
Abstract
Depression and anxiety can significantly reduce the effectiveness of cardiac rehabilitation (CR). Several studies have assessed the effectiveness of virtual reality (VR)-based interventions for symptoms of anxiety and depression; however, they do not relate to patients with heart disease. The aim of this study was to assess the effects of VR therapy on the mental state of patients with coronary artery disease (CAD). Thirty-four CAD patients with elevated anxiety or depression symptoms were recruited. After randomization, 17 participants were assigned to the intervention group, and 17 to the control group. Both groups underwent standard CR for outpatients. In the intervention group, eight VR therapy sessions were applied. In the control group, eight sessions of Schultz’ Autogenic Training were applied. To assess patient mental states, Hospital Anxiety and Depression Scale (HADS) and Perception of Stress Questionnaire (PSQ) were used, before and after 4 weeks of CR. In the intervention group, a significant decrease in HADS score was observed (19.46 pretreatment vs. 15.73 post-treatment, p = 0.003), HADS-Anxiety subscale decreased by 16.0 percent (p = 0.01) and HADS-Depression by 23.0 percent (p = 0.003). Similarly, a significant decrease in PSQ was recorded at 12.8 percent (64.73 vs. 56.47, p = 0.03). In the control group, HADS and PSQ data did not change. VR therapy significantly reduced the severity of depressive symptoms, anxiety, and stress levels in CAD patients undergoing CR. Immersive VR therapy effectively supports the CR of individuals with anxiety-depressive symptoms.
ClinicalTrials.gov (NCT04045977)
Introduction
Cardiovascular disease (CVD) includes all heart and vascular diseases and is the leading cause of death, disability, and disease burden in the developed world. 1 Several studies indicate that depression and anxiety symptoms are among the psychological factors associated with the development of CVDs.2,3 Over the past 25 years, research has found that not only is depression more common in cardiac patients, when compared with the general population, but it is also a risk factor for cardiac morbidity and mortality, independent of traditional risk factors. Coronary artery disease (CAD) refers to the atherosclerosis of blood vessels supplying blood to the heart, and CAD is the cause of myocardial infarction (MI). Between 31 and 45 percent of CAD patients suffer from clinically significant depressive symptoms. 4
A high proportion of depressed CVD patients suffer from a comorbidity anxiety disorder. 5 Anxiety is independently associated with increased mortality in CAD patients, particularly in the presence of comorbid depression. The presence of anxiety early after an acute cardiac event can predict the later development of depression. 5 The authors showed that anxiety disorders were associated with an elevated risk of a range of different cardiovascular events, including stroke, CAD, heart failure and cardiovascular death. 6 The meta-analysis published by Batelaan et al. comprised 37 studies with 1,565,699 participants, and showed that anxiety was associated with a 52 percent increased incidence of CVD (hazard ratio = 1.52, 95 percent CI 1.36–1.71). 7 In their literature review, Chalmers et al. revealed that anxiety disorders are associated with significant reductions in heart rate variability, suggesting this may be one of the mechanisms linking anxiety disorders to CVD. 8
Cardiac rehabilitation (CR) is an essential component in the comprehensive management of cardiac patients. 9 During the first stage of CR, the main goal is to restore self-reliance in basic activities of daily living. For the second stage of CR, it is extremely important to improve the physical capacity of the patient, and to reduce levels of negative emotions (anxiety, mood disorders, and stress) caused by cardiac events and cardio-surgical interventions, as well as reducing the impact of psychological factors that led to disease development. 10 Successful completion of the second stage of CR should significantly improve patient quality of life, and should ignite and strengthen the need for changes in lifestyle. 9
Depression and anxiety are likely to persist despite cardiac treatment and rehabilitation. 10 Therefore, psychiatric symptomatology should be determined as early as possible, to provide patients with additional therapeutic support. Otherwise, the positive effects of expensive specialist cardiac procedures can be diminished. These observations were verified during an 8-year study on patients who underwent a successful coronary artery bypass grafting, yet did not undergo psychiatric treatment or therapy. 11 Therefore, there is a need to determine efficient methods for managing depression and anxiety in CAD patients.
The recent literature reviews evaluated the effectiveness of virtual reality (VR)-based interventions for symptoms of anxiety and depression.12–14 In the Fodor et al. meta-analysis, the 39 randomized-controlled trials (RCTs) that included 869 participants compared a VR intervention with a control group or an active psychological intervention for adults. The most frequent mental condition was anxiety (31 studies). The most frequently used VR intervention was VR-enhanced exposure (21 studies), followed by VR-enhanced cognitive behavioral therapy (19 studies). The most frequently used VR device was the head-mounted display (35 studies). The authors concluded that VR-enhanced interventions had moderate to large effects, when compared with control conditions, and they could be an effective choice for clinicians and patients. 12 However, no article analyzed in the reviews mentioned above focused on patients with cardiac diseases. This gap in the literature therefore prompted this study, which evaluated how VR therapy affected the intensity of depressive symptoms as well as anxiety and stress levels in CAD patients who had undergone CR.
Materials and Methods
Design and participants
The study was conducted at a cardiac clinic, which provided the second stage of CR. Based on Whitehead et al. sample size for a pilot randomized trial guideline, the study included 34 patients. 15 The study was designed as a parallel-group RCT (Fig. 1). The design follows the recommendations for the second phase (VR2) of clinical trials in health using VR, focusing on acceptability, feasibility, tolerability, and initial clinical efficacy. 16 Patients were randomly assigned to receive CR combined with eight sessions of VR therapy (intervention group, n = 17), conducted twice a week for 20 minutes, or CR combined with eight sessions of standard relaxation technique 17 (control group, n = 17), conducted twice a week for 20 minutes. Table 1 presents patient baseline characteristics. Study attendance was entirely voluntary, the patients provided written consent to participate and were informed beforehand that they could leave the program at any given moment, without consequences to their clinical care. The study was granted ethical approval by the Scientific Research Ethics Committee (reference number: 31/2019) at the University of Physical Education in Wroclaw, Poland in June 2019 (NCT04045977).
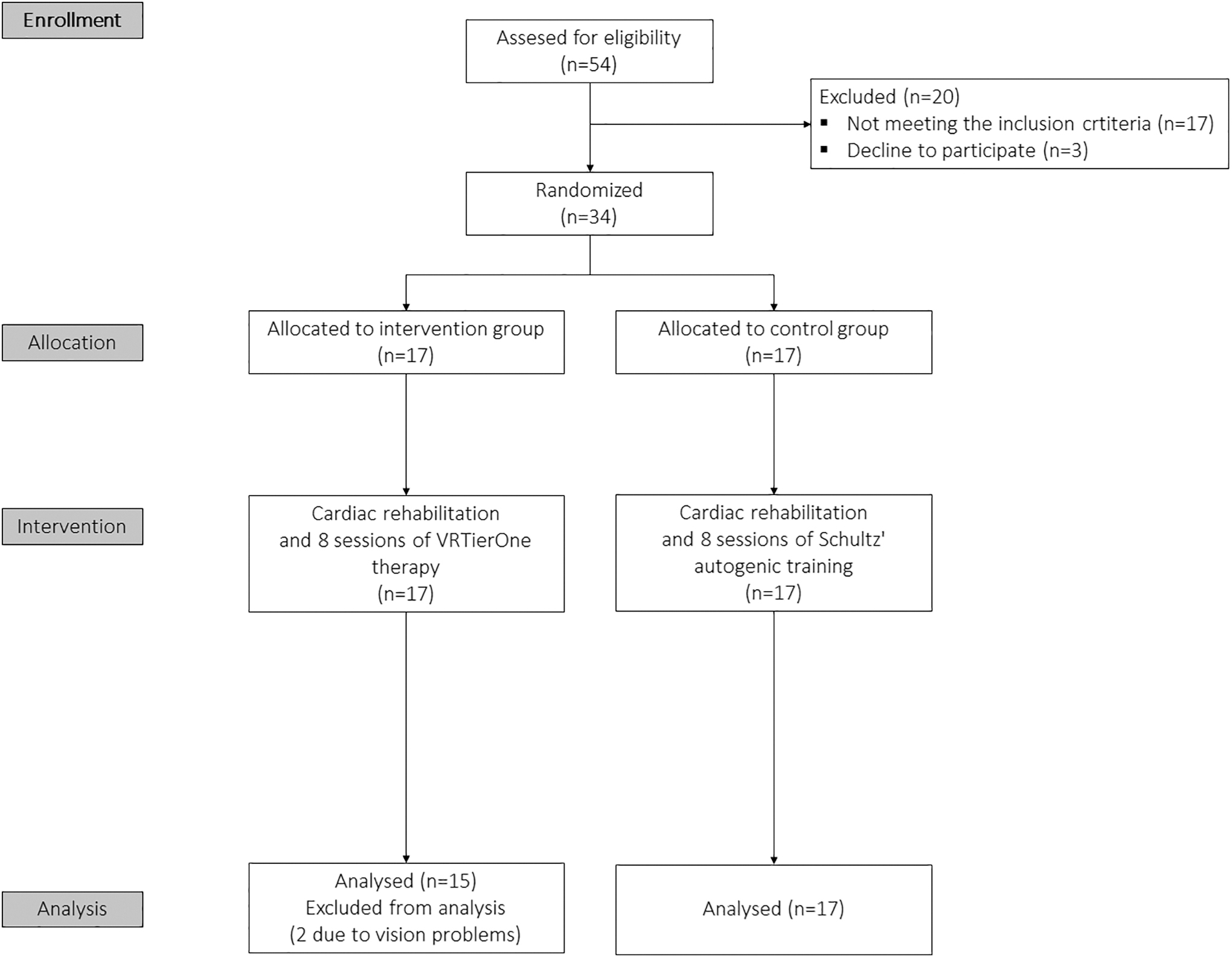
Study flow diagram.
Participants' Baseline Characteristics
BMI, body mass index; SD, standard deviation.
Inclusion criteria were as follows: CAD patients undergoing the second stage of CR in ambulatory conditions, anxiety symptom scores of 8 and higher in the Hospital Anxiety and Depression Scale (HADS), HADS-Anxiety (HADS-A) or depressive symptoms scoring 8 and higher in HADS, HADS-Depression (HADS-D), and aged 60–80. Exclusion criteria were as follows: cognitive impairments preventing self-completion of research questionnaires, the presence of the following issues at the time of the examination or in the medical records: disturbances of consciousness, psychotic symptoms, bipolar disorder or other serious psychiatric disorders, initiation of psychiatric treatment or individual psychological therapy during the research project, contraindications for virtual therapy (epilepsy, vertigo, eyesight impairment), and the patient's refusal to participate at any stage of the research project.
Outcome measures
As a primary outcome measure, HADS was used. It is a 14-item scale scoring from 0 to 3 for each item. Seven items related to anxiety (HADS-A), while the remaining seven related to depression (HADS-D). The global scoring ranged from 0 to 42, with a cutoff point of 8/21 for anxiety, and 8/21 for depression. The higher the score, the greater the anxiety or depression symptoms. 18 According to the authors, Cronbach's alpha ranges from 0.78 to 0.93 for the HADS-A, and from 0.82 to 0.90 for the HADS-D, and test/retest correlations were r = 0.80. 19
As a secondary outcome measure, the Perception of Stress Questionnaire (PSQ) was used. This questionnaire was created by Plopa and Makarowski and is a 27-item scale, scoring from 1 to 5 for each item. 20 Twenty-one items examined the level of stress in the areas of emotional tension, external stress, and intrapsychic stress, and 6 items referred to the lie scale. The global scoring for the perception of stress ranged from 21 to 105, with a cutoff point of 60 for elevated levels of perceived stress. The higher the score, the greater the sense of stress. According to the authors, Cronbach's alpha for the individual scale ranged between 0.69 and 0.80. 20
In addition, all patients filled in a questionnaire pertaining to their sociodemographics, such as age, sex, education, and marital status. They also answered questions on how they judged their own health (good, neither good nor bad, bad), whether they worried about their life (yes/no), whether they suffered from insomnia, whether they took any psychoactive medication and if so whether the doses had been altered recently, and whether besides CR, they were undergoing any other psychological therapy.
All measures were taken at baseline and after 4 weeks of CR. The outcome assessment (both before and after the intervention) was performed by a masked psychologist.
Intervention
Cardiac rehabilitation
The standard treatment included cardiological training, which occurred three times per week, lasting 1.5 hours per session, with a 15-minute break. The intensity of training and the scale of training burdens were individually prescribed. Based on an exertion test, a heart rate reserve was calculated, which is the maximum exertion of heart rate, minus resting heart rate. The exercised heart rate is the resting heart rate plus 40–85 percent of the reserve. All exercises were supervised by medical personnel. A detailed description of the CR has been included in Supplementary Appendix SA1.
As a part of standard CR, the control group received Schultz’ Autogenic Training (SAT). 17 SAT is a relaxation method in which the patient, lying or sitting in a comfortable position with eyes closed, is listening to suggestions delivered by a therapist. Following the therapist's instructions, the patient is trying to breathe slowly and gradually relax the individual parts of his or her body. SAT was played from a CD by a psychologist.
VR therapeutic support
As a VR source, the VRTierOne® device produced by Stolgraf, without® was used. The hardware consisted of VR HTC VIVE goggles and two controllers (manipulators), all plugged into a personal computer. 21 Thanks to a head-mounted display and total immersion, VR therapy provides an intense visual, auditory, and kinesthetic stimulation. In the Virtual Therapeutic Garden, there is a rich set of symbols and metaphors based on the Ericksonian psychotherapy approach. 22 The most important is the Garden of Revival, which symbolizes the patient's health. The metaphor of the garden, weakened and gray at the beginning, but becoming more and more colorful and lively with every session, symbolizes the process of regaining energy and vigor (Supplementary Figs. S1–S4). There were eight sessions of VR therapy, each 20 minutes long. The therapy was conducted twice a week for 4 weeks. The patients participating in VR sessions did not take part in SAT. VR therapy was administered by a physical therapist. A detailed description of the therapy and screen captures (pictures) has been included in Supplementary Appendix SA1.
Statistical analyses
The data were analyzed in Statistica 12 (StatSoft). Descriptive statistics were presented with means and standard deviation percentages. Data normality was analyzed using the Shapiro–Wilk test. Differences between variables were evaluated before and after the intervention, and were calculated using paired sample t-tests. The between-group differences in categorical data were compared using chi-square tests, and continuous variables with independent t-tests. A significance level of α < 0.05 was established.
Results
In total, 34 participants were included in the study. Two of them could not complete the intervention because of vision problems (Fig. 1). Baseline characteristics were similar between groups (Table 1). The average age was 68.9 years, with a mean body mass index of 27.8. All participants had CAD, with 62.5 percent postendarterectomy and 37.5 percent post-MI. A total of 75.0 percent of participants examined at baseline expressed fear about their lives, 59.3 percent evaluated their health as “bad,” 72 percent suffered from insomnia, and 62.5 percent had used calming psychoactive drugs before starting their CR. In the course of the research, medicine doses were unchanged nor was any new kind of treatment initiated.
In analyzing the results of primary outcome measures, we found a statistically significant decrease in the general HADS data in the intervention group of 19.2 percent (mean 19.46 pretreatment vs. 15.73 post-treatment, p = 0.003). The results obtained in HADS subscales were also significantly reduced: HADS-A by 16.0 percent (10.47 vs. 8.80, p = 0.01) and HADS-D by 23.0 percent (9.00 vs. 6.93, p = 0.003). In contrast, in the control group, HADS-D increased significantly by 4.1 percent (10.06 vs. 10.47, p = 0.03), and the general HADS results, together with HADS-A, were not significantly changed (Table 2).
Virtual Reality Therapy Effects, Mean (Standard Deviation)
CI: confidence interval; HADS, Hospital Anxiety and Depression Scale; PSQ, Perception of Stress Questionnaire.
With reference to data from the secondary outcome measures, we found a statistically significant decrease in general PSQ results of 12.8 percent (64.73 vs. 56.47, p = 0.03). Analysis of the PSQ constituents revealed that emotional tension was reduced by 19.0 percent (25.93 vs. 21.00, p = 0.0001), and intrapsychic stress by 12.5 percent (21.80 vs. 19.07, p = 0.03). There were no statistically significant changes in the PSQ in the control group (Table 2).
Discussion
Timely identification of patients who are depressed or anxious could help improve cardiac treatment outcomes. Similarly, knowing a patient is depressed should alert the cardiologist that more effort may be needed to help the patient to maximize the benefits of treatment. 23 The question therefore arises concerning the type of additional treatments that should be implemented to improve the mental state of CAD patients. To date, only one RCT focusing on CAD patients found that treating depression by pharmacotherapy improved event-free survival, 24 but all the major trials have found that patients whose depression improved had longer event-free survival than those who continued to report significant depression symptoms. 25
In the large Cochrane review summary, the authors stated that psychological treatments had important health benefits for CAD patients, reducing the rate of cardiac mortality and alleviating the psychological symptoms of depression, anxiety, and stress, however, future trials testing the efficacy of specific psychological techniques were essential. 26 Modern technologies can provide high-quality therapeutic programs for patients. The recent literature has shown that VR therapy could be a very effective treatment for mental anxiety and depression problems. 12 Although no VR-related studies in this review have referred to the mental state of patients with heart disease, there are some reports describing VR-augmented cardiopulmonary rehabilitation and “exergames” for CAD patients. 27 In the summary of a literature review published in 2018 on this topic, the authors stated that virtual CR was shown to improve the physical conditions of cardiac patients more effectively than conventional CR and that augmented VR rehabilitation was a promising candidate for next-generation CR, with good compliance. 28
Our research project bridged studies evaluating VR for mental problems and VR-enhanced CR. We believe that depression and anxiety in CAD patients are so important that we should develop specific VR therapy, which would support a patient's psychological state. The therapeutic method used here is the first to implement Ericksonian psychotherapy into the virtual environment. However, other psychosocial interventions that improve mental health, for example, cognitive behavioral therapy or relaxation techniques, have also been successfully applied in studies using the VR environment. 12 Our study demonstrated a statistically significant decrease in depression symptoms, as well as stress and anxiety levels after VR therapy. Similar data were published in 2014 assessing the effectiveness of a VR-based stress management program in people with mood disorders. 29 VR relaxation had significantly lowered subject stress (p < 0.001), depression (p < 0.001), anxiety (p < 0.001), and increased skin temperature (p < 0.001), but there were no patients aged older than 60 in the studied group, and therefore, our results are a relevant addendum to current knowledge. 29
Important observations can be found in the article published in 2019, due to the same method of assessing mental state (HADS). 30 Navarro-Haro et al. found that in patients with generalized anxiety disorders, mindfulness-based virtual interventions were as effective as standard mindfulness procedures, but VR was a good tool to increase treatment adherence and motivation. In their study, the average HADS-A scores decreased by almost three points in the VR group, from 13.0 (SD 4.1) to 10.2 (SD 4.72). 30 In our study, the difference was almost two points, from 10.5 (SD 2.5) to 8.8 (SD 3.1) (p = 0.01). With regard to HADS-D data, Navarro-Haro et al. reported a reduction of about two points in depressive symptoms, from 8.6 (SD 3.8) to 6.5 (SD 3.9). 30 This reduction was similar to our data, where we observed a decrease in depressive symptoms from 9.0 (SD 2.4) to 6.9 (SD 3.1) (p = 0.003). However, it is worth noting that the average age of physically healthy patients in Navarro-Haro et al. was 44.3 (SD 10.2), whereas in our study, the average age of our seriously ill patients was 68.9 (SD 6.3). Therefore, our results serve as an important addendum to the current knowledge.
The analysis of the results obtained in the control group calls for a separate consideration. It was found that in the group receiving standard CR, the patients' mental health did not improve despite CR and regular SAT sessions. Similar outcomes were observed by Szczepańska et al., published in 2012. 10 It seems that SAT no longer serves its purpose. The most important studies on that technique date back to the 1960s.31–34 Its efficacy in heart diseases was demonstrated in the 1970s,35–37 and it was implemented into standard CR in the 1990s. The last decade has seen such an acceleration of the pace of life and the amount of stimuli that are constantly affecting us (as, for instance, a mobile phone) that we have lost the natural ability to enter into a state of psychophysical relaxation, which restores our mind and body. This may prove even more difficult for cardiac patients with severe anxiety and depression symptoms. The possibility of total immersion in an appropriately prepared VR environment seems beneficial, as it helps to grab the patient's attention, stop the torrent of thoughts, and allow him or her to receive the therapeutic content.
Our study has limitations. First, due to the innovative nature of the research, the study group was small. Second, the PSQ was used as a secondary outcome measure and despite its high repeatability and validity, it is not widely used in scientific research. According to Birckhead et al.'s (2019) recommendation for Methodology of Virtual Reality Clinical Trials in Health Care, future studies should focus on VR3 phase (RCTs). 16 Thus, it is recommended that this study be repeated with a larger group of cardiac patients, using a wider range of diagnostic tools, including more objective ways of measuring stress levels (e.g., cortisol levels) and exercise tests, before and after intervention.
Conclusions
VR therapy significantly reduced the severity of depressive symptoms, anxiety, and stress levels in CAD patients undergoing outpatient CR. Immersive VR therapy effectively supports the CR of individuals with anxiety depressive symptoms. Cardiac patients gain benefits from total immersion in a Virtual Therapeutic Garden.
Footnotes
Acknowledgment
The authors would like to thank Krzysztof Klajs, the Director of Polish Milton H. Erickson Institute, for his support throughout the study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.