
Abstract
Abstract
Background:
Surgical site infections (SSIs) after ventral hernia repair typically occur after discharge from the hospital, making timely diagnosis difficult. Successful treatment of SSIs may require re-admission and weeks to months of care and follow-up visits, which is potentially costly and burdensome to patients. To address these challenges, we have developed the Mobile Post-Operative Wound Evaluator (mPOWEr), a mobile health application that allows patients to record and transmit SSI symptom data and photographs to clinicians.
Case Presentation:
A 45-year-old female underwent open repair of a large recurrent ventral hernia with component separation and synthetic mesh sub-lay. After noting a change in the character of her drain output and transmitting the information via mPOWEr, she was diagnosed with a deep SSI requiring re-admission, operative washout, and negative pressure therapy. This management resulted in mesh salvage and healing without hernia recurrence, documented serially using mPOWEr.
Conclusions:
Diagnosis and treatment of SSIs after ventral hernia repair is challenging for physicians and patients alike. Mesh salvage is feasible in deep SSIs involving lightweight macroporous polypropylene mesh, but may require protracted care. Mobile health solutions that allow transmission of patient-generated health data can facilitate early diagnosis of SSI and long-term monitoring of outpatient treatment.
With modern advances in hernia surgery including component-separation techniques, surgeons are able to repair increasingly large and complex ventral hernias with low recurrence rates [1]. However, post-operative surgical site infections (SSIs) remain common, affecting more than 20% of open ventral hernia repairs [2]. Treatment of these infections typically requires a combination of antibiotic therapy, wound care, percutaneous drain placement, or re-operation, in some cases with mesh explantation. Thus, it is perhaps not surprising that SSIs have been shown to be the overall costliest healthcare-associated infection [3].
In addition to being costly, SSIs can pose diagnostic challenges, because 60% of SSIs occur after hospital discharge [4], placing patients at risk for delayed diagnosis and attendant septic complications. Moreover, given that more than half of patients who develop an SSI after discharge are re-admitted to the hospital and many require ongoing SSI care with close incision monitoring, even non-operatively treated SSIs can be burdensome to patients, in particular those who live far from their surgical care environment or have limited mobility or transportation means. In an effort to aid in early diagnosis and treatment of SSIs, we have developed the Mobile Post-Operative Wound Evaluator (mPOWEr), a patient-centered mobile health (mHealth) application accessible via smartphone, tablet, or computer that combines a validated post-discharge SSI surveillance questionnaire with patient-generated incision photographs [5]. In this report, we describe a case of deep SSI after abdominal wall reconstruction that was treated successfully with salvage of the involved synthetic mesh, highlighting the utility of mHealth-transmitted patient-generated health data in SSI management.
Case Presentation
A 45-year-old female presented to our clinic with an 8-year history of progressive abdominal bulge associated with debilitating pain. She had undergone a mesh repair of a primary umbilical hernia 13 years prior. On physical examination, she had a large irreducible ventral hernia (Fig. 1A). Computed tomography (CT) corroborated the physical examination findings, demonstrating an 11 cm (craniocaudad) by 8 cm (transverse) fascial defect with loss of abdominal domain (Fig. 1B–1C); an associated large hernia sac contained most of the small and large bowel, including an inflamed-appearing loop of ileum suspicious for entero-enteric fistula (Fig. 1B). Additional medical history included morbid obesity (weight, 135 kg; body mass index [BMI] 51 at her initial clinic visit), type 2 diabetes mellitus, and active smoking. Over the ensuing 15 months, she lost 36 kg in a medically supervised weight-loss program (reducing her BMI to 37), improved her blood glucose control, and achieved complete smoking cessation. Having optimized her pre-operative risk factors, we planned a retro-rectus mesh repair with an option to perform bilateral transversus abdominus release to restore abdominal domain and recreate the mid-line with wide mesh reinforcement.

Pre-operative hernia assessment. (
We began her operation with a mid-line laparotomy and extensive lysis of adhesions. Approximately 50 cm of hardened, abnormal ileum was densely adherent to the abdominal wall, consistent with a contained perforation and chronic entero-enteric fistula. We dissected this segment free, resected it, and performed a stapled anastomosis. There was no gross spillage of enteric contents. Pathologic review of this specimen revealed mesh from the patient's prior umbilical hernia repair within the small bowel lumen. After completing adhesiolysis, we noted that the fascial edges were more than 10 cm apart under great tension (Fig. 2A). This necessitated creation of bilateral myofascial advancement flaps, extending our dissection into the retro-rectus space to accommodate a bilateral transversus abdominus release [1]. We closed the posterior rectus sheath (Fig. 2B), placed a 60×60 cm macroporous polypropylene mesh sub-lay in the retro-rectus plane (Fig. 2C), and then closed the anterior rectus sheath. We placed closed-suction drains in both the retro-rectus and subcutaneous spaces and closed the subcutaneous tissue in layers after excising the hernia sac and 300 cm2 of ischemic skin, long attenuated by the hernia contents (Fig. 2D). Operative time (incision to closure) was 9 hours and 25 minutes.

Intra-operative photographs. (
The patient's initial post-operative course was unremarkable, and she was discharged from the hospital on the third post-operative day with drains in place. On post-operative day 6, the patient noted a change in character of the fluid in her subcutaneous drain from light and clear to dark, cloudy, and malodorous, as she documented in mPOWEr's “Drain Tracking” feature. As a result, she was seen in clinic the following day and given a prescription for antibiotic agents given the purulent appearance of her drain output (Fig. 3A). Whereas she initially was clinically well, she subsequently began reporting chills and malaise and thus was re-admitted on post-operative day 12 and started on intravenous antibiotic agents. Computed tomography demonstrated a subcutaneous fluid collection consistent with deep SSI. We returned to the operating room for incision and drainage, evacuating approximately 100 mL of frank purulence and debriding an area of non-viable anterior rectus sheath, leaving a 15 cm length of intact exposed mesh (Fig. 3B). We initiated negative-pressure wound therapy with instillation of dilute Dakin solution until the first dressing change at 48 hours; by the second vac change on post-operative day 16, there was robust granulation tissue and no evidence of ongoing infection (Fig. 3C). The operative cultures grew multi-drug–resistant
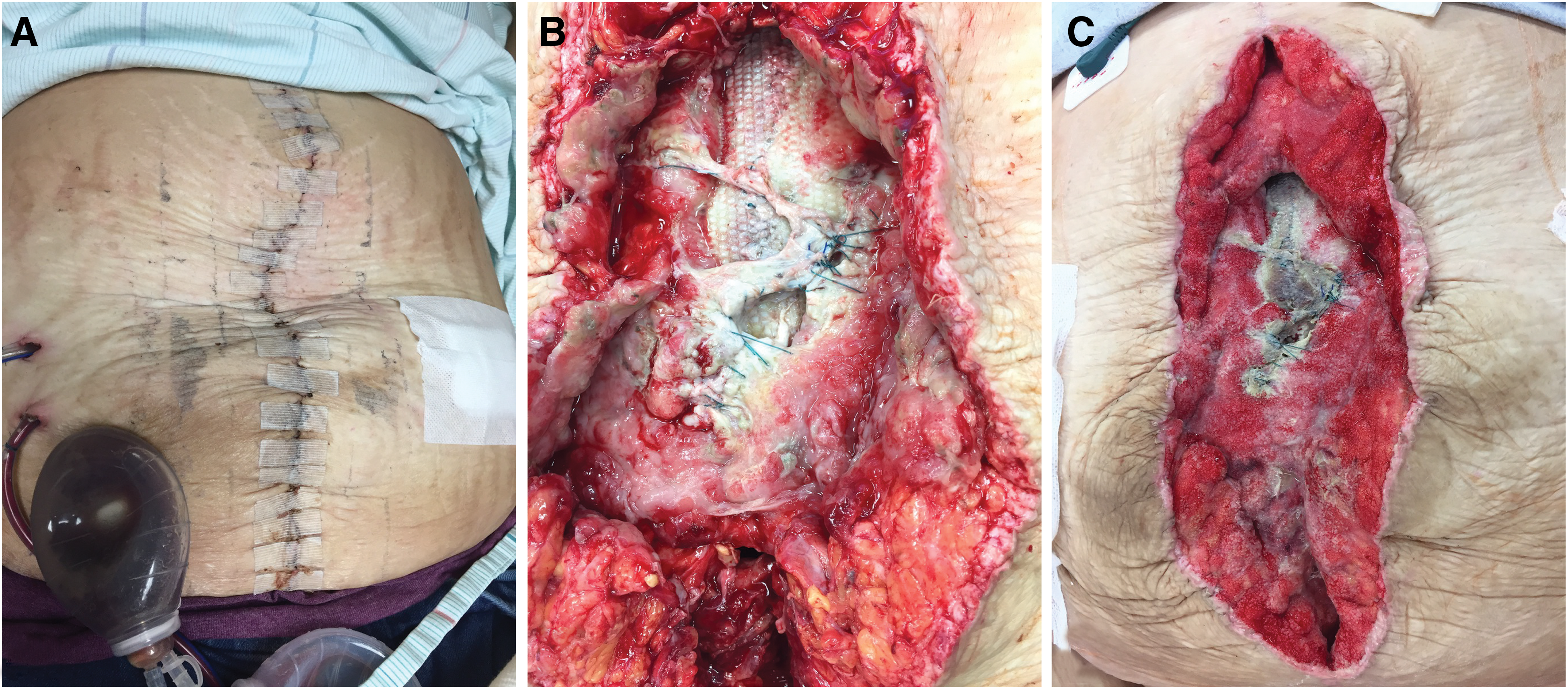
Early post-operative photographs. (
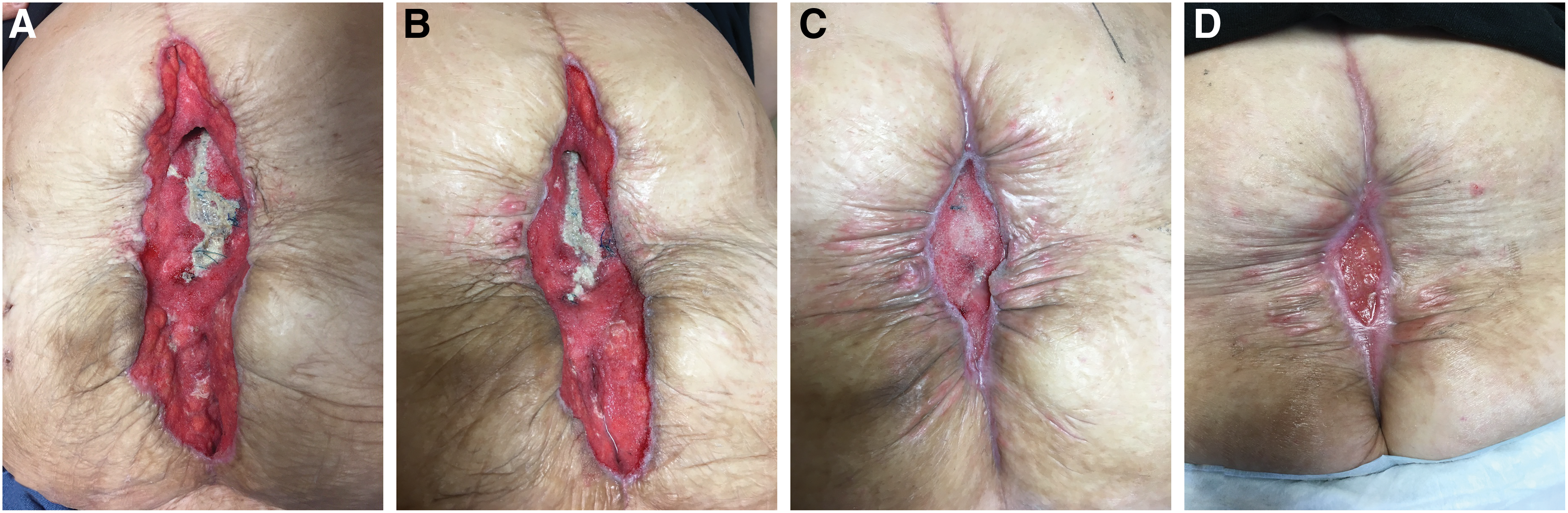
Late post-operative photographs. Progression of healing incision with negative pressure therapy at post-operative day 26 (
Discussion
Mesh infection after ventral hernia repair can be a devastating complication, because historically it has typically required re-operation for mesh removal, leading to hernia recurrence and the need for additional operations. Accordingly, careful pre-operative assessment and optimization of SSI risk factors is of paramount importance in minimizing occurrence of mesh infection. At her initial presentation, our patient had three modifiable risk factors for SSI: morbid obesity, diabetes mellitus, and smoking [6]. Pre-operatively, she was able to achieve considerable weight loss, excellent blood glucose control, and complete smoking cessation, favorably altering her SSI risk profile. However, she had several other SSI risk factors that were not modifiable: American Society of Anesthesiologists (ASA) score of 3, concomitant bowel resection, and relatively long operative time [6,7] because of the complexity of her case. These factors may have contributed to her development of a deep-space (i.e., mesh) infection.
Given the presence of these non-modifiable risk factors for SSI, in particular the unavoidable contamination introduced by the small bowel resection for her chronic entero-enteric fistula related to prior hernia mesh, our decision to use permanent, synthetic mesh in our repair warrants comment. Until recently, standard practice in the United States has been to avoid synthetic mesh in contaminated fields, instead favoring biologic mesh. The rationale for this practice had been fear of mesh infection requiring mesh explanation. However, there are no high-quality data to support this practice, and with the advent of modern lightweight macroporous monofilament polypropylene mesh—shown to be much more resistant to infection, likely because of decreased surface area for bacterial adherance—there has been increased enthusiasm for using synthetic mesh in contaminated fields [8]. Multiple recent reports confirm that although ventral hernia repair in clean-contaminated and contaminated fields are unsurprisingly associated with high incidence of SSIs, the vast majority of these infections can be treated successfully with negative pressure therapy, avoiding the need for mesh explanation often required in the prior era of dense, microporous, multifilament mesh [9,10]. Our case report adds to this growing literature supporting the practice of using synthetic mesh in contaminated hernia repair, because despite the occurrence of a deep SSI, our patient has made a full recovery with mesh salvage and has no sign of hernia recurrence at nine months post-operative.
This case also illustrates the utility of mHealth-transmitted patient-generated health data in diagnosing and treating SSI. Our patient documented and communicated the change in the character of her drain output via the mPOWEr application, ultimately leading to timely re-admission and initiation of treatment and therefore potentially helping to avoid sepsis or other serious sequelae. In addition, we and the patient used mPOWEr to document serially the progress of her wound, both while she was an inpatient and then during months of outpatient incision care. The patient and providers believe that patient-generated incision photographs enhanced communication and engendered confidence in the care delivered. This was especially important because the patient lived more than an hour from the hospital. The secure transmission and storage of incision photographs allowed providers to track the progress of the incision accurately over time with fewer clinic visits, mitigating some of the burden associated with SSI. Until recently, the use of mPOWEr has been limited to the University of Washington, but we are currently in the process of expanding its availability and studying its clinical efficacy in hopes it may ultimately be used widely to improve outcomes related to SSIs.
Conclusions
Diagnosis and treatment of SSIs after ventral hernia repair can be challenging for physicians and patients alike. Mesh salvage is feasible in deep SSIs involving lightweight macroporous monofilament polypropylene mesh, supporting the use of synthetic mesh in contaminated hernia repairs. Mobile health solutions such as mPOWEr may facilitate early diagnosis and long-term management of SSIs.
Footnotes
Author Disclosure Statement
The authors have no competing financial interests.