from both the northeast and southwest monsoons, with good rainfall between May and October and the wettest month being September, followed by October and August. Temperatures range from 16°C in January to 35°C in April and May.
Skin Aging Assessment
Skin aging was assessed at 1 time-point using a validated score, the Score of Intrinsic and Extrinsic Skin Aging (SCINEXA™), 30 to assess extrinsic skin aging characteristics of the face. The SCINEXA scores are based on the Tschachler and Morizot 31 photoreference scales. This tool has been used previously in several epidemiological studies.17,19,30,32,33 The number of pigment spots (≥3 mm in diameter) on the forehead and cheeks was scored as follows: 0 (no spots), 1 (1–10 spots), 2 (11–50 spots), and 3 (>50 spots). The 6 major wrinkle signs (wrinkles on the forehead, in the frown lines, in the crow’s feet, under the eyes, on the upper lip, and in the nasolabial fold) were scored as follows: 0 (not present) to 6 (very severe). The score was originally developed for Caucasians and was adapted for the Indian population in this study by incorporating specific skin aging characteristics of the Indian population according to the Skin Aging Atlas by Bazin and Flament. 34 The assessment and scoring were carried out by trained staff on-site using a standardized protocol. 30 In addition, facial photographs were taken of each woman using Visia-CR (Canfield Scientific, Inc.). The skin aging scores were re-categorized into 4 categories, with 0 indicating no signs of skin aging, the original scores 1 and 2 being combined as low severity, 3 and 4 as moderate severity, and 5 and 6 as high severity. To illustrate the spectrum of severity of skin aging phenotypes in women of this cohort, we have added some photographs and corresponding gradings in Supplementary Figure S2.
Environmental Exposures
Daily mean temperature (Tmean) and RH were obtained from the website of the Central Pollution Control Board (CPCB) of India (https://cpcb.nic.in/). Individual exposures were modeled based on the nearest monitoring station. Daily Tmean and RH data were obtained from ERA 5 reanalysis data at 10 × 10 km (www.ecmwf.int/en/forecasts/dataset/ecmwf-reanalysis-v5) 35 as observed data were missing for study participants in Mumbai. The validation of the data is presented in Supplementary Appendix SA1. Solar UVR exposure was determined by the (UVI, which describes the expected daily peak of erythemal UV irradiance at ground level. The UVI is based on the hour of maximum UVR per day. The UVI includes both ultraviolet B (UVB) and ultraviolet A (UVA) radiation but is mainly determined by the UVB dose. The spatio-temporal data of UVI have been extracted from the Tropospheric Emission Monitoring Internet Service (www.temis.nl/index.php) for each city with a resolution of 25 × 25 km. 36 Daily data on particulate matter with an aerodynamic diameter of <2.5 µm (PM2.5) were obtained from a satellite-based ambient PM2.5 database developed for India at a high resolution of 1 × 1 km. 37 Ground-level nitrogen dioxide (NO2) measurements were conducted at 60 outdoor sites in each of the 3 cities during the winter of 2019–2020. Individual outdoor residential NO2 exposures for participants in the 3 cities were estimated using the inverse distance-weighted method.38,39 In general, all data were extracted for the last 5 years from the date of examination at the participant’s coordinates, and values were averaged as a 5-year mean, with some deviations to account for missing data.
For analysis, we used the HI developed by Rothfusz
10
as a main exposure because it has been widely used in the past to determine the risk of heat-related morbidity.11,40,41 The HI was calculated as
Statistical Analyses
All women for whom information on skin aging phenotypes was available were included in the analysis, so our final study sample comprised 1510 women with complete information on skin aging phenotypes. We performed a correlation analysis between the different covariates used in the present analysis. The choice of correlation test depends on the structure of the variables, whether continuous, nominal, or ordinal. 43 A correlation coefficient (r) >0.7 was considered to indicate high multicollinearity. Because of the ordinal nature of skin aging outcomes, we analyzed the association of extrinsic skin aging with long-term exposure to HI using a multivariate ordinal logistic regression model, adjusting for potential confounders such as UVI and age, which have been shown to be associated with skin aging in previous studies.17,18 UVI is considered an important risk factor for skin aging in response to growing concerns about the potential increase in UVR-induced skin damage due to ozone depletion. 44 Failure to adjust for UV radiation would therefore introduce uncertainty into the results. We used 1 IQR increment for UVI. Predictor variables were centered around zero before fitting the model to reduce problems of multicollinearity. In addition, we assessed effect modification based on passive smoking exposure and age (<50 years and >50 years) to investigate whether passive smoking exposure and age modify the association between HI and skin aging characteristics. We performed some sensitivity analyses to test the robustness of the model. First, we used Tmean as the main exposure variable instead of HI. Second, because UVI and air pollutants (NO2 and PM2.5) were highly correlated, the main model was not adjusted for the potential effect of air pollutants, but we performed a sensitivity analysis replacing UVI with PM2.5/NO2. Third, we performed a separate analysis using only participants from Delhi, who are exposed to a wide range of temperatures throughout the year.
All results from the above analyses were presented as odds ratios (ORs) with 95% CIs for a 1°C increase in HI. The data were analyzed using the R statistical software version 4.1.2; the R package “MASS” (version 7.3-54) was used for subsequent analysis. 45
RESULTS
Description of the Study Cohort and SCINEXA Scores
Summary statistics are shown in Table 1. The analyses included 1510 women with a mean age of 45.5 years (SD ± 15.5). Most of the participants were nonsmokers (99.7%), but about one-third of the participants (35.2%) were exposed to passive smoking. The skin aging characteristics are shown in Table 2. The participants showed the presence of both skin aging phenotypes, facial pigmentation, and coarse wrinkles. Based on the SCINEXA scores, the signs of skin aging, when present, were generally in the low to moderate category. However, some participants had high severity signs of facial aging.
Study Characteristics of CASAI Cohort Participants
The values represent 5-year mean averages at the participant’s address prior to investigation.
Mean ± standard deviation is presented for continuous parameters, N (%) is presented for categorical parameters.
CASAI, climate, air pollution, and skin aging in Indian women; HI, heat index; NO2, nitrogen dioxide; PM2.5, particulate matter <2.5 µm; RH, relative humidity; UVI, ultraviolet index.
Description of SCINEXA Scores in CASAI Cohort
Low score range from 1 to 2, medium from 3 to 4, and high from 5 to 6.
SCINEXA, Score of Intrinsic and Extrinsic Skin Aging.
Climate and air pollution exposures at residence
Summary statistics of weather variables and exposure to air pollutants at participants’ addresses are shown in Table 1. The long-term mean (±SD) HI, Tmean, RH, and UVI for CASAI participants were 29.0°C (±1.0), 26.5°C (±0.6), 66.3% (±8.0) and 10.3 (±1.5), respectively. The long-term mean (±SD) PM2.5, and NO2 concentrations were 104.7 (±40.7) μg/m3 and 49.4 (±14.1) μg/m3, respectively, at the addresses of the CASAI participants, which are much higher than the WHO and Indian national air quality standards (PM2.5: 40 μg/m3; NO2: 50 μg/m3). 46 It should also be noted that the average annual temperature and air pollution levels in the Indian subcontinent are higher than in most countries in the northern hemisphere.47,48
HI and Extrinsic Skin Aging Traits
The association between long-term HI and extrinsic skin aging features is shown in Figure 1. The univariate model showed a significant association between HI and hyperpigmented macules on the forehead and coarse wrinkles (frown lines, crow’s feet, under the eyes). Notably, the associations between HI and extrinsic skin aging traits remained positive and significant after adjusting the model for the confounding effects of solar UVI and age. In the adjusted model, each 1°C increase in HI was associated with a 1.31-fold (95% CI: 1.12, 1.54) increase in the odds of “hyperpigmented macula on the forehead,” a 1.17-fold (95% CI: 1.05, 1.30) increase in the odds of “crow’s feet,” and a 1.3-fold (95% CI: 1.15, 1.47) increase in the odds of “eye wrinkles.” Negative and significant associations were also found between HI and pigmented spots on the cheeks and “nasolabial wrinkles.”
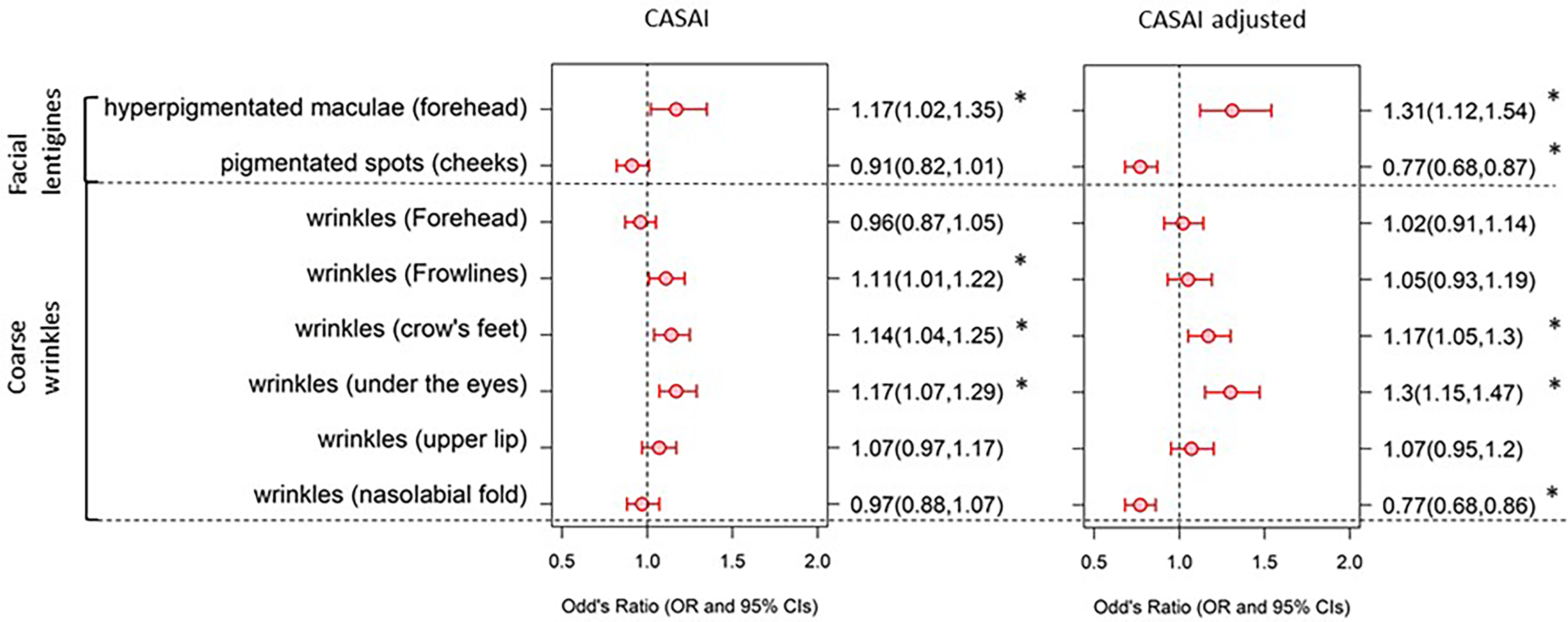
Association between HI with scores for extrinsic skin aging in the CASAI cohort. Adjusted—the estimates are adjusted for UVI and age; * shows that the values are significant at P < 0.05. CASAI, climate, air pollution, and skin aging in Indian women; HI, heat index; UVI, ultraviolet index.
Effect Modification
Smoking or exposure to passive smoking may increase the risk of developing extrinsic signs of skin aging. 49 Therefore, we performed effect modification to investigate whether exposure to passive smoking modified the association between HI and skin aging. As most of the participants were nonsmokers, the analysis was restricted to passive smoking exposure. The interaction between HI and passive smoking was insignificant for all skin aging. The effect modification by age over 50 years also shows no significant interaction between HI and age.
Sensitivity Analysis
In order to determine the robustness of our core model, we conducted several sensitivity analyses (Table 3). The results of replacing HI with Tmean as our main exposure variable show similar results to the main model. Similarly, replacing UVI with PM2.5/NO2 in the main model gave similar results. Thus, the sensitivity analysis results support that the association between HI and skin aging is robust to the use of an alternative temperature metric or the inclusion of air pollutants as a potential confounding factor. In a third step, we restricted the analysis to participants from Delhi. The results showed no significant associations between HI and signs of skin aging, due to the low power of the sample for the analysis.
Association of HI with Markers of Extrinsic Skin Aging in CASAI Cohort, Using Additional Model Specifications
Values in bold are significant at P < 0.05.
OR, odds ratio; UCL, upper confidence interval; LCL, lower confidence interval.
DISCUSSION
To the best of our knowledge, this is the first epidemiological study on the effect of high temperature and humidity on skin aging phenotypes in Indian women. We found a positive association of HI with facial pigmentation and coarse wrinkles in a cohort of Indian women. It is worth noting that an increase in ambient temperature is usually associated with an increase in sun intensity. Given that sun exposure consists of harmful UVR, which threatens the skin and is a major cause of skin aging, we carefully assessed the potential confounding role of UVI. 50 The results clearly show that the association between HI and facial pigmentation (hyperpigmented macules on the forehead) and coarse wrinkle signs (crow’s feet and under-eye wrinkles) was robust, after accounting for the confounding effect of UVI and age. The results show that temperature is an independent threat to skin aging, along with solar UV and air pollution. Many people living in high-temperature areas have high heat thresholds. 51 For example, the heat thresholds for people living in Delhi, Mumbai, and Bengaluru (India) are 25.5–26.5°C, 28.5–29.5°C, and 29.5–30.5°C, respectively. This suggests that people exposed to high temperatures for long periods of time gradually adapt to warmer temperatures, and therefore may have a gradually attenuated response to heat. 51 This may also explain the better adaptability to heat and less severe skin aging in Indian women. On the other hand, the high severity of certain skin aging characteristics in the study population may be related to the higher HI levels in India. In general, we found that Indian women are exposed to higher levels of environmental exposures, such as HI, UVI, PM2.5, and NO2. We have previously shown that SCINEXA is significantly associated with both chronological age and UV exposure (sunbed use) and that these associations were not confounded by skin phototypes. 30 It is currently unknown whether different skin phototypes have different susceptibilities to the observed association between HI and skin aging phenotypes. Effect modification showed no significant interaction between HI and passive smoking for severe facial pigmentation and coarse wrinkles in CASAI. This may be due to the low exposure to passive smoking among CASAI participants. Smoking is undoubtedly a potential risk factor for premature skin aging. 49 Tobacco smoke extract increases the degradation of collagen tissue and elastic fibers through several pathways. Previous studies have shown that smoking modifies the association between O3 and coarse wrinkles, 21 but there is no prior evidence on whether smoking modifies the association between temperature and skin aging. Effect modification based on age, below and above 50 years, mostly resulted in insignificant associations. In contrast to our study, a study focusing on German and Chinese women reported a higher effect of NO2 on facial pigmentation when the analysis was restricted to Chinese women above 50 years of age. 17 However, there is no evidence of whether age modifies the association between temperature and skin aging.
As part of the sensitivity analysis, Tmean was chosen as an alternative temperature metric to show that temperature does not independently affect the aging parameter. HI seems to be a better choice than Tmean. The main reason is that temperature doesn’t affect health on its own. Instead, health effects often result due to a combined function of temperature and humidity, such that the combined effect of temperature and humidity is often more detrimental than their individual effects.41,52–54 Therefore, HI is the better temperature metric to show heat-induced health effects. Similarly, previous studies have shown a significant association between PM2.5 and NO2 (NO2 is a more specific indicator of traffic-related air pollution) and facial pigmentation in older German women,17,18 so we used these pollutants as potential confounders in this study. We accounted for the potential bias in the association due to differences in HI exposure (due to large seasonal differences in HI in New Delhi). The analysis conducted after including participants from Delhi only did not show significant associations due to low sample size power.
As this is the first epidemiological evidence of the role of environmental temperature expressed as HI, the biological mechanism establishing a causal relationship between temperature and skin aging characteristics is lacking. A mechanistic study based on animal models found that high skin temperature upregulates tropoelastin, fibrillin, and matrix metalloproteinase (MMP) expression55,56 and induces oxidative DNA damage. 57 MMP is an extracellular matrix-degrading enzyme that causes the degradation of extracellular matrix proteins such as type 1 and type 3 collagen in the dermis, contributing to skin wrinkling.58,59
The study has several strengths. First, it is the first epidemiological evidence of the role of ambient temperature as HI on extrinsic signs of skin aging in Indian women. Second, the study uses a well-characterized cohort from 3 different geographical regions with contrasting levels of exposure and different skin aging traits, thus contributing to a better understanding of the variation in the strength of association with different levels of exposure. Third, the study uses the validated SCINEXA tool to differentiate between extrinsic and intrinsic signs of skin aging. 30 Fourth, we used a multiexposure model adjusting for the strong confounding effect of solar UVR and PM2.5/NO2 (in a sensitivity analysis) to show that the observed associations of HI with extrinsic signs of skin aging were independent of other factors. Fifth, we performed sensitivity analyses to test the robustness of the core model.
There are several caveats to this study. First, we performed the exposure assessment partly based on modeled climate and air pollution data, which may have led to misclassification of individual exposure. Second, because we relied in part on modeled exposure data, we cannot completely rule out uncertainty in the true relationship between HI and extrinsic signs of skin aging. Thirdly, due to the lack of harmonized information on the personal characteristics of the study participants, the model could not account for other potential confounders and several effect modifications could not be tested. For example, we have no information on indoor exposure due to cooking with fossil fuels, which is a major problem in India. Similarly, we do not have information about occupational exposures and how they affect skin aging. For example, women who have high occupational exposures would have worse SCINEXA scores related to work-related chronic exposures. This type of information is not available, and its absence is a pitfall of this study.
CONCLUSIONS
The study provides the first epidemiological evidence of an adverse role of HI as a combined function of ambient temperature and RH on facial pigmentation and coarse wrinkling in Indian women, independent of other known potential environmental risk factors. As environmental factors are closely interrelated, future investigations of skin aging need to consider the interactions of ambient temperature with solar UVR and air pollutants. In addition, mechanistic studies are needed to further establish a causal relationship between the long-term effects of temperature and skin aging phenotypes.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.