
Abstract
Abstract
In the last decade, several programs for the treatment of cannabis-related disorders were developed. Until now, no information is available on the efficacy of Internet-based counseling approaches for this target group. This article describes the evaluation of “quit the shit,” a web-based intervention developed to help young people to quit or reduce their cannabis use significantly. Cannabis users seeking web-based treatment were included in a two-arm controlled trial conducted on a website for drug-related information and prevention. After the baseline assessment, members of the treatment condition were randomized to a 50-day intervention program. Other trial participants were put on a waiting list. A post-test was conducted 3 months after randomization. Of all 1,292 subjects included in the trial, a total of 206 participants took part at the post-test. Per-protocol- and intention-to-treat analyses were conducted. Members of the treatment condition showed a significantly stronger reduction in cannabis use (primary outcome) than the control group. In the per-protocol analyses, moderate-to-strong effects were found for the reduction of the frequency and the reduction of the quantity of consumed cannabis. Small-to-moderate effects were observed on the secondary outcomes (use-related self-efficacy, anxiety, depression, and life satisfaction). Despite limitations concerning the interpretation of the results, the intervention seems to offer an effective treatment option for persons with cannabis-related problems.
Introduction
Although cannabis use has been comparatively prevalent in Western European and North American countries for more than 40 years, only during the last 10 years have intervention programs for cannabis addicts been empirically evaluated. By now, several randomized controlled trials (RCT) examined the effects of motivational enhancement therapy (MET), cognitive-behavioral therapy, and the combination of these two approaches on patients with cannabis addiction.4–9 The Cochrane Collaboration 10 summarizes the results of these works as follows: “(…) all psychotherapies tested (cognitive-behavioral, motivational enhancement) have been demonstrated to be effective to reduce cannabis use delivered both in individual or group sessions.”(p9)
Due to the high number of Internet users in developed countries, and due to their considerable interest in health-related topics, 11 the World Wide Web offers new promising ways of addressing individuals affected by addiction-related problems. Content can be accessed anytime and thanks to mobile devices from almost anywhere at a high-cost effectiveness. At present, several web-based interventions in the realm of anxiety disorders,12,13 burnout-related problems,14,15 overweight,16,17 and eating disorders 18 have been shown effective.
Regarding web-based interventions for addiction-related disorders, a varied picture can be drawn. Although several evaluated programs on smoking cessation and on the reduction of alcohol consumption are by now at hand, Internet-based interventions for drug addicts are still rather rare. 19 In the last 2 years, several overview works on the potential of web-based programs for smoking cessation were published.20–22 Out of 287 published scientific articles, Myung and colleagues 21 included an overall of 22 RCTs with a total number of nearly 30,000 participants into a meta-analysis that was used to evaluate the effects of computer- or web-based interventions on smoking cessation. The authors of that work draw the conclusion “that there is sufficient clinical evidence to support the use of web- and computer-based smoking cessation programs.”(p929)
The web-based programs for smokers are meant to support cessation, whereas alcohol-related interventions aim at a reduction of problematic alcohol use. In general, these are single-session interventions. They include a one-time personalized feedback on current alcohol consumption, generated by a database on grounds of the provided information by the user. The efficacy of web-based interventions to reduce alcohol consumption was also dealt with in a meta-analysis, which included 14 randomized controlled trials. 23 According to its results, single-session interventions delivered via the Internet are well suited to reduce alcohol consumption at least in the short term.
According to a systematic research by the EMCDDA,
19
an empirical evaluation of Internet-based intervention programs in the field of illegal drugs is still pending. In the summer of 2004, the German Federal Centre for Health Education (BZgA) developed a web-based counseling program for cannabis users called “quit the shit” (QTS) and integrated it into the drug prevention website
The present trial aims at assessing the effectiveness of QTS, with the use frequency and quantity being primary outcomes. An increase of use-related self-efficacy, a secondary outcome, is also expected. Cannabis use and abuse have repeatedly been related to an impaired psychological well-being.24–26 Moreover, there is evidence that intervention programs targeting cannabis abuse also have an effect on related measures. 8 Therefore, we expected a positive impact on psychological well-being and included trait-anxiety, depression, and life satisfaction as secondary outcomes.
Methods
The structured counseling program QTS
The 50-day counseling program QTS comprises four consecutive phases: (1) The registration procedure mainly consists of an online questionnaire that is used to collect data relevant both for counseling and for program evaluation. (2) Admission takes place in the one-to-one chat of the program and is carried out by one of four qualified psychotherapists working for QTS. Usually, each user stays with the same counselor throughout the whole program. The admission chat takes ∼50 minutes, aims at clarifying the individual situation of the counseled person, and helps determine individual consumption goals and coping strategies. (3) After the admission chat, the online diary of QTS is activated. In this personal, password-protected area of the counseling program participants are required to write down all relevant aspects of their cannabis use over a period of 50 days. Once a week, all participants get detailed feedback on their entries by their counselor. The feedback relates to the consumption (current, in the course of the program), to the psychosocial situation of the participant, and to the counseling process as such. (4) The aims of the concluding chat are to reconsider to what extent the individual consumption goals were achieved, which strategies were suited to control cannabis consumption, and to determine whether further professional help is required. The program structure and counseling are based on the principles of self-regulation and self-control. 27 In the intervention, a solution-focused approach 28 is applied. So, all endeavors in the process of counseling focus on the aim to cease or reduce cannabis consumption. The program is free of charge. A secure connection to the program server via https-protocol is provided. The only personal data required for participation is the e-mail-address. Therefore, if an incognito e-mail-address is used, it is possible to utilize the program anonymously.
Study design
The study was conducted on the website of QTS (
To generalize the study results on the regular users of QTS, there were no predefined exclusion criteria. Everybody who expressed the wish to reduce or to cease cannabis use and wanted to take part in the study was included. To keep the threshold for a participation low and, thus, avoiding selection effects, personal data such as name, address, or phone number were not required, just like in everyday business of QTS.
Trial participants were recruited directly from the website of
After registering with the trial and filling out the baseline questionnaires (i.e., by entering the online-schedule for the admission chat), the participants were randomly allocated to the conditions by a software algorithm independent of the investigators and counselors. The follow-up survey was carried out 3 months after registration in an online-questionnaire. Recruitment was done by e-mail; thus, all QTS participants (regardless of the duration of the program usage) and all waiting list members were invited 3 months after trial registration. If participants did not react within 5 days, they were sent another invitation. This time, they were offered remuneration for their effort (shopping voucher worth 30 Euro).
Measures and instruments
At baseline, sociodemographic data, information on cannabis use, on use-related self-efficacy, and on psychological well-being was collected. Information on the frequency (days of consumption) and the quantity (in grams) of cannabis use during the last 30 days was gathered. The use-related self-efficacy was measured using a German adaptation of the Drug-Taking Confidence Questionnaire-8. 29 Cannabis addiction was determined in line with DSM-IV criteria published by the American Psychiatric Association. 3 The Trait Scale of the State-Trait Anxiety Inventory 30 with a total of 20 items was used to measure the level of anxiety. Depressive symptoms was measured using the short version of the General Depression Scale (Allgemeine Depressions-Skala, ADS) 31 consisting of 15 items. In addition, general life satisfaction was measured with the German adaptation of the Satisfaction with Life Scale (SWLS, 5 Items). 32
Statistical analysis
To examine the efficacy of the program, analyses of covariance were conducted. In each analysis, the baseline score of the corresponding outcome measure was included as covariate. In case of statistical significance, we calculated baseline-corrected Cohen's d as effect size. 33 An alpha level of 0.05 (two-tailed) was chosen. Per-Protocol- (PP) and intention-to-treat-analyses (ITT) were conducted. To deal with missing follow-up information, data of all randomized participants who did not complete the follow-up were imputed by Multiple Imputations (MI) and Last-Observation-Carried-Forward (LOCF) method. However, since MI usually provides more accurate parameter estimates of missing data than LOCF,34,35 our ITT analyses concentrated on MI. To account for the sizeable drop-out rates, 100 imputations were conducted with Stata's “MI” command using the predictive mean matching method.
To determine differential loss to follow-up and to compare both study groups at baseline, logistic regressions were conducted (two-tailed α=0.05). All analyses were performed with Stata 11. After conducting a power analysis, a total sample size of n=200 was aimed for. We yielded to detect small to medium between group effects (d=0.35) with 80 percent power at an alpha-level of 5 percent. 33
Participants
1,292 persons declared that they were motivated to quit or at least significantly reduce cannabis use within the next weeks and, thus, registered with the study (Fig. 1). Of these, 429 persons were allocated to the waiting list and 863 to the treatment. To have comparable group sizes for the follow-up survey, two of three persons were allocated to the treatment condition. This unequal distribution was necessary to make up for the losses arising through persons who had been allocated to the treatment condition but who, in fact, did not take part in QTS (n=503). They had made use of the scheduler but then did not keep their appointment. Eventually, 360 persons participated in QTS. One hundred eighty-three of the QTS participants discontinued the intervention, that is, they quit the program before its duration of 50 days was reached. All 360 participants of QTS were invited for the follow-up.
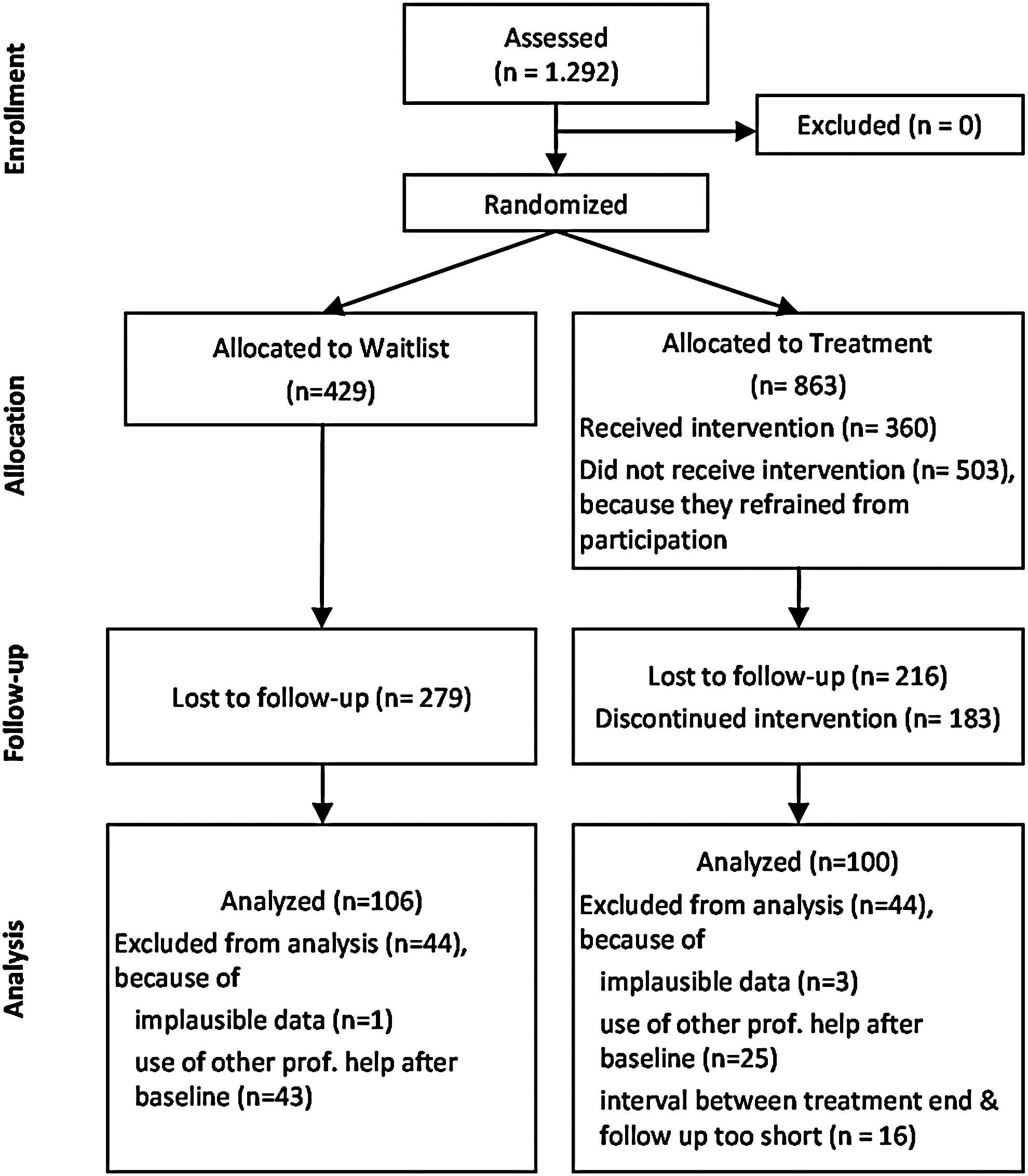
Flowchart of participants.
Of the 429 persons allocated to the waiting list, 150 persons took part in the follow-up survey in due time, that is, within 15 days after receipt of the first invitation e-mail. In the treatment condition, 144 persons answered the questionnaire in the given period of time. 44 data records of the waiting list were excluded from analysis, as they either contained implausible information (n=1) or because the person completing the questionnaire claimed having made use of other professional help during the last 3 months (n=43), such as a drug advice center or a psychotherapist. Consequently, 106 cases were included in the analysis. In the treatment condition, 44 follow-up cases were excluded from the data analysis, mainly because they made use of additional professional help (n=25) or due to implausible information in the questionnaire (n=3). Further, 16 data records had to be rejected, because less than a minimum of 30 days had passed since the completion of QTS. This may happen if the registration and the admission chat are relatively far apart from each other due to time constraints. The analyzed sample in the treatment condition consists of 100 cases.
The mean age of the 206 follow-up participants (70.5 percent male) was 24.7 years (SD=6.8). On average, they consumed cannabis for 8.9 years (SD=6.2). The vast majority (92.0 percent) was cannabis dependent according to DSM-IV criteria. The educational level of the participants was relatively high, 36 with 58.7 percent attending grammar school (“Gymnasium”) or having reached A-Levels (“Abitur”). Participants of QTS used the intervention an average of 30.2 days (SD=19.8).
Results
Differential loss to follow-up
To detect differential loss to follow-up, bivariate logistic regressions were conducted with sociodemographic variables, cannabis use, and measures of psychological well-being as predictors and follow-up participation as outcome. Life satisfaction was the only significant predictor for follow-up participation (SWLS score: odds ratio: 1.02; 95 percent-confidence interval: 1.00–1.04; Wald Chi 2 (1)=4.07; p=0.044). Hence, participants with a higher score in the SWLS provided valid follow-up data slightly more often. Moreover, members of the treatment group who used QTS over the full 50 days were more likely to take part at follow-up than those who quit QTS prematurely (odds ratio: 3.80; 95 percent-confidence interval: 2.30–6.27; Wald Chi 2 (1)=27.06; p<0.001). The over-representation of those who completed the program as scheduled was balanced by applying a probability weight to the data during the following analyses. Since differential loss to follow-up had either been addressed by data weights or was just marginal, it was assumed that participants in the follow-up trial adequately represent all study participants.
Pretreatment differences
No between-group differences in pretreatment scores were detected in any of the study measures.
Evaluation results
In the PP analysis, which only included the data of those who left valid follow-up data, the analyses of covariances yielded significant effects in every outcome variable (Table 1). Users of QTS show a significantly stronger reduction in both consumption measures than members of the waiting list. The between-group effect sizes in use frequency and quantity can be considered as moderate to large. There are moderate effects on use-related self-efficacy. Further, QTS participants show a significantly stronger improvement of psychological well-being (Table 1). Thus, a lower level of anxiety and depression and a higher life satisfaction were observed in the treatment condition.
Group comparisons were conducted with univariate ANCOVAs adjusted for the baseline value of each measure.
SD, standard deviation; DTCQ, drug-taking confidence questionnaire; STAI-T, trait scale of the state-trait anxiety inventory; ADS, allgemeine depressions-skala; SWLS, satisfaction with life scale; ANCOVA, analyses of covariance.
The ITT-analysis, which utilized MI, reveals statistically significant group differences in the use-related measures (frequency, quantity, and self-efficacy) and the level of anxiety (Table 2). However, the only effect that can be regarded clinically relevant was found for use frequency. In the LOCF-analyses, significant group differences use can be shown for the use-related measures too (frequency, quantity, and self-efficacy; p≤0.017; not shown in Table).
Group comparisons were conducted with univariate ANCOVAs adjusted for the baseline value of each measure. The F-test of each comparison refers to the whole model including the covariate. The T-values refer to the group differences. Effect sizes are reported only in case of statistical significance.
Discussion
Depending on the method of analysis, fairly different results were found. First of all, the PP analysis indicates considerable treatment effects. Thus, according to follow-up data, users of QTS showed a noticeable stronger consumption reduction than nontreated individuals. Moreover, the clients' self-efficacy was enhanced remarkably. The scores in measures of psychological well-being improved as well. At completion of the program, QTS users stated a lower level of anxiety and depression, as well as a higher life satisfaction. No similar tendencies were observed among waiting list members who provided follow-up data. However, the results of the ITT analysis only partly reach statistical significance. According to this analysis, which included all participants, only the use frequency was substantially affected.
To interpret the data, the advantages and disadvantages of both methods of data analysis have to be reviewed at this point. Analyses according to the ITT principle can be regarded as the gold standard in efficacy studies, as they are assumed to provide a conservative estimation of the treatment outcome. However, in case of high attrition, the power of an ITT analysis to detect between-group differences diminishes considerably—a problem to be faced in numerous online trials. 37 Especially the high and differential dropouts in the treatment condition had a remarkable impact on the ITT effects. In detail, the 503 members of the treatment condition, who did not take part in the intervention but were still included in the ITT analysis, presumably lead to an underestimation of the treatment effects. In light of this situation, the small effects found within the ITT analysis are not surprising.
On the other hand, the PP analysis probably overstates the effect of the intervention, as the differential dropouts in the treatment condition supposedly lead to a varied motivational level in both study groups. That is, at least the willingness to make use of web-based aids such as QTS was presumably stronger in the treatment condition. However, it is unclear whether this also applies to the motivation to change one's own cannabis use. Individuals who finally opted against a program participation still might have seriously been working on reducing their cannabis use. Moreover, the differential loss to follow-up in the observed variables had either been addressed by data weighting or just was of small size.
So, how are the results of the trial to be interpreted in the light of these results? First of all, one has to point out that there are no controlled trials on web-based interventions for cannabis users currently at hand. However, in comparison with outpatient interventions, at least the results of the PP analysis suggest a satisfactory effectiveness of QTS. Thus, the effects on use frequency seem to be quite similar to the results found in the RCT performed by Stephens and colleagues, 5 who examined the performance of two different kinds of outpatient treatments for cannabis use. In the trial, the effects of the relapse prevention support groups on use frequency were strong (d=1.01) and for the alternative treatment (individualized assessment and advice), medium (d=0.85). The Marijuana Treatment Project, 8 which compared two brief interventions for cannabis-dependent adults in a multisite RCT, found medium-to-strong effects on cannabis use as well. Thus, the outcomes for a two-session MET amounted to d=0.59, and the effects for a nine-session multicomponent therapy (with MET, cognitive-behavioral therapy, and case management) added up to d=1.14. Comparing the level of depression, QTS presumably comes to better results. Thus, according to the results obtained by the Marijuana Treatment Project, the nine-session intervention had no impact 4 months after randomization (d=0.02) and weak effects on anxiety (d=0.20). Nevertheless, we again have to point out that there are considerable constraints to the comparability of the studies, mainly because of the different character of the interventions and due to the methodological issues which have been just mentioned.
To overcome the methodological constraints, future trials of QTS should improve the recruitment procedure. The goal should be to establish a more thorough commitment on behalf of the participants to stay within the trial, as a great amount of subjects obviously regarded their participation as nonbinding and dropped out. Therefore, we should optimize the recruitment for the follow-up survey (e.g., by additional telephone-calls). Especially selective drop-out from only one trial condition should be avoided in any case.
In spite of their many potential benefits, there are significant drawbacks to Internet-based interventions. First, anonymity cannot be guaranteed if program users register with a nonanonymous e-mail-address or an address that is published elsewhere in the World Wide Web and, thus, can be connected to this person. Moreover, confidentiality can be endangered if the computer used for program participation is also utilized by other persons. However, by using a new and incognito e-mail-address and the privacy-mode in the web browser, these risks to confidentiality can be minimized.
Conclusion
Despite these limitations, the results suggest that the web-based counseling program QTS provides an effective support for those who want to quit or significantly reduce their cannabis use. These effects are presumably not limited to cannabis use, but also become apparent in an enhanced well-being of the clients. Thus, web-based QTS offers a promising new method of treating cannabis users.
Footnotes
Authors' Contributions
HPT and MDT conceived of the study and participated in its design and coordination. BJ participated in the design, data collection, and statistical analysis. PL and ES participated in the co-ordination. All authors read and approved the final article.
Disclosure Statement
No competing financial interests exist.