
Abstract
Abstract
Background:
Ascaris lumbricoides is a common nematode infection that has not been associated previously with the development of gallbladder carcinoma.
Case Presentation:
A 73-year-old Filipino female who had immigrated recently to the United States presented to the emergency department with right upper quadrant abdominal pain associated with nausea and emesis. Her laboratory data were significant for a mild transaminitis and a computed tomography (CT) of the abdomen showed a dilated gallbladder with a non-mobile, heterogenic mass concerning for a gallbladder neoplasm. She underwent open cholecystectomy and was found to have a live Ascaris lumbricoides in her common bile duct. She did well post-operatively and was treated with albendazole for her Ascaris infection.
Discussion:
Liver fluke infection has previously been implicated as a cause of biliary carcinoma secondary to chronic inflammation. However, our patient was infected with Ascaris lumbricoides, which has not been associated previously with gallbladder carcinoma. Chronic inflammation from an active Ascaris infection may have contributed to the development of gallbladder carcinoma in a similar manner as is observed with liver fluke infection
Gallbladder carcinoma is a rare but noted deadly carcinoma with overall five-year mortality reported to be as high as 80% depending on the stage at diagnosis [1]. Multiple risk factors for gallbladder carcinoma have been identified and include age, smoking, and presence of gallstones [1,2]. One infectious cause that has been associated with an increased risk of gallbladder carcinoma is infection with the liver flukes Clonorchis sinensis and Opisthorchis viverrini [1]. This is believed to be from chronic inflammation of the biliary tract.
Although liver fluke infection has been associated with the development of biliary cancer, infection with nematodes, such as Ascaris, has not been described previously. Ascaris is a common nematode worldwide, with a reported infection rate of 1.2 million [3]. Infection with Ascaris ranges from asymptomatic to abdominal pain secondary to bowel obstruction [4,5]. On review of the literature, we were unable to identify any infection with Ascaris in association with gallbladder carcinoma. We herein report a case of concomitant Ascaris infection and gallbladder carcinoma.
Case Presentation
We present the case of a 73-year-old Filipino female who presented to the emergency department with a four-day history of worsening right upper quadrant abdominal pain associated with nausea and emesis. She had immigrated recently to the United States from the Philippines. On examination, she was noted to have normal vital signs. She exhibited abdominal tenderness in the right upper quadrant without guarding but was noted to have a negative Murphy sign. Her laboratory data revealed a normal white blood cell count. Her liver function tests revealed a mild transaminitis with an aspartate aminotransferase (AST) and an alanine aminotransferase (ALT) of 118 and 118, respectively, and an alkaline phosphatase of 269. Her bilirubin was normal. Computed tomography (CT) of the abdomen and pelvis as well as an abdominal ultrasound showed a dilated gallbladder with a non-mobile, heterogenic mass concerning for a gallbladder neoplasm (Fig. 1). Her common bile duct was dilated to 1.5 cm. She was admitted for rehydration and pre-operative medical clearance. A magnetic resonance cholangiopancreatography (MRCP) was obtained that correlated with the CT findings and did not show invasion of the mass into the liver. Tumor markers CA-19-9 and CEA were also obtained and were normal.

Axial computed tomography (CT) showing dilated heterogeneous gallbladder (arrowhead) with distended common bile duct (arrow)
The patient was brought subsequently to the operating room for a radical cholecystectomy. This was attempted laparoscopically initially but was soon converted to an open procedure given the inability to retract the gallbladder cephalad. Her gallbladder was thickened and woody in appearance. After transection of her cystic duct, inspection of the common bile duct revealed an intra-luminal entity that resembled a worm (Fig. 2). There was no evidence of hepatic invasion and intra-operative frozen sections were negative for malignancy. The patient did well after surgery and was discharged home on post-operative day five.
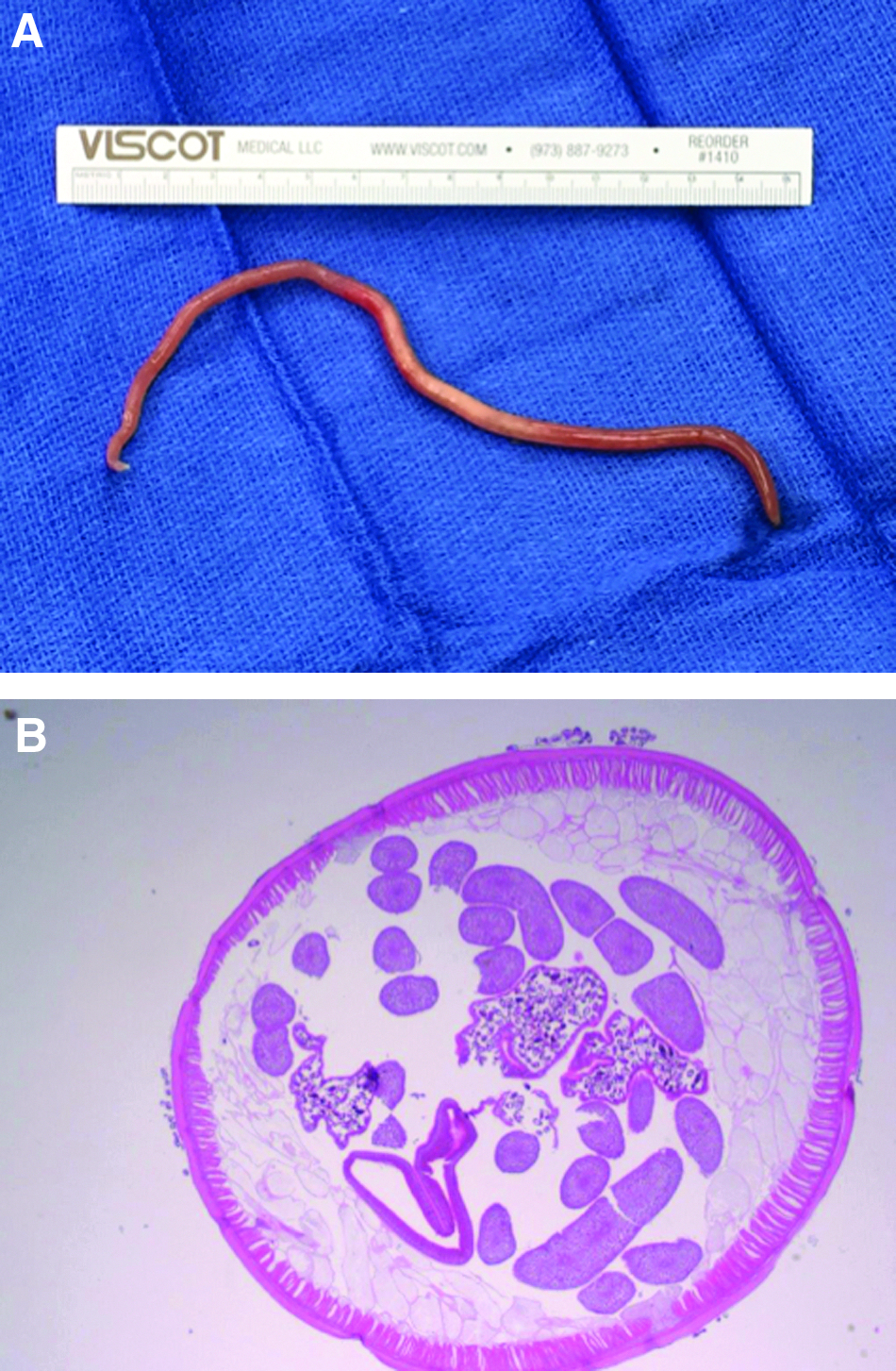
Ex vivo image of Ascaris lumbricoides (
The patient's pathology returned as T1bN0 gallbladder carcinoma with negative margins. The common bile duct intra-luminal mass was a female Ascaris lumbricoides. The patient was treated subsequently with a course of albendazole for the nematode infection.
Discussion
We present the concomitant presence of gallbladder carcinoma and Ascaris lumbricoides infection. Although chronic infection with liver flukes such as Clonorchis sinensis and Opisthorchis viverrini is a known risk factor for the development of cholangiocarcinoma, the documented association between the nematode Ascaris lumbricoides and cholangiocarcinoma or gallbladder carcinoma is not well documented [1,6,7]. We were unable to identify any cases of gallbladder carcinoma and Ascaris infection and thus, we believe this is the first reported case of gallbladder carcinoma associated with Ascaris lumbricoides infection.
Adult Ascaris species live primarily in the duodenum or proximal jejunum and can grow to up to 35 cm in length [8,9]. The organism is transmitted via the fecal–oral route [10,11]. Once the eggs are ingested, they hatch in the intestine of the host organism [10,11]. The larvae then penetrate the mucosa and invade the blood stream [10,11]. This allows the larvae to be carried to the lung where they undergo the next stage of their life cycle and mature in the alveolar capillaries [10,11]. Their presence stimulates respiratory clearance mechanisms allowing for the larvae to move to the epiglottis where they are then commonly swallowed and re-enter the small intestine to complete their development to adulthood before being passed in the host's stool [8,9].
Ascaris infections are usually asymptomatic, but a large burden of infection may result in abdominal pain, especially if there is intestinal obstruction [5]. Ascaris has been noted to infect other sites including the bile duct, liver, and appendix [5,8,12]. There are a few case reports of Ascaris infection and associated extra-hepatic cholangiocarcinoma [6,13]. The inflammatory response to infection may lead to an increased risk of cholangiocarcinoma in a similar manner as is observed with liver fluke infection [1,8]. We suspect that chronic inflammation of the biliary tree may also contribute to the development of gallbladder carcinoma. In the United States, Ascaris infection is uncommon, with some studies suggesting as low as 2% of the population [11]. Our patient had recently immigrated from an area in which Ascaris is endemic, and the reported infection rate ranges from 25%–75% of the population [10,14,15].
To our knowledge, this is the first reported case of gallbladder carcinoma with concomitant Ascaris lumbricoides infection. Our patient presented with symptoms of gallbladder carcinoma, and only during the operation was her infection identified. We hypothesize that the chronic inflammatory state from her helminth infection likely contributed to the development of her gallbladder carcinoma. Although uncommon, the clinician should be aware of such concomitant infections, especially in patient populations in which helminth infection is high as demonstrated in our patient.
Footnotes
Author Disclosure Statement
No competing financial interests exist.