
Abstract
Objective:
To determine disease severity, burden, and treatment use and satisfaction in adults with AD.
Methods:
An international internet-based survey was conducted (October 5–November 1, 2021) in participants with AD from Canada, France, Germany, Italy, Japan, Spain, the United Kingdom, and the United States.
Results:
Of 2005 AD patients surveyed, 92% had body surface area (BSA) involvement <10%. Itch was the most bothersome symptom; 48.5% of participants reported severe itch in the past week (Itch Numerical Rating Scale [NRS] 7–10; 45.9% for BSA <10%, 75.0% for BSA ≥10%). Most participants reported moderate or severe sleep disturbance in the past week (Sleep NRS 4–10; 67.1% for BSA <10%, 92.3% for BSA ≥10%). Itch was the top reason for participants' most recent health care provider visit; reducing itching was their top treatment goal. Topical therapies, which were most commonly used, resulted in low treatment satisfaction.
Conclusions:
Itch was the most bothersome AD symptom. Although clinical development has focused on improving skin lesions, improving itch is patients' top treatment goal. This survey highlights the need for systemic antipruritic therapies that could reduce itch in nonlesional and lesional skin.
Capsule Summary
This international online survey found that itch is the most bothersome symptom for patients with atopic dermatitis (AD) and reducing itch is their top treatment goal.
Most respondents used topical treatments; however, treatment satisfaction was low for topical treatments across all measured disease domains.
There is an unmet need for antipruritic therapies, particularly systemic therapies, for patients with AD.
Atopic dermatitis (AD) is a chronic inflammatory skin disease that affects up to 2% to 10% of adults worldwide.1,2 Symptoms of AD include itch, skin pain, sleep disturbance, and decreased quality of life (QoL). 3 AD has a large impact on patients' lives, including disruption of relationships, frequent embarrassment about their appearance, and a negative impact on work or school. 4 Patients with AD frequently have disrupted sleep patterns, including trouble falling asleep and staying asleep. 4 Patients with AD also have increased risk of developing anxiety and depression. 3
The most common symptom of AD is itch accompanied by an urge to scratch, to the extent that the disease is commonly referred to as the “itch that rashes.” 5 Up to 100% of AD patients spontaneously report itch, and 60% of patients report their itch is severe to very severe.2,6–8 Even patients with mild-to-moderate AD report itch as a major contributor to their reduced QoL with variable treatment satisfaction.7,9–11
AD is an incredibly heterogeneous disease, with variation in the presentation, severity, and frequency of signs and symptoms. 12 Despite many clinical trials focusing on moderate-to-severe AD, reports indicate that most adults with AD suffer from mild-to-moderate disease, 2 which may differ in inflammatory signature and therapeutic needs compared with more severe disease. 9 Thus, to further understand the effects of AD symptoms from the perspective of the patient, we conducted an international survey to evaluate disease and symptom burden, treatment use, and treatment satisfaction in adults with AD.
METHODS
Burden of disease and unmet needs in atopic dermatitis (BAND-AD) was a 45-minute internet-based survey conducted by AplusA Bell Falla (Newark, NJ) between October 5 and November 1, 2021. Institutional review board approval for data collection in the United States was received before the survey was commenced; applicable regulations of other countries participating in the study were followed as well. All participants provided informed consent before participating in the survey.
Respondents were screened from an existing research panel and drawn from Canada, France, Germany, Italy, Japan, Spain, the United Kingdom, and the United States. For eligibility, respondents had to be adults (age ≥18 years; ≥20 years in Japan) with a previous health care provider diagnosis of AD and currently experiencing symptoms of AD. Respondents had to consent to participation and potential pharmacovigilance follow-up. Respondents were excluded if they or a family member worked in market research, advertising, pharmaceuticals, or the health care/health insurance field.
Screening continued until the prespecified quotas were obtained (n = 500 respondents for the United States, n = 215 respondents for all other countries). Survey topics included questions about demographics, disease severity, disease history, disease and symptom burden, symptoms experienced in the past week, the physical location and overlap of AD symptoms, treatment history and satisfaction, and treatment-seeking behaviors. Symptoms assessed included those extracted from validated AD tools including the Patient-Oriented Eczema Measure (POEM) and Patient-Oriented SCORing Atopic Dermatitis index.13–15
Severity of AD was defined by self-reported body surface area (BSA) and POEM. Participants were asked how many palms of eczema they had over the past week. Less than 10 palms of eczema was defined as BSA <10% and mild-to-moderate AD; ≥10 palms of eczema was defined as BSA ≥10% and severe AD. POEM scores of ≤7 were defined as mild, 8–16 as moderate, and ≥17 as severe eczema. Participants were also asked to identify the location of rash and itch on their skin using a body map (both ventral and dorsal perspectives, with 30 distinctly marked locations).
Ranks-based assessments were obtained for some survey items. In these instances, participants were presented with a list of choices and asked to put them in rank order. Data were summarized descriptively using sum of ranks.
RESULTS
Population
Of 23,308 individuals screened, 2005 met eligibility criteria and completed the survey (screen fail rate: 74%). Participants were considered screen failures due to 1 or more of the following: (a) not consenting to participation and/or protocol violation, (b) respondent or family member works in the market research, advertising, pharmaceutical, health care/health insurance field, (c) not meeting age inclusion criteria, (d) not having a diagnosis of AD (primary reason for screen fail, representing 78% of excluded respondents), or (e) does not currently have AD. Survey participants were with a mean age of 42.1 years, 54% were female, and the mean age at first AD diagnosis was 25.2 years (range: <1–83 years; Table 1).
Patient Demographics and Disease History
*Other includes nonbinary/nonconforming and “prefer not to answer” categories.
†N = 1697 for these categories because some respondents were unable to recall the age at which they first received an AD diagnosis from their health care provider.
AD, atopic dermatitis.
Most survey participants (92%) reported BSA involvement <10% (Fig. 1A). This was true regardless of county of residence, with 83% (United Kingdom) to 97% (Spain) of each country's respondents reporting a BSA <10% (Fig. 1A). Based on the POEM score, most participants had mild (31%) or moderate (47%) AD (Fig. 1B). The United States had the greatest proportion of respondents reporting severe or very severe POEM scores (33%), while Spain had the lowest (11%).

AD severity by BSA and POEM. Severity of AD was defined by BSA and POEM. (A) Participants were asked: Based on the amount of eczema that could be covered by the palm of your hand (excluding fingers), would you say that you have 0 palms (no eczema), <1 palm, 1–3 palms, 4–9 palms, 10–19 palms, or 20 or more palms of eczema that has covered your body over the past week (<10% BSA = 0–9 palms; ≥10% BSA = 10 or more palms). (B) Participants were asked: For the next series of questions, we would like you to think of your experience and symptoms solely due to your eczema that have occurred over the past week (POEM score questions). For purposes of this report, calculated POEM scores of “clear or almost clear” and “mild” are presented combined as mild, and “severe” and “very severe” are presented combined as severe. AD, atopic dermatitis; BSA, body surface area; POEM, Patient-Oriented Eczema Measure.
Itch Is the Most Prevalent, Severe, and Burdensome Symptom
To evaluate AD symptoms, respondents were presented with 11 common AD symptoms (derived from validated AD tools as described in the Methods section) or a write-in choice of “other.” A numerically lower percentage of participants with BSA <10% compared with ≥10% reported experiencing each symptom in the past week. The top 3 most commonly occurring symptoms in the prior week, regardless of BSA, included itchy skin, dry or rough skin, and redness or change in skin color, which were also reported to occur with the greatest severity during the past week (Fig. 2).
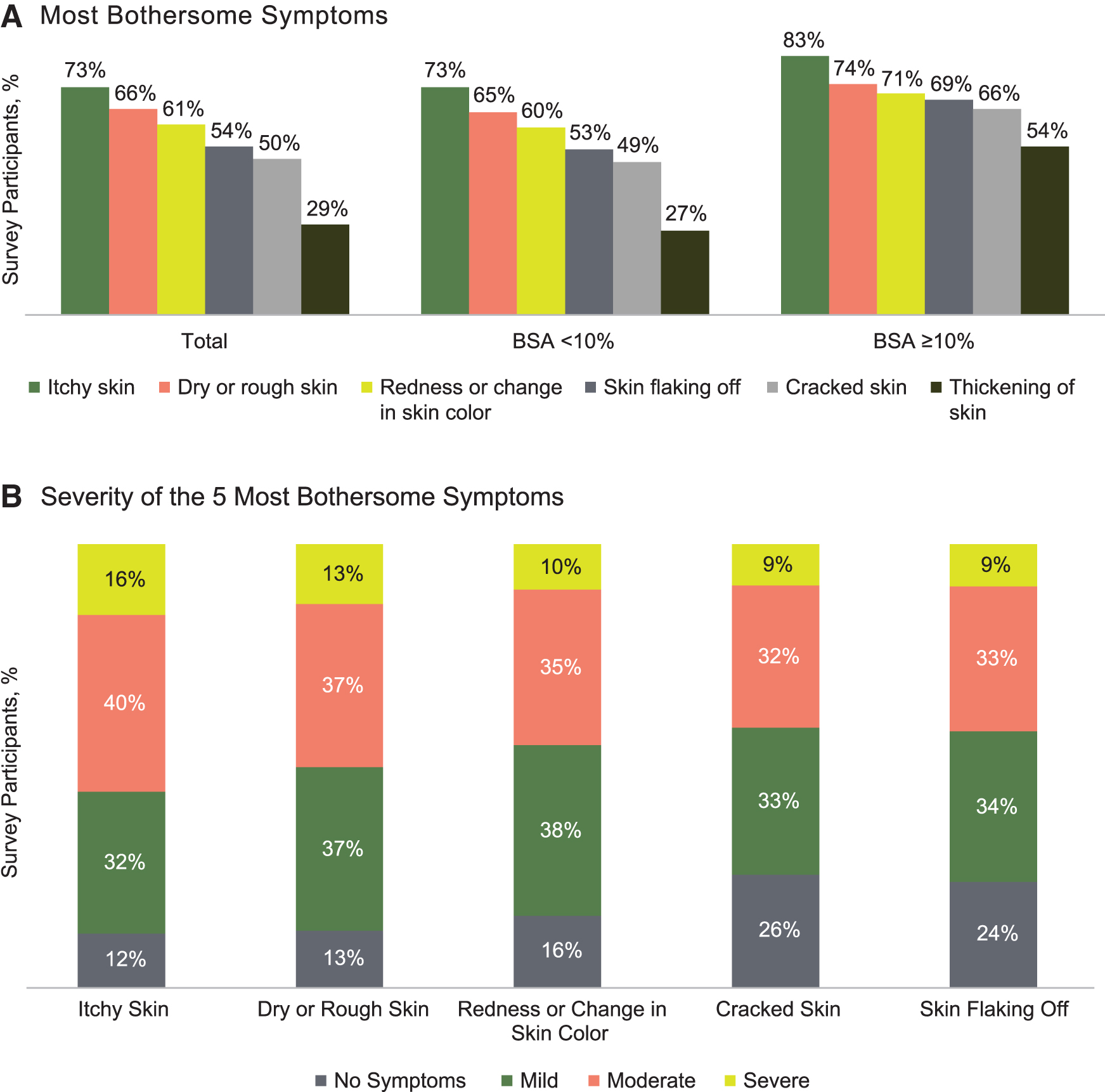
Itchy skin is the most frequently occurring and most severe symptom of AD. (A) Participants were asked: What types of symptoms, when active/present, do you typically experience due to eczema/AD? Itchy skin, dry or rough skin, redness or change in skin color, skin flaking off, cracked skin, or thickening of skin. (B) Participants were asked: In the past week, what is the intensity of the following due to your eczema? Bleeding, cracked skin, dry or rough skin, itchy skin, redness or change in skin color, skin flaking off, skin weeping or oozing clear fluid, swelling, thickening of skin, other, dryness (on healthy, unaffected skin), scratch marks or scarring. Only the top 5 symptoms are shown. AD, atopic dermatitis.
In a sum-of-ranks analysis, these same symptoms emerged as the most burdensome overall. In total, 1866 participants assigned a rank to itchy skin, with 40% ranking it as the most burdensome symptom and 62% ranking it in the top 3 most burdensome symptoms of AD (Fig. 3).

Itchy skin is also the most bothersome symptom of atopic dermatitis. Participants were asked: Please rank your symptoms in order from 1 to least, where 1 is the most bothersome and the last of the symptoms is the least bothersome. aSurvey Q317: Please rank your symptoms in order from 1 to LEAST where 1 is the most bothersome and the last of the symptoms is the least bothersome. bExplanation of the sum of ranks calculation: Assume that 4 symptoms are ranked. The number of times a symptom is ranked first is multiplied by 4; the number of times a symptom is ranked second is multiplied by 3; the number of times a symptom is ranked third is multiplied by 2; and the number of times a symptom is ranked fourth is multiplied by 1. Number of respondents who rank symptom first (eg, 24 × 4 = 96); number of respondents who rank symptom second (eg, 35 × 3 = 105); number of respondents who rank symptom third (eg, 46 × 2 = 92); number of respondents who rank symptom fourth (29 x 1 = 29). Calculate the sum of ranks by adding all the subtotals (eg, sum of ranks for symptom: 96 + 105 + 92 + 29 = 322).
Survey participants were asked to complete an Itch Numerical Rating Scale (I-NRS) and a Sleep NRS. In the prior week, most participants experienced itch intensity that was moderate or severe (no itch [0], 1%; mild [1–3], 14%; moderate [4–6], 36%; severe [7–10], 49%; Fig. 4A). Whereas a greater percentage of participants with BSA ≥10% ranked their itch as severe, most participants in both the low (83%) and higher BSA groups (98%) had NRS scores indicating moderate-to-severe itch. The mean past week I-NRS score was 6.1 (6.0 for participants with BSA <10% and 7.6 for participants with BSA ≥10%).

Itch and sleep numerical rating scale over the past week. (A) Participants were asked: On a scale of 0 to 10, where “0” is “No itching” and “10” is “Worst itching imaginable,” please select the number that best describes your worst level of itching due to eczema over the past week. (B) Participants were asked: On a scale of 0 to 10, where “0” is “Did not interfere” and “10” is “Completely interfered,” please select the number that best describes how much your itch has interfered with your sleep over the past week. NRS, Numerical Rating Scale.
Greater than 67% of patients reported that itch moderately to severely interfered with their sleep in the past week (Fig. 4B). Similar to itch, most participants with both low (67%) and higher (92%) BSA experienced moderate-to-severe sleep disturbance in the past week, with a larger proportion of the BSA ≥10% group falling into the severe category. The mean sleep NRS score in the past week was 5.1 (4.9 for participants with BSA <10% and 7.4 for participants with BSA ≥10%).
The most commonly reported locations for AD-related lesions (skin with noticeable rash in the past week) were forearms (30%), palms (27%), and face (24%). These were also the areas where experiencing itching was most commonly reported. In the past week, 27% of respondents reported itching on their forearms, 25% on the palms, and 20% on the face. Participants were further asked whether they experienced pain and/or itch on skin with and without visible rash; 93% reported that they experience itch (with or without pain) on skin with visible rash, and 65% said that they experience itch (with or without pain) on skin without visible rash (Fig. 5). Forty-five percent of respondents reported experiencing pain (with or without itch on skin with visible rash) and 31% experienced pain (with or without itch) even on skin without visible rash (Fig. 5).

Patients experiencing pain/itching in the past week. (A) Participants were asked: In the past week, have you experienced pain or itching on your skin where there is a visible eczema rash? Select one. (B) Participants were asked: In the past week, have you experienced pain or itching on your skin where there is no visible eczema rash? Select one.
Treatment-Seeking Behavior
The main reasons for the most recent visit to health care provider included itch (61% of participants), closely followed by visible rash/skin appearance (57% of participants; Fig. 6A). The most commonly reported specialty physicians visited were dermatologists (61% of participants), followed by primary care physicians (26% of participants).

Itch drives treatment-seeking behavior. (A) Participants were asked: Thinking back to that most recent visit for your eczema, what were the main reasons for seeking care? Select all that apply. (B) Participants were asked: We would now like to understand what is important to you when treating your eczema. Please rank your treatment goals for your eczema in order, where 1 is the most important, 2 is the second most important, and so on. Rank order as many as apply, but at least 3. HCP, health care provider.
Sum-of-ranks analysis found that survey participants considered reducing itching to be the most important treatment goal (Fig. 6B). Most participants (85%) were currently using topical treatments for their AD, with 46% using a prescription topical medication. Only 22% of survey participants were currently using a prescription oral medication, and 17% were using a prescription injectable medication (Fig. 7A). Use of systemic treatments was higher among participants with BSA ≥10% compared with those with BSA <10% (Fig. 7B). Participants generally reported lower satisfaction with topical therapies and greater satisfaction with systemic therapies across all measured treatment domains (among those reporting current use of each; Fig. 8).

Treatment usage of eczema patients. Participants were asked: What type of treatments, over-the-counter and/or prescription, are you currently using or have used in the past to treat your eczema? (A) Treatment use and history in the full participant population. (B) Current treatment use by body surface area. OTC, over-the-counter.

Treatment satisfaction of eczema patients. Participants were asked: On each of the following attributes, how would you rate your satisfaction with the treatment(s) you are currently using to treat your eczema? Select 1 for each row. Participants were probed on satisfaction only for those classes of therapies for which they reported current use. The percentages shown are for survey participants who responded “very” or “extremely” satisfied. BSA, body surface area; OTC, over the counter.
DISCUSSION
The vast majority of participants had a diagnosis of mild-to-moderate AD as defined by BSA (<10%) and POEM. This is consistent with previous reports that most adult AD is mild to moderate in severity.2,16 Despite low BSA involvement, participants reported a range of symptoms with severity ranging from mild to severe. Participants with AD reported itch as the most common and bothersome symptom of their disease, regardless of the overall severity of their AD, a finding consistent with published literature describing the burden of itch in patients with AD.8,17
Nearly all of the participants with BSA ≥10% reported moderate-to-severe itch and sleep disturbance. Of note, however, is that >83% of participants with BSA <10% group also reported moderate-to-severe itch, and two-thirds had moderate-to-severe sleep disturbance in the past week.
Most respondents were using topical treatment, with only a minority reporting current use of prescription systemic medications. Despite reporting lower mean past week itch and sleep NRS scores and less skin involvement, participants with lower BSA involvement were less satisfied with their current treatment than were the participants with higher BSA. The reasons for this discrepancy are unknown, but the difference in satisfaction is apparent across all domains, including the ability to improve itch, sleep, and skin appearance and condition.
It could be that patients with lower BSA are less likely to seek health care or receive systemic therapies to fully address their disease burden. Indeed, previous research has shown that less frequent office visits are associated with lower patient treatment satisfaction, whereas systemic therapy managed by a specialist is associated with greater treatment satisfaction. 18
In this survey, 65% of participants said they experience itch, with or without pain, on skin without visible rash. Such itch may be difficult to treat with topical therapies, application of which may be limited to areas with lesions. As treatment satisfaction with topical therapies was low, particularly in the group with BSA <10%, it may be more appropriate to address itch with systemic therapies. Itch is known to be negatively correlated with QoL in patients with AD. For many of these survey participants, their itch was severe enough to cause interference with sleep. In addition to adverse effects on sleep, itch has adverse effects on participation in activities, clothing choices, and social interactions in children and young adults with AD. 3
Pain was also a fairly common symptom reported by the respondents, with 31% experiencing pain even on skin without visible rash. As only a small minority of patients report pain but not itching, it is tempting to speculate that pain in AD may occur, at least occasionally, as a sequela of itching. Previous reports have identified pain as a frequent symptom of AD that tends to correlate more strongly with other AD symptoms (eg, itch, QoL) as opposed to outward signs of AD (eg, Eczema Area and Severity Index).19–21
Although it is possible for pain in AD to occur separately from itching and scratching, pain is more commonly reported by patients with excoriations, and a subset of patients experience a seemingly neuropathic pain emerging from the itch itself. 22 Pain should not be overlooked as a patient symptom and may be alleviated by therapies that effectively control pruritus and/or scratching behavior.
Although drug development to date has focused mostly on medications for improving skin lesions, our survey participants identified improving itch as their top treatment goal and primary reason for AD-related health care utilization. 23 Alleviating itch is crucial to improving patient QoL and may control the itch–scratch cycle, which consists of continuous scratching, irritation, itching, and subsequent scratching. 23 If patients with AD are not treated adequately, the itch–scratch cycle may become chronic with more severe consequences, as damage to the skin barrier through continued scratching worsens the uncomfortable itch sensation, further exacerbating skin injury and inflammation, and potentially leading to infection.5,24
This survey highlights an unmet need for antipruritic therapies, particularly systemic therapies that could directly reduce itch in both lesional and nonlesional skin. This treatment gap may be especially relevant to patients with more limited BSA involvement.