
Abstract
Abstract
Background:
Primary peritoneal carcinoma (PPC) is a rare malignancy, which is closely related to ovarian cancer. Surgical debulking and chemotherapy are the hallmarks of therapy; the malignancy has an acceptable prognosis.
Case Presentation:
A 70-year-old female with known metastatic PPC presented to the emergency department with acute abdomen six days after chemotherapy. Computed tomography (CT) revealed substantial amounts of free air. During emergency exploratory laparotomy, peritoneal carcinomatosis was found and the source of the peritonitis was identified as a leak in the small bowel at an area of tumor necrosis. The ulcerated perforated area was excised and primarily closed in two layers; mobilization of the small bowel for an anastomosis was not possible technically because of the mesenteric tumor infiltration. The patient was discharged after 10 d and chemotherapy was re-started. She died five months later from tumor progression.
Discussion:
Surgeons may become involved in managing patients with PPC if complications such as bowel obstruction or perforation develop. Bowel perforation caused by tumor lysis of intra-mural metastases has been described for several types of cancer, however, to the best of our knowledge, this is the first such case reported for metastatic PPC.
Primary peritoneal carcinoma (PPC) is a rare malignancy, most closely related to ovarian cancer, with the principal difference being a decreased prevalence for involvement of the ovaries and spread along the fallopian tubes [1–4]. Grading, staging, and therapy of this rare tumor are identical to that of ovarian cancer, namely primary debulking followed by chemotherapy, with Cisplatin being the agents of choice [5–9]. The prognosis of PPC is acceptable with up to 50% of patients surviving five years. Patients may require multiple courses of chemotherapy, however, this appears to be associated with an improvement in overall survival. Primary cancers and metastases of various malignancies may infiltrate the wall of intra-abdominal organs. During chemotherapy this can lead to perforation of the affected viscus because of tumor lysis and subsequent development of intra-abdominal abscess or peritonitis. This has been described for multiple types of cancer, such as lymphoma, lung, ovarian, and breast cancer among others but none to date in the setting of PPC [10–15]. The course of such patients may be prolonged as a result of the intra-abdominal infection occurring during profound immunosuppression associated with recent chemotherapy.
Case Presentation
A 70-year-old female presented to the emergency department with an acute abdomen six days after her last chemotherapy treatment with carboplatin for PPC. She had been diagnosed four years previously with a pelvic tumor, ascites, pleural effusions, and elevated cancer antigen 125 (CA-125). Exploratory laparotomy showed peritoneal carcinomatosis involving the ovaries, although they did not seem to be the primary origin of the tumor. Chest tubes were placed, multiple peritoneal biopsies were taken, and a bilateral salpingo-oophorectomy was performed. Pathology ultimately revealed a diagnosis of a PPC stage IV (pT3b). Tumor cells stained positive for cytokeratin 7 (CK7) and negative for cytokeratin 20 (CK20) on immunohistochemistry. She received six cycles of chemotherapy (carboplatin at a dose of 625 mg in combination with Taxol® (Bristol-Myers Sqibb, New York, NY) at a dose of 135 mg/m2 and dexamethasone at a dose of 20 mg), after which her CA-125 decreased from 200 to 10. She had been progression-free for two years when a surveillance CT scan showed development of ascites and diffuse thickening of the peritoneum. Chemotherapy was restarted (carboplatin at a dose of 588 mg together with gemcitabine at a dose of 400 mg/m2) with an initial response, however, she then developed pancytopenia necessitating discontinuation of gemcitabine. One year later, she experienced several bouts of small bowel obstruction requiring hospitalization, all of which resolved without surgical intervention. She developed a pulmonary embolism and anticoagulation with warfarin was started.
Upon admission to our emergency department after another year, her white blood cell count (WBC) was 9.8 and her international normalized ratio (INR) was 2.5. Computed tomography scan showed intra-abdominal free air and free fluid, and loops of small bowel contracted dorsally as a result of tumor infiltration into the mesenteric root (Fig. 1). The decision for emergency laparotomy after administration of fresh frozen plasma was made. Intra-operatively, a large amount of small bowel content and free air was found in the peritoneal cavity; peritonitis was present. The abdomen was rinsed with warm saline and the small bowel was inspected in its entirety. Diffuse peritoneal carcinomatosis involving visceral and parietal peritoneum was present. An initial attempt to perform adhesiolysis was aborted because of the massive tumor infiltration. The perforation was found at the mesenteric insertion of a proximal small bowel loop (Fig. 2). Closer inspection revealed a 1 cm ulcer with necrotic rims. The necrotic tissue was excised and the lesion closed in a standard double layer fashion. Peritoneal biopsies were taken from the upper and lower abdominal peritoneum. On pathologic examination, the upper peritoneal biopsy showed infiltration of the previously diagnosed PPC, and the excised ulcer showed infiltration of the same malignancy with extensive necrosis present (Fig. 3). Gram staining of the peritoneal fluid showed mixed gram-negative and gram-positive bacteria; cultures grew Candida albicans. Ertapenem and fluconazole had been empirically begun after the initial cultures were drawn. The post-operative course was complicated by paralytic ileus, which resolved after one week. The patient was discharged after 10 d in satisfactory condition, and outpatient chemotherapy was restarted. The patient died from tumor progression five months later.
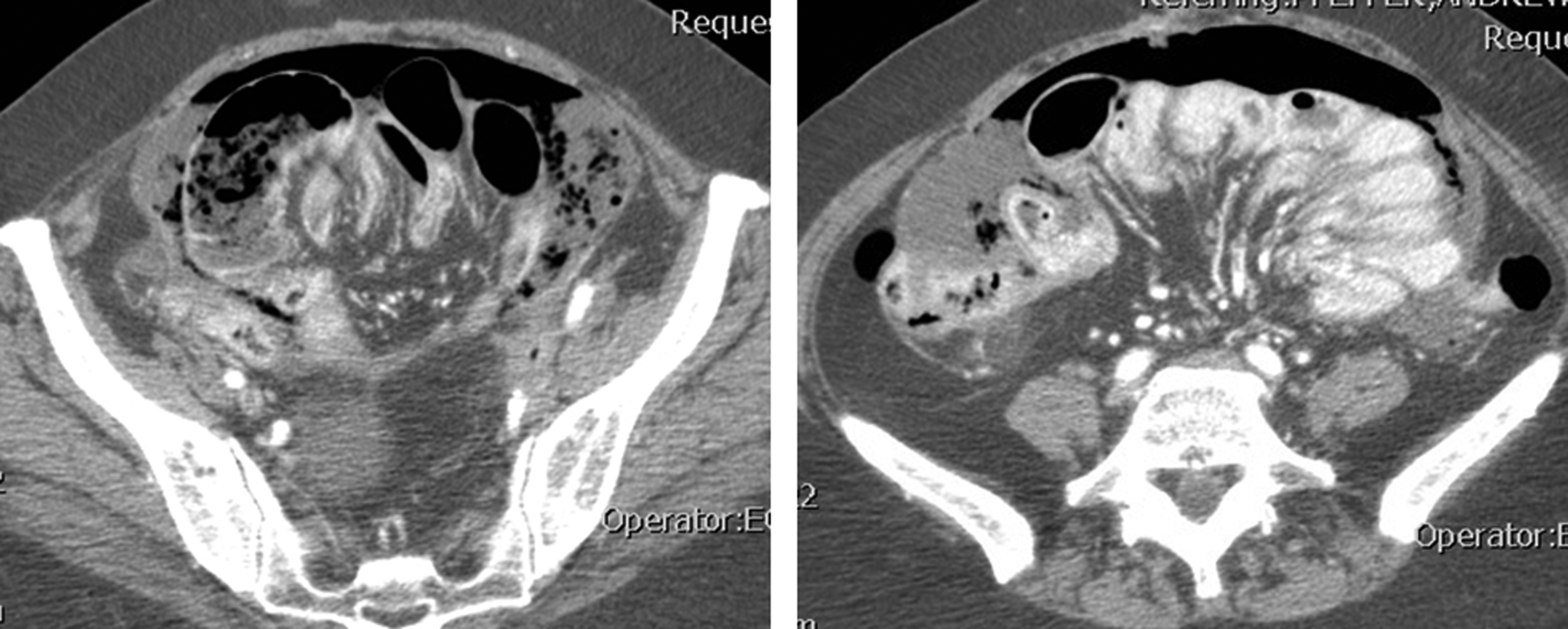
Abdominal computed tomography (CT) scan. Free air and fluid, massively thickened peritoneum.
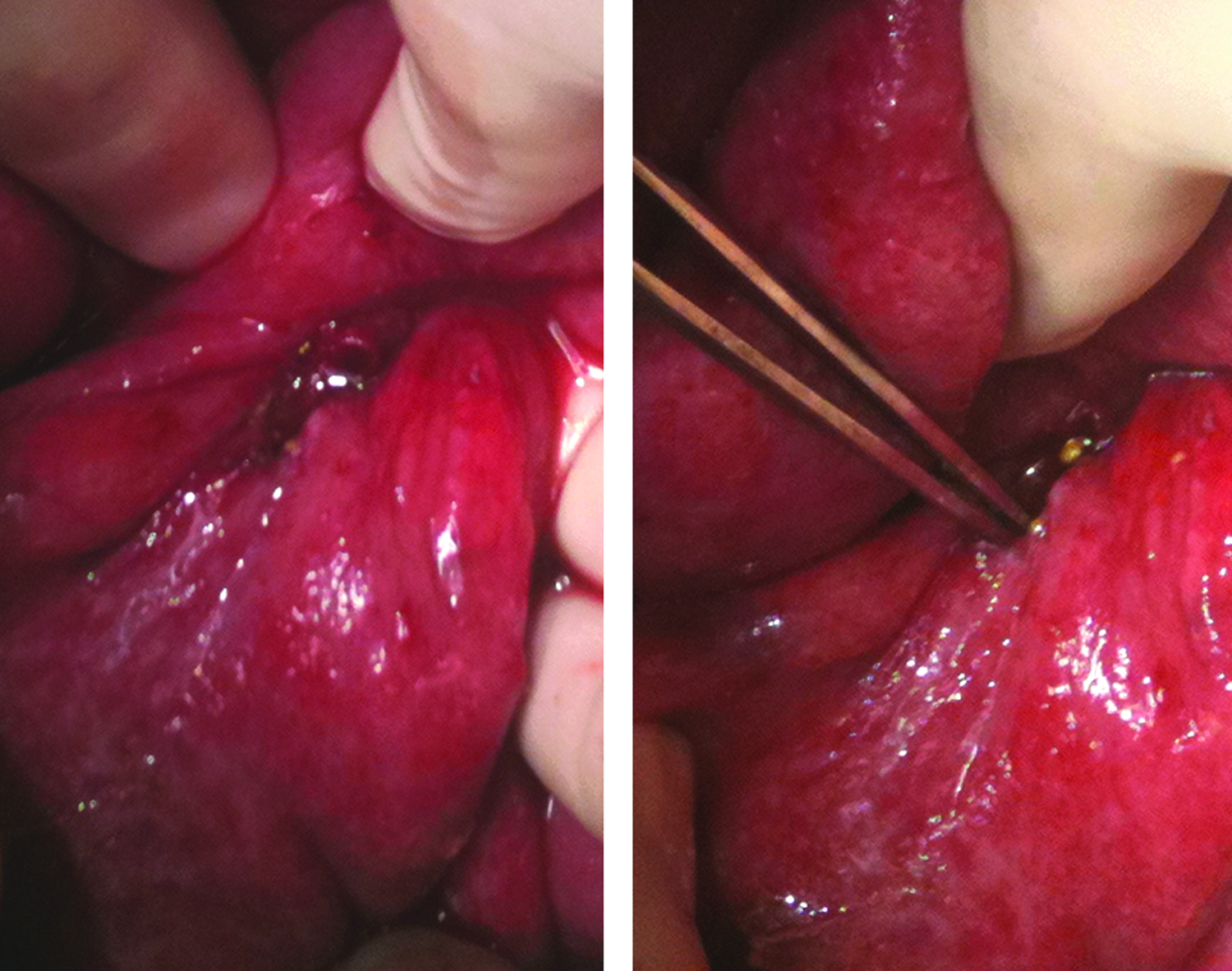
Intra-operative findings. Small bowel loop with peritoneal carcinomatosis and perforation (forceps).

Histopathology. (
Discussion
We herein report a small bowel perforation caused by tumor lysis after chemotherapy in a patient suffering from a rare malignancy. The vast majority of cases of PPC have been published in the gynecology literature [16], however, this type of cancer has also been described in male patients. Common presentations include pelvic masses, massive ascites, and hydrothorax [1]. General surgeons may be involved in the treatment of this malignancy in the case of surgical complications such as hydrothorax, ileus, and perforation, among many others. In addition, therapy-related complications may also occur. Indeed within two months of the described case a second patient with PPC was admitted to our hospital with an acute abdomen that was caused by a perforated peptic ulcer. Small bowel perforation as a consequence of tumor lysis is a rare event, however, various types of cancers and several agents have been linked to this complication. Management consists of source control with either primary closure of the leak or partial bowel resection with or without diversion. In our case, it was decided not to perform a resection but rather an excision of the necrotic ulcer with primary closure of the enterostomy. A resection would have involved mobilization of a significant portion of the small bowel with high risk of injury to the bowel as a result of the massive tumor infiltration of the mesentery. Surgeons should be aware of the potential complications of this rare tumor. In addition, a recent article emphasized a high probability of severe side effects including bowel perforation with use of more aggressive chemotherapy against ovarian, primary peritoneal, and fallopian tube cancer [17]. Nevertheless, because of the relatively good prognosis, all attempts should be made to treat surgical diseases and complications in patients with PPC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.