
Abstract
Capsule Summary
Stasis dermatitis (SD) is associated with a significant burden of disease, with debilitating symptoms such as pain, swelling, and itching leading to poor sleep, loss of mobility, and the inability to participate in work and leisure activities.
Serious secondary complications such as skin ulceration can increase patient morbidity and mortality, reduce quality of life, and increase health care costs.
Diagnosis can be challenging due to poor recognition among general practitioners and the clinical resemblance of SD to other skin conditions, predominantly cellulitis and allergic contact dermatitis.
INTRODUCTION
Characterized by pruritus, sore or painful skin, swelling, and skin discoloration, stasis dermatitis (SD), an inflammatory dermatosis of the lower extremities, leads to a substantial disease burden.1–3
Patients typically present with poorly demarcated erythematous and eczematous patches and plaques on the lower leg, usually the medial malleolus. Dermal deposition of hemosiderin, the breakdown product of hemoglobin from red blood cells, can lead to hyperpigmentation and persistent discoloration of the affected area (Fig. 1A, B).4,5 These visual symptoms associated with SD result in a negative self-image, adding to the psychological burden of disease. 5

Presentations of SD. (A) SD usually begins on the inside of the ankles, causing dry, discolored, and itchy skin. Reprinted with permission from Dr. Adam J. Friedman, George Washington School of Medicine and Health Sciences, Washington, DC, USA. (B) Classic hyperpigmentation and varicosities of SD. There is inflammatory eczematous change overlying the medial ankle, with healed scarring from recent ulceration. Reproduced with permission from Medscape. 4 (C) Lipodermatosclerosis observed in SD. Reprinted with permission from Dr. Mark G. Lebwohl, Icahn School of Medicine at Mount Sinai, New York, NY, USA. (D) SD with erythema. Reprinted with permission from Dr. Takashi Hashimoto, Department of Dermatology, National Defense Medical College, Saitama, Japan. (E) Varicose veins. Reprinted with permission from Science Photo Library. (F) Venous stasis ulcer. Inadequately treated SD may rapidly progress to a venous stasis ulcer. Reprinted with permission from Science Photo Library. (G) SD with extensive venous leg ulcerations. Reprinted with permission from Dr. Takashi Hashimoto, Department of Dermatology, National Defense Medical College, Saitama, Japan. SD, stasis dermatitis.
SD may progress to conditions such as lipodermatosclerosis (Fig. 1C) and leg ulcerations5,6 that place an additional burden on patient quality of life (QoL) and on the health care system due to additional costs associated with the treatment and management of these complications.7,8 The recurrence of SD and secondary venous ulcers after the resolution of symptoms remains a problem irrespective of the type of treatment used, often leaving patients feeling despondent. Although the recurrence of venous ulcers has been reported to be greater in patients treated nonsurgically,9–11 recurrence rates of venous ulcers after surgery of ∼20–40% have been reported.9,12–14 In 500 patients with chronic venous insufficiency (CVI) randomly assigned to receive either surgery plus compression therapy or compression therapy alone, a recurrence rate at 4 years of 56% for the compression group and 31% for the compression plus surgery group was reported. 14
CVI affects a significant proportion of the elderly population, with prevalence increasing with age, likely due to increased pressure on superficial veins arising from weakening of calf muscles and deterioration of vessel walls. 15 Estimates of geographic prevalence vary widely in the different population studies reported, with the highest reported in Western countries and a lower number among Asian populations.15–17 According to a study based in the United Kingdom, minor stigmata of venous disease was present in half of the adult population. 18
In the United States, the prevalence of SD has been estimated at 6% in patients older than 50 years, equivalent to 15 to 20 million patients, thereby making it twice as prevalent as psoriasis.4,19 Overall, an estimated 2% of the global health care budget is consumed by CVD care and treatment. With the increasing age of several population groups, the rising rates of obesity, and more-sedentary lifestyles and occupations, the prevalence of SD and more serious forms of CVI, and the associated burdens are expected to increase.15,16,20
Patients with SD not only experience a significant burden arising from the disease and its complications but also face additional challenges during the process of effectively managing their disease. Here we review the burden of SD associated with diagnostic challenges, signs and symptoms, complications, and treatment.
DIAGNOSTIC CHALLENGES
Early diagnosis and treatment of CVI may prevent disease-related complications; however, patients often delay seeking medical attention until the disease progresses and those patients seeking medical attention may encounter several diagnostic challenges. SD is often diagnosed based on the physical appearance of the affected skin and the patient's medical history. An initial examination typically reveals erythema and eczematous patches, which are usually found on the lower legs (Fig. 1D). Such symptoms usually involve the medial ankle, and in advanced cases, the inflammation may extend almost to the knee.5,21,22 Other symptoms can include pruritus, restless legs, cramping, tingling, swelling, and other presentations of CVD; hyperpigmentation due to dermal deposition of hemosiderin is often present.5,21,22 Progression of SD may result in pain, oozing, and ulcerations resulting in an increased burden on the patient.
In addition to the diagnostic challenges outlined above, the dermatological changes typical of SD may resemble those of other skin diseases (Table 1),5,22–25 leading to inaccurate diagnosis, delayed or incorrect treatment subsequently increasing patient anxiety and financial burden. Cellulitis is commonly confused with SD; ∼10–30% of patients hospitalized for cellulitis were misdiagnosed, with SD being the most common correct diagnosis.26,27 In contrast to SD, cellulitis usually presents unilaterally with tenderness in the involved area; is often accompanied by fever, chills, tachycardia, and elevated white blood cell count; and is responsive to intravenous antibiotic treatment (Table 2).5,22,28
Conditions That Mimic Stasis Dermatitis
Features of Stasis Dermatitis and Lower Limb Cellulitis
TCIs, topical calcineurin inhibitors; TCSs, topical corticosteroids.
Because cellulitis is a potential medical emergency, this misdiagnosis can lead to unnecessary hospitalization and antibiotic exposure, which may place patients at risk for complications, including rash, gastrointestinal upset, diarrhea, repeat visits to the emergency department, and hospital readmission. 27 In total, 84.6% of patients mistakenly diagnosed with cellulitis did not require hospitalization and 92.3% received unnecessary antibiotics, increasing the financial burden on the health care system. 27 Unnecessary use of antibiotics has been estimated to result in >9000 nosocomial infections and between 1000 and 5000 Clostridium difficile infections. 27
The misdiagnosis of lower extremity cellulitis has been estimated to lead to 50,000–130,000 unnecessary hospitalizations and $195 million–$515 million in avoidable health care costs. 27 In addition to the financial implications of these admissions, health care professionals are also put under additional burden due to the increased number of patients requiring time and resources both within the emergency department and other general wards.
Early consultation with a dermatologist improves diagnostic accuracy and outcomes among hospitalized patients with inflammatory diseases.29,30 In patients admitted with presumed cellulitis, 30.7% were misdiagnosed, and among those patients 26% were diagnosed with SD after dermatology consultation. 31
Allergic contact dermatitis is another cutaneous disorder commonly mistaken for or complicating SD. A thorough physical examination and a history of using topical medications, emollients, cleansers, and other products may help plan patch testing that can differentiate between the 2 conditions. However, a differential diagnosis can be complicated because allergic contact dermatitis can occur on a background of SD due to the breakdown of the skin barrier and frequent exposure to topical treatments that can contain sensitizing components. Patch testing is needed to identify the allergen. 22
Early diagnosis and treatment of CVI may prevent disease-related complications. However, patients often delay seeking medical attention until the disease progresses. The misdiagnosis and consequent undertreatment or incorrect treatment are confounded by the fact that SD is underrecognized within the health care system. Moreover, SD lacks a definite International Classification of Diseases (ICD) code, which complicates the study of disease burden. On average, a patient may see an average of 6.9 doctors for this condition, often due to patients lacking the resources or knowledge needed to adhere to compression therapy rather than misdiagnosis. 32
When comparing the outcomes of patients whose care was guided by an order set for SD (ie, providing patient and family education on the role of compression in treatment, physical therapy consultations to provide fittings for gradient compression stockings and to assess the need for assistive devices, and providing information on how to obtain additional replacement stockings), there was a significantly lower readmission rate compared with those admitted without an order set (4.17% vs 20.27%; P = 0.039). 32
SIGNS AND SYMPTOMS ASSOCIATED WITH SD ARE TROUBLESOME AND IMPACT PATIENT QUALITY OF LIFE
The symptoms of venous insufficiency can be debilitating, compromising the ability of patients with SD to lead a normal life. As venous insufficiency progresses, pain and discomfort intensify and limit many physical activities. Patients have reported that symptoms worsen at the end of the day, at night, and after prolonged standing. 33 Night-time pain in patients with venous ulcers leads to sleep disturbances, causing patients to feel tired and lacking in energy. 8 In a study of 600 patients, chronic leg ulcers limited mobility in 11% of patients and interfered with work and leisure activities to a moderate-or-severe degree in 42% of patients, placing a financial and social burden on the patient and society. 34
Edema of the lower legs may limit physical activity due to associated pain and decreased ankle range of motion. Severity of edema is further precipitated by decreased mobility that can result in a cycle of worsening edema.35,36 Lack of improvement and limitations on daily activities result in an increased burden on the patient and caregivers.
Itch is another troublesome symptom reported frequently by patients with SD that also interferes with sleep and concentration. Scratching the already impaired skin can further increase the risk of secondary infection and wound aggravation. 1 More than half (66%) of patients with mild-to-moderate CVI reported that itch had been present for a median duration of 7.8 years. In almost half of patients, itch was a daily occurrence, with each occurrence lasting an average of 9 hours daily. 37 In another study of patients with CVD, 55% experienced itch, with 19% rating the itch as unbearable. 1
Itching was more frequent during the evening and night, leading to sleep disturbances and increased use of medications for sleep. The itch and the burning sensation and pain that accompanied itch lowered patients' QoL (Table 3).1,37 The itching in SD is nonhistaminergic and caused by inflammatory mediators liberated in the microcirculation, including interleukin-31, a pruritogenic cytokine that is also involved in other inflammatory skin conditions characterized by itching. 38 The use of antihistamines does not, therefore, provide relief in SD-related itch. High- or mid-potency topical corticosteroids (TCSs) are thus used; however, long-term use is not advised because of local and systemic side effects.22,38
Analysis of the Difference in Itch on Lower Limbs in Relation to Quality of Life, Comorbidities, and Leg Pain (Analysis of Variance)
Adapted from Paul et al. 1
The SF-12 consists of 12 questions from the 36-Item Short Form Survey quality of life questionnaire that measure physical and mental health.
NS, not significant; SF-12, 12-Item Short Form Survey.
Varicose veins are not only a cosmetic concern but can also cause discomfort, pain, loss of working days, and disability (Fig. 1E). 39 The QoL among patients with uncomplicated varicose veins (C2 disease) is reduced compared with that of the general population, particularly because of poorer physical functioning, limitations due to physical problems, and pain. 40 However, reduced physical QoL among patients with varicose veins is often associated with concomitant venous insufficiency and not necessarily the varicose veins. 41
Varicose veins also constitute a substantial financial burden. In a claims-based study, 2-year treatment costs per patient (standardized to 2012 US dollars) after a diagnosis of varicose veins ranged from $204 for conservative management (surveillance and compression) to $5836 for multiple interventional modalities. The same study showed high recurrence rates, with >50% of patients requiring additional interventional treatment with the same or a different modality during 2 years of follow-up. 3
COMPLICATIONS CAN INCREASE PATIENT MORBIDITY
Many patients do not understand that CVI (with or without SD) is a progressive disease that can lead to complications that significantly increase morbidity and mortality. Indeed, patients with mild SD are often unaware of underlying CVI. Longitudinal studies show that the rate of progression to venous ulceration in patients with skin changes was estimated to be 1–2% per year. 42 It has been estimated that ulcers due to venous insufficiency affect 1% of the adult US population. 43 The QoL of patients with ulcerations from venous insufficiency is poor and has been reported to be comparable with that of patients with congestive heart failure or chronic lung disease. 44
More than 60% of ulcers last >6 months and 20% last for >5 years; recurrence rates are also high, at ∼45%. 45 Venous leg ulcerations (Fig. 1F, G) are associated with a range of incapacitating symptoms. Patients with leg ulcers have described their pain as relentless, stabbing, and interfering with sleep; the inability to relieve pain with analgesics can be frustrating.7,45 Improved pain control is important because a lack of pain relief may result in the overuse of analgesics. The negative psychological impact of these ulcers on patients resulted in anxiety, depression, and even suicidal thoughts. 7 Patients reported feeling frustrated and disheartened when ulcers did not heal or recurred after healing.7,45 The economic burden of direct health care costs for venous leg ulcers to US payers has been estimated at ∼$15 billion. 46
COMPLICATIONS CAN INCREASE HOSPITAL COSTS
Although some patients with SD typically have their care managed in the dermatologist's office, admission to the hospital is common if a patient's SD becomes exacerbated or if the discomfort of itch and swelling is too difficult to manage at home. 4 In the United States, the mean incidence of CVI-related hospital admissions is 92 per 100,000 patients. 47 Because SD is a chronic disease and many patients have difficulty adhering to treatment regimens, readmissions may be frequent, increasing the burden on the health care system. Between 2007 and 2011, Medicare patients with venous leg ulcers had 0.7 (77.8%) more days of hospitalization and privately insured patients had 3.2 (88.9%) more days of hospitalization, compared with matched patients without ulcerations due to venous insufficiency over a 12-month period. 46 The presence or absence of SD in the patients included in this study was not indicated. 46 Inpatient costs comprised 18.2% and 48.3% of the overall excess per patient cost for Medicare and privately insured patients, respectively. Infections add to the economic burden of venous ulcers. 46 A retrospective single-center study reported that 11.5% of patients with a venous leg ulcer required ≥1 inpatient admission for infection over a 1-year period; total cost of treatment for a patient hospitalized for infection was ∼2.5-fold higher than for a patient without infection ($27,408 vs $11,088). 48
TREATMENT AND PATIENT ADHERENCE
The main goal of treatment in patients with SD is to minimize the clinical impact of the underlying venous insufficiency (namely, to reduce pain and discomfort), relieve pruritus and edema, improve skin changes, and heal any associated ulcers. Initially, conservative approaches are frequently used, which must include compressions and, in some patients, adjunctive leg elevation, exercise, management of weight, and adherence to a low-salt diet (a low-salt diet reduces fluid buildup and associated edema).22,36
However, maintaining lifestyle changes is difficult, and patient adherence is poor. Exercise increases the movement of the ankle joint and strengthens the muscle pump in the calf muscles, thereby improving hemodynamics and preventing disease progression. However, the efficacy of exercise for patients with nonulcerated disease has not been clearly established, and the effectiveness of an exercise program is often dictated by adherence. In patients with venous leg ulcers, ∼40% of patients did not adhere to the program, underscoring the difficulty of self-management. However, patients who adhered to the exercise program had faster healing rates versus nonadherent participants. 49
Compression therapy with stockings or bandages remains the cornerstone of treatment for venous diseases. 50 A systematic review reported that compression increased the rate and rapidity of ulcer healing compared with no compression and also improved pain. 51 Support stockings can ameliorate symptoms of pain, swelling, and stasis skin changes in CVD. It is important that arterial insufficiency be excluded before application of compression because compression on a leg with compromised arterial circulation can increase claudication and the risk of ischemic damage.5,52 Although compression is considered effective therapy, it is also the most difficult to self-manage.5,22
In a study of >3100 patients with CVD referred to a tertiary venous practice between 1998 and 2006, only 37% of patients were fully or partially adherent with stocking use (Fig. 2); adherence was low (<50%) regardless of Clinical (C), Etiological (E), Anatomical (A), and Pathophysiological (P) classification or symptoms (pain, swelling, stasis ulcer, or SD). 52 Reasons frequently mentioned by patients for not using compression therapy included discomfort from legs heating up, especially in hot and humid weather; poor fit leading to excessive compression; and exacerbation of itching. 52
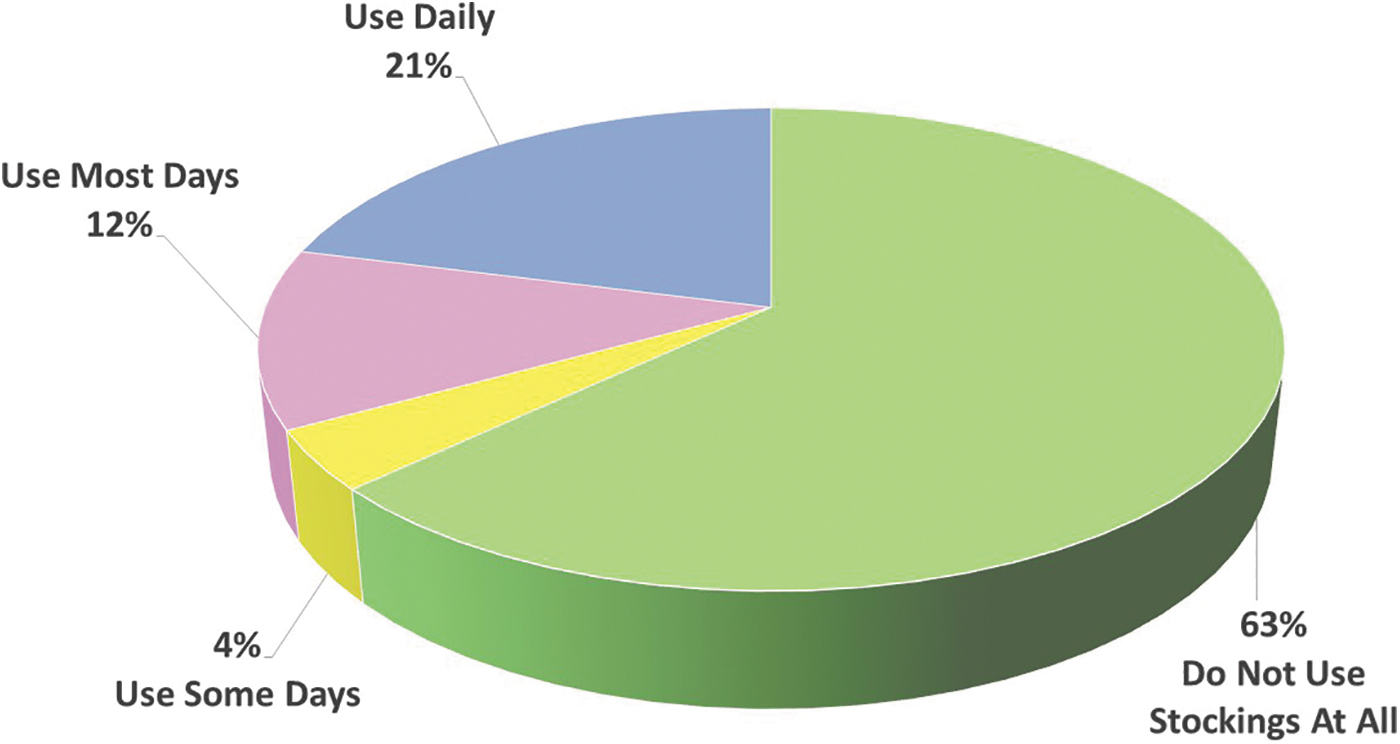
Use of compression stockings among 3144 patients with chronic vascular insufficiency. Reproduced with permission from Raju et al. 52
One major barrier to routine use of compression stockings reported by both patients and caregivers was decreased mobility and the difficulty and daily struggle of putting them on, particularly among elderly and obese patients. This often results in an additional burden on caregivers who may often feel overwhelmed due to their lack of skill or training.52,53
The cost of prescription-grade stockings was also a financial burden on patients without health insurance, often leading to continued wear even after the compression was weakened and thus ineffective.54,55 The daily routine of stocking wear restricted some patients' lifestyle, and some patients felt self-conscious and had body image concerns related to compression. 55
If required, high-level compression can be achieved with professional application of elastic bandages, paste boots or pneumatic compression devices. Application requires attention from a wound care expert for dressing changes, which becomes burdensome because of transportation issues; it also interferes with work schedules.45,55,56
The effectiveness of compression bandages is also predicated on the training and skills of the operator and the application technique; the performance of a bandage in a laboratory setting and in clinical use may not always be similar.51,56 It is important to inform patients that compression therapy should be continued even after healing has occurred to prevent recurrence of dermatitis and ulcers, as many patients are unaware of the consequences of nonadherence and discontinue the use of compression once the ulcer heals. 55
Adherence of patients with compression therapy is closely linked to their understanding and motivation to wear the compression product consistently; however, constraints on clinicians' time and reimbursement issues have been a barrier to more effective communication. 57 Adherence to the use of compression therapy could be potentially improved by educating patients regarding the correct fitting, usage, and application of stockings or bandages for the treatment of SD. Although the rate of adherence is higher with stockings than with bandages, bandages have displayed higher efficacy for alleviating SD symptoms. However, bandages are more challenging to use and, hence, require expertise for correct application. The use of donning devices could aid patients in correctly applying stockings on their own. 5
The cost of prescription-grade stockings was also a financial burden on patients without health insurance, often leading to continued wear even after the compression was weakened and thus ineffective.54,55 The daily routine of stocking wear restricted some patients' lifestyle, and some patients felt self-conscious and had body image concerns related to compression. 55
Interventional options for CVI are available if conservative measures are not effective, with a variety of surgical methods being used to correct the underlying cause of reflux and increased venous pressure.5,9 These include minimally invasive venous procedures such as endovenous thermal ablation, ambulatory phlebotomy, and ultrasound-guided foam sclerotherapy. These newer procedures have advantages over the previously open procedures, including less postoperative pain, lower incidence of complications, faster recovery, and greater cost efficacy.5,9
A focus on diagnosing and managing venous insufficiency can overshadow and minimize the need for more direct dermatological care of SD in addition to the vascular care. However, there is no approved pharmacological intervention specifically for SD. Topical treatment for SD, which is in common with treatment for other forms of eczematous dermatitis, includes the use of mid-potency corticosteroids such as triamcinolone acetonide and topical calcineurin inhibitors (TCIs) such as pimecrolimus and tacrolimus to reduce inflammation and itching.22,58–60
Prolonged use of high-potency corticosteroids should be avoided because of the risk of skin atrophy, whereas TCIs may cause application site burning pain and have a boxed warning for rare cases of malignancy (eg, lymphoma), although no causal link has been confirmed.22,58–60 Corticosteroids can also lead to contact sensitization in patients with SD. 61 Systemic treatment options derived from therapy options used to treat CVI include acetylsalicylic acid, flavonoids, pentoxifylline, and horse chestnut seed extract, which minimize inflammation and improve circulation.22,62–66
Because inflammation is key in the cutaneous manifestations of SD, treatment directed at inhibiting inflammatory processes may provide an additional approach to reducing signs and symptoms of SD. Phosphodiesterase 4 is an intracellular nonreceptor enzyme that modulates inflammation, and crisaborole, a topical phosphodiesterase 4 inhibitor approved for the treatment of atopic dermatitis in multiple countries, is currently under evaluation in adults with SD in a phase 2 trial (NCT04091087). 67
CONCLUSIONS
SD is an advanced cutaneous presentation of CVI and is more commonly reported in older patients. The common symptoms of CVI and SD, including pain, swelling, and pruritus, can be debilitating and lead to poor sleep; lack of mobility; and a profound effect on patients' daily physical, emotional, and social functioning. Loss of independence as well as the socioeconomic impact of SD secondary to these symptoms are factors affecting not only the lives of these patients but also of their families.
The diagnosis of SD is complicated by its clinical similarity to other dermatological conditions. Misdiagnosis may lead to hospitalization, the use of unnecessary antibiotics, and delays in initiating appropriate treatment. Consequently, time and resources of both patients with SD and the health care system are wasted.
Amelioration of the signs and symptoms of SD such as by leg elevation during hospitalization does not ensure permanent resolution of the disease. Lack of improvement and recurrence can be demoralizing for the patient. With no pharmacological agents other than TCSs currently approved for the treatment of SD, there is a need for more targeted therapeutic alternatives having minimal adverse effects and improved long-term control. In the future, targeted treatment options may lead to improved therapy-related outcomes in patients with SD.
Treatment of SD is focused on alleviating symptoms and preventing complications; however, adherence is always an important factor to consider in the management of these patients. Compression therapy, which forms the cornerstone of treatment, is effective in relieving pain and swelling and healing ulcers; however, patient adherence is typically poor. With no pharmacological agents other than TCSs currently approved for the treatment of SD, there is a need for targeted therapeutic alternatives having minimal adverse effects and improved long-term control.
In the future, targeted treatment options may lead to improved therapy-related outcomes in patients with SD. Effective, safe, and user-friendly treatment options together with more accurate and timely diagnosis of SD in the future are essential in reducing the burden of disease.