
Abstract
Abstract
Background:
Anorectal abscesses are a common condition in surgical emergencies. Their presentation can be challenging in elderly patients with dementia who are incapable of describing symptoms and duration. Pelvic abscess or other complications should be suspected when general symptoms do not improve after drainage. In these cases exhaustive source control (including defunctioning colostomy in some cases) and targeted antibiotic therapy are the correct management.
Case Presentation:
A 76-year-old female with Alzheimer dementia (memory loss and verbal incapability), fecal incontinence, and who was dependent for all activities presented to the emergency department on several occasions with fever of unknown origin and abdominal pain. On this occasion after a thorough physical examination she was diagnosed with an ischiorectal abscess. It was treated with drainage, empirical antibiotic therapy, and pus was sent for culture. Despite this theoretically adequate management, the condition progressed to a pelvic abscess. Culture results informed of mixed flora including Clostridium sp., Escherichia coli, Enterococcus faecium, Enterococcus faecalis, and Bacteroides fragilis. The infection was controlled with a targeted antibiotic therapy and a colostomy as a defunctioning technique. The patient recovered completely and the colostomy was well accepted by her caregivers.
Conclusion
This case illustrates the importance of an adequate initial diagnosis and infection control because even conditions considered easy to manage can progress to a life-threatening infection. In aging populations diseases usually have atypical presentations and unspecific symptoms. This case also illustrates how important it is to monitor patients post-operatively, because despite a theoretically adequate management they can present negative outcomes.
Anorectal abscess is a common surgical condition, although its real incidence is unknown, because only patients with most symptomatic abscesses or needing drainage visit emergency departments. It is estimated that approximately 100,000 cases per year are diagnosed in the United States [1]. It is usually considered a condition of minor severity and one that is easy to resolve with surgical drainage. However, a small percentage of cases can present as a complicated pelvic sepsis or perineal gangrene and produce a critical infection with associated complications and high mortality [2]. This is especially true in elderly patients with comorbidities and insidious presentations that are not identified by caregivers until clinical signs of systemic infection are noted. In this case report we present an illustrative example of an anorectal abscess with an atypical presentation that developed infection and pelvic sepsis despite initial surgical drainage.
Case Presentation
A 76-year-old female presented to the emergency department with a medical history of hypothyroidism, idiopathic pulmonary fibrosis, and 16 years of severe Alzheimer dementia (with loss of memory and verbal abilities) and fecal incontinence; she was dependent for all activities. She lived with her husband, who was her main caregiver, and her daughters. She had presented to the emergency department several times in the last six months because of fever of unknown origin and apparent abdominal pain on examination; she was incapable of reporting any symptoms. On the present occasion she presented with a similar episode with high fever (temperature, 40°C) and apparent restlessness. She was evaluated by the medical team in the emergency department and no urinary or pulmonary pathology was identified. After 24 hours in emergency department the surgical team was consultated because of the persistence of symptoms. On examination she had abdominal pain that was difficult to evaluate because of her lack of communication. A thorough physical examination identified a tender anal lump and swelling was noted. The patient was stable but she presented leucocytosis (15,500×103/muL) and a high C-reactive protein (CRP) of 162 mg/L. To rule out any abdominal condition, she underwent a diagnostic computed tomography (CT) scan that identified a horseshoe ischiorectal abscess (Fig. 1A).
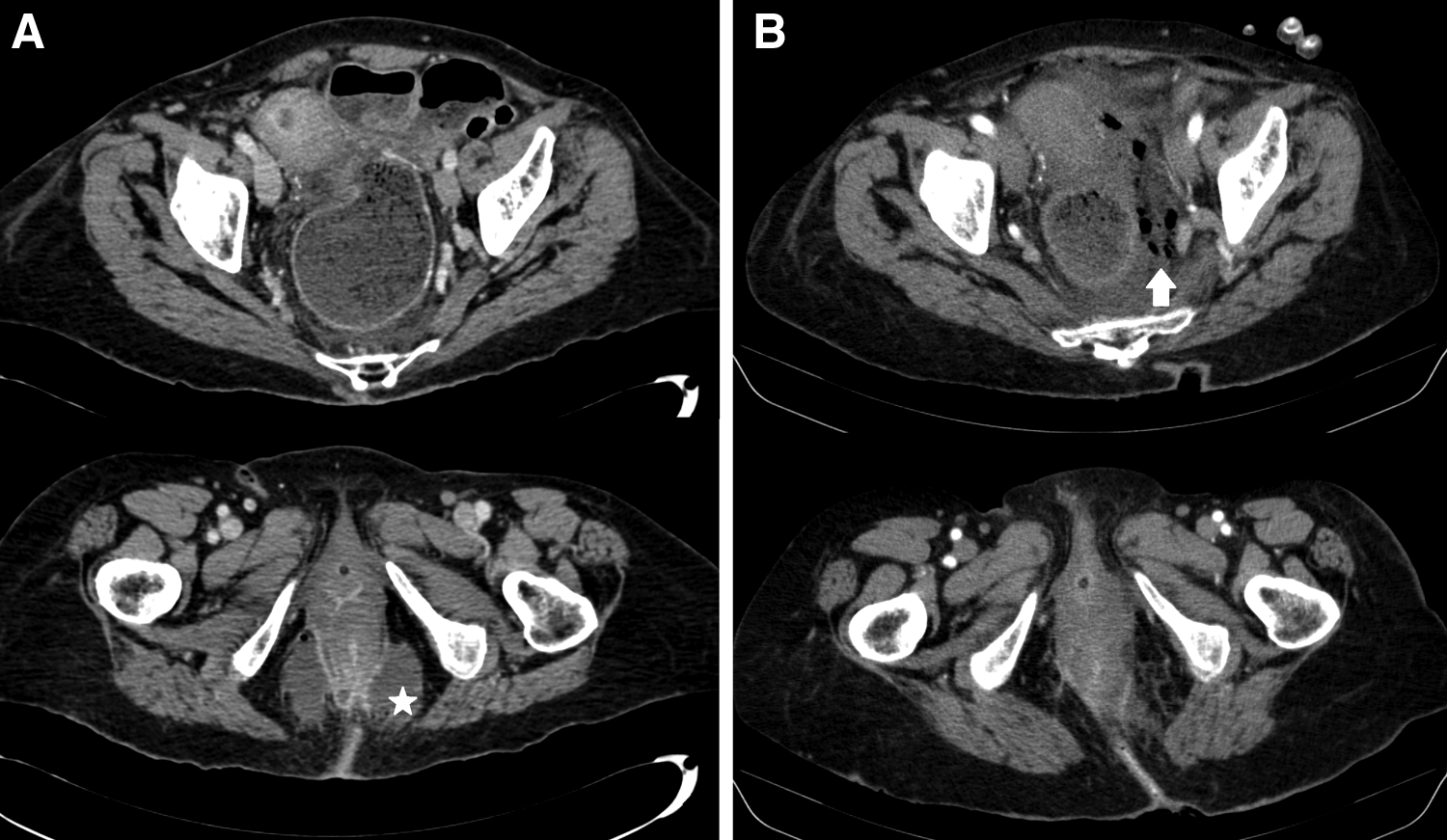
This image compares two abdominal computed tomography (CT) scans before (
An examination under anesthesia allowed perineal drainage of the abscess with two incisions (bilateral) to explore cavities and to break down loculations. Purulent discharge was sent for culture and empirical antibiotic therapy with piperacillin-tazobactam was prescribed. The surgical site was irrigated twice per day with saline until clear. Despite the theoretically adequate initial management, three days after the intervention the patient's general status was not improving as expected. Pain was uncontrolled with drugs, blood tests continued to be altered with persistent leucocytosis and high CRP, and she again presented fever. A second abdominal and pelvic CT scan was performed, showing a supraelevator progression of the infection with gas and fluid in the pelvis (Fig.1B). Culture results informed of Escherichia coli, Enterococcus faecium, Enterococcus faecalis, Bacteroides fragilis, and Clostridium sp (Table 1).
Culture Results and Antibiogram Showing the Identified Bacterial Species and their Resistance Patterns
Minimum inhibitory concentration (MIC) mcg/mL breakpoints according to EUCAST 2013.
The patient was taken back to the operating room where an abdominal approach was performed by an infra-umbilical laparotomy. The peritoneal reflection was opened and the pelvic abscess was drained with thorough lavage. A defunctioning terminal colostomy was created, excluding the affected area, after evacuation and lavage of the rectal stump. The perineum was also revised and debrided. In view of the initial cultures, targeted antibiotic therapy was initiated, adding linezolid and clindamycin to the initial piperacillin-tazobactam.
The patient recovered completely and was discharged after completing antibiotic therapy. The colostomy was well accepted by caregivers and would actually improve the patient's quality of life and perineal hygiene.
Discussion
With an increasing aging population worldwide, we can encounter in our daily practice many patients with dementia and neurologic disorders who may not be able to describe their symptoms or have atypical presentations of common conditions [3]. In these cases it is especially important to speak with the family or caregivers who know the patient and can detect changes in their basal status. As surgeons, we must have a high level of suspicion and perform a thorough physical examination of the patient to avoid missing important clinical signs and always include the perineal area. It is important to insist on this to trainees and residents. In the case presented, a more exhaustive initial examination, including a rectal examination, could have diagnosed the condition, saving time and improving clinical management.
Although sometimes altered due to age-related changes in physiology, clinical criteria such as systemic inflammatory response syndrome (SIRS), quick sequential organ failure assessment (qSOFA) score, or sequential organ failure assessment (SOFA) score can still be useful to help suspect infection and evaluate severity in the ED [4]. In our case, mental status could not be evaluated because of dementia, but other objective variables such as fever and leucocytosis were present. It is also important to consider that elderly patients with comorbidities and various medications may not present tachycardia or blood pressure alterations, so this can be misleading when calculating infection severity scores.
An adequate source control is essential, in this case the drainage of the abscess. However, it is also essential to continue evaluating the patient closely and to confirm that the clinical signs of infection improve because as in cases similar to ours, the infection may not be resolved completely or can recur. The message of this case for surgeons in training is to remember that surgery is not only what happens in the operating room, it is also all the process until the initial problem is completely resolved.
Empirical antibiotic therapy is also important in complicated infections but the only way to confirm spectrum or adapt it is by microbiologic confirmation. It is essential to obtain cultures, which can sometimes be surprising as in our case where multiple bacteria were found, including the gas-producing Clostridium, that could therefore be targeted. If the cultures had not been obtained in the first intervention, the delay in adequate antibiotic therapy could have resulted in a poor outcome.
There is some debate about the best approach for a pelvic abscess complicating an anorectal condition, and it is common to use only a perineal approach to drain it [5]. However in some cases with a complicated infection that is not being controlled or intra-abdominal collections, an abdominal approach must be performed. Defunctioning colostomies were widely used in the past to control fecal contamination of any perineal wound [6]. Presently, the decision for a colostomy must be targeted in each case, considering the background of the patient, the clinical condition, and the severity of the infection. In our case, the colostomy was a surprisingly positive outcome for the patient, because it improved her personal well-being and hygiene and facilitated care due to the previous fecal incontinence.
Finally, considering educational aspects of the case, when facing any infection younger residents must be mentored and trained to detect the clinical signs of an optimal or poor response. Anorectal pathology is usually drained and followed by younger trainees, as it is considered simple and easy to treat, but we must remember any infection is potentially severe and can result in a poor outcome if not managed correctly.
Conclusion
This case illustrates the importance of an adequate initial diagnosis and infection control, as even conditions considered easy to manage can progress to a life-threatening infection. In an aging population diseases usually have atypical presentations and unspecific symptoms. This case also illustrates how important it is to monitor patients post-operatively, because despite a theoretically adequate management they can present negative outcomes.
Footnotes
Acknowledgments
The authors would like to thank the Surgical Infection Society Europe for the opportunity of participating in the educational SIS-E Olympics in Hamburg (June 2017).
Author Disclosure Statement
No competing financial interests exist