
Abstract
Abstract
Background:
Persistent omphalomesenteric remnants are diagnosed most commonly in childhood. The condition is rare in adults with only a few cases of laparoscopic management reported thus far.
Case Presentation:
A 32-year-old male underwent open umbilical hernia repair without mesh at an outside hospital. He developed an abdominal wall phlegmone followed by a chronic umbilical infection. Computed tomography (CT) scan showed a tubular structure at the inner surface of the abdominal wall suggestive of a urachus cyst. During laparoscopy, the tubular structure was found to have no relation to the bladder but instead could be followed toward the small bowel originating 100 cm proximal to the terminal ileum. The chronic infected umbilical fistula was resected, and at the origin the duct was excised longitudinally and the enterotomy was closed transversely. The patient developed a superficial surgical site infection but ultimately did well.
Discussion:
Surgeons should be aware of this rare condition as a cause of chronic umbilical infection. The omphalomesenteric remnant is suitable for laparoscopic repair.
The persistent omphalomesenteric remnant (OER) is a rare condition diagnosed most commonly in childhood [1] that causes chronic abdominal wall infections, abdominal pain, and small bowel obstruction. Pathologies associated with the primitive yolk stalk are summarizes as vitelline duct anomalies [2,3]. In contrast to the Meckel diverticulum, in OER a connection with the umbilicus persists. It is rarely seen in adults and only few cases of laparoscopic management have been reported thus far [4–6]. Chronic umbilical infection may be one of the clinical presentations.
Case Report
A 32-year-old male underwent open primary repair of an umbilical hernia without mesh at an outside hospital. After the procedure he developed a chronic umbilical infection treated with antibiotics and dressing changes. The infection progressed and an abdominal wall phlegmone developed. Computed tomography (CT) scan demonstrated a tubular structure adherent to the inner surface of the abdominal wall associated with the soft tissue infection (Fig. 1). It was suggested that a urachus cyst may be causing the chronic infection. Antibiotics were administered and the patient improved but had persistent drainage from his umbilicus. He was consented for laparoscopic exploration and removal of the pathology. Three 5-mm trocars were placed in the left abdomen. Omental adhesions to the abdominal wall were divided. The reported tubular structure was identified and had no relation to the bladder but could be followed toward the mesenterium and developed into a small bowel loop (Fig. 2). An OER was suspected and the small bowel was inspected. At 100 cm proximal to the terminal ileum the origin of the OER was identified. A feeding artery was clipped and a 4-cm peri-umbilical incision was made including the chronic fistulizing infection. Three prolene stitches from his umbilical hernia repair were also removed. The fistula with the entire duct was brought out of the abdomen. At the origin, the OER was resected (Fig. 3) longitudinally and the enterotomy was closed transversely in two layers. The abdominal wall was closed with interrupted absorbable sutures; the skin was left open. The patient recovered well from his operation, however, he developed a superficial surgical site infection requiring local therapy. After four weeks the incision healed and the patient was well at his three month follow-up.

Computed tomography (CT) scan: Tubular structure attached to the infraumbilical abdominal wall with local inflammation.
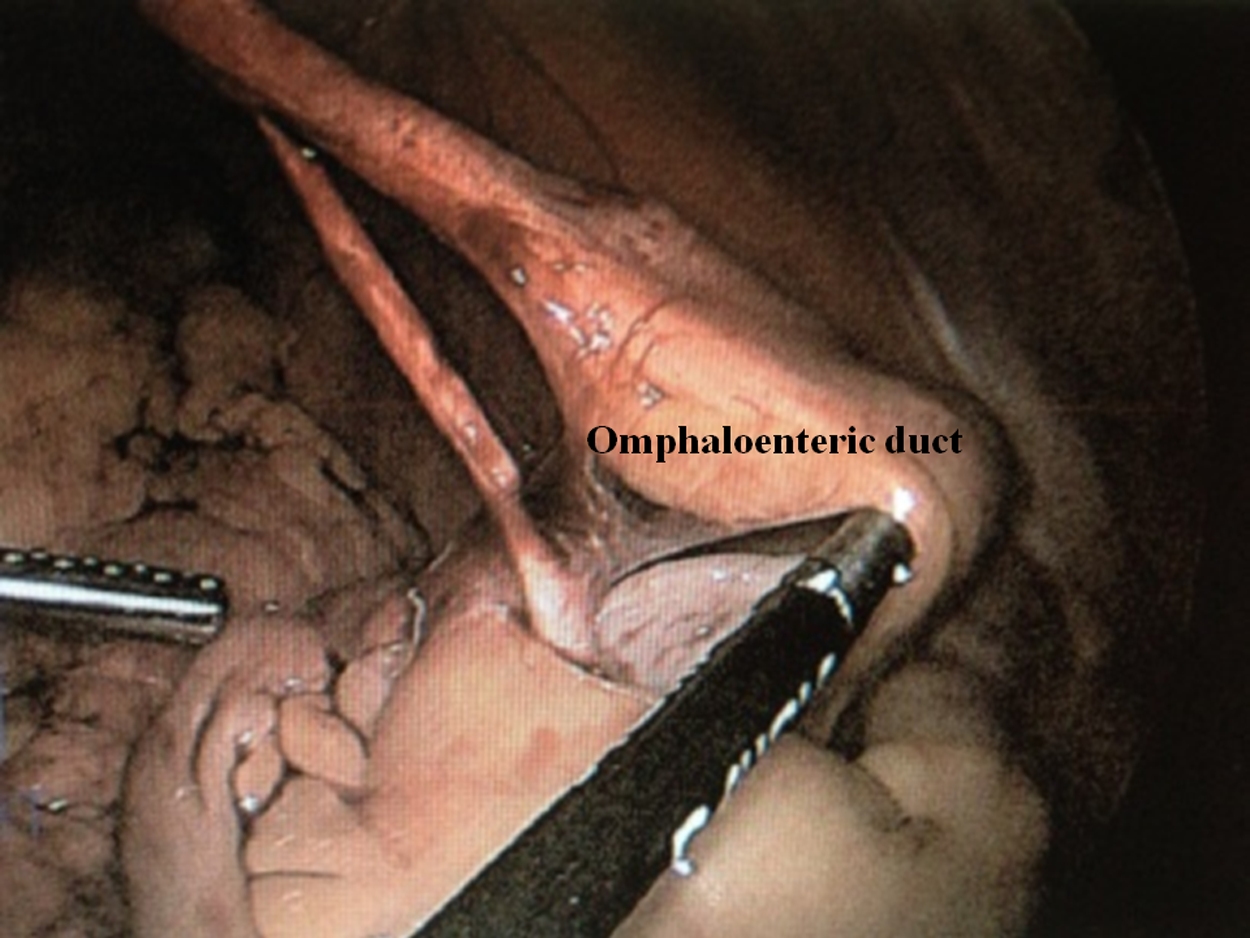
Intra-operative findings: the tubular structure can be followed to the ileum.

Specimen with omphaloenteric duct and chronic fistula.
Discussion
Surgeons should be aware of the rare condition of an OER. In our case, initial presentation was an umbilical hernia and subsequently a chronic infection, which progressed to an abdominal wall phlegmone. On CT scan a urachus cyst was suspected; diagnosis of the OER was made intra-operatively. The anomaly was resected using a laparoscopic approach.
Most malformation associated with the OER present as a Meckel diverticulum [1]. A persistent OER is much less frequent and in adults extremely rare with small bowel obstruction, gastrointestinal bleed, abdominal pain, umbilical hernia, and chronic umbilical drainage being presenting symptoms [7–9]. Computed tomography scan should detect the OER but as in our case it may be difficult to distinguish from a urachus cyst especially in the presence of post-infectious changes.
If symptomatic, the OER should be removed [10]. Laparoscopic approach has been shown to be safe and feasible leaving only a small incision for extraction of the resected specimen. In our case the fistula was used for the mini-laparotomy and resection and closure of the enterotomy were done extracorporeally. Despite excision of the chronic fistulizing infection and antibiotics and leaving the incision open, our patient developed a superficial surgical site infection, which was treated successfully with local therapy. We confirm that the OER is suitable for laparoscopic repair.
Footnotes
Author Disclosure Statement
No competing financial interests exist.