
Abstract
Abstract
Background:
Transrectal ultrasound guided prostate biopsy (TRUS-PB) is a common investigation for assessment of prostatic carcinoma. Loco-regional complications of TRUS-PB are uncommon and usually relate to infective processes from bacteria present in the rectum. We present a novel case of an abscess from a rectal diverticular perforation secondary to TRUS-PB to highlight this complication as a potential concern for this diagnostic modality.
Methods:
We present a 55-year-old male who underwent TRUS-PB for investigation of elevated prostate-specific antigen (PSA) (PSA 3.5ug/l). Three weeks following this procedure, at the hospital, the patient presented with septic shock requiring inotropic support. Computed tomography (CT) identified a contained rectovesical abscess anterior to the upper rectum. The patient required operative intervention as he failed to improve on conservative management. Histopathological assessment confirmed recent perforation through the anterior rectum via a rectal diverticulum.
Results:
Post-operatively, the patient recovered rapidly and was discharged day nine. The patient underwent a laparoscopic-assisted reversal of Hartmann's stoma approximately 8 mo after his initial operation.
A 55-year-old male with comorbid hypertension and depression underwent TRUS-PB for investigation of elevated PSA (3.5 ug/L) (reference range <2.5 ug/L). Prostatic biopsy was performed under transrectal ultrasound (TRUS) guidance. A standard institutional extended biopsy protocol comprising 24 cores, with four cores per peripheral zone sextant and no anterior zone sampling, was performed using an end-firing endorectal probe (Philips C9-5; Philips Healthcare, Amsterdam, the Netherlands). Peri-procedural antimicrobial prophylaxis comprised trimethoprim-sulfamethoxazole 800/160 mg BD one day prior to the procedure and continued for nine days post-procedure per the institutions' standard protocol. Three weeks following biopsy, the patient presented to the emergency department with a five-day history of increasing suprapubic pain, vomiting, chills, and rigors.
Physical Examination and Laboratory Results
On examination, the patient was febrile (39.1°C), tachycardic (135 bpm), and hypotensive (78/50 mmHg) with a clinically benign abdomen and no evidence of peritonism. Digital rectal examination excluded palpable rectal mass or bleeding. The prostate was non-tender, firm, and smooth with no features suggestive of malignant disease. Initial laboratory investigations showed serum leukocytosis (3.5×109/L), neutrophillia (3.28×109/L), thrombocytopaenia (88×10 9/L), hyponatraemia (Na 124 mmol/L), and hypokalaemia (2.5 mmol/L) with an International Normalized Ratio (INR) of 1.6. Arterial blood gas examination suggested a compensated respiratory alkalosis (serum lactate 2.8 mmol/L).
Diagnosis
Computed tomography imaging (Phillips Brilliance 64-slice CT Scanner; Philips Healthcare, Amsterdam, the Netherlands) of the abdomen using intravenous contrast demonstrated a collection within the rectovesical recess containing both fluid and gas measuring 37 mm x 59 mm (Figs. 1 and 2). Microbiological testing isolated anaerobic gram-positive bacilli and Bacteroides fragilis on blood cultures taken at admission (sensitive to metronidazole), despite negative urine culture.
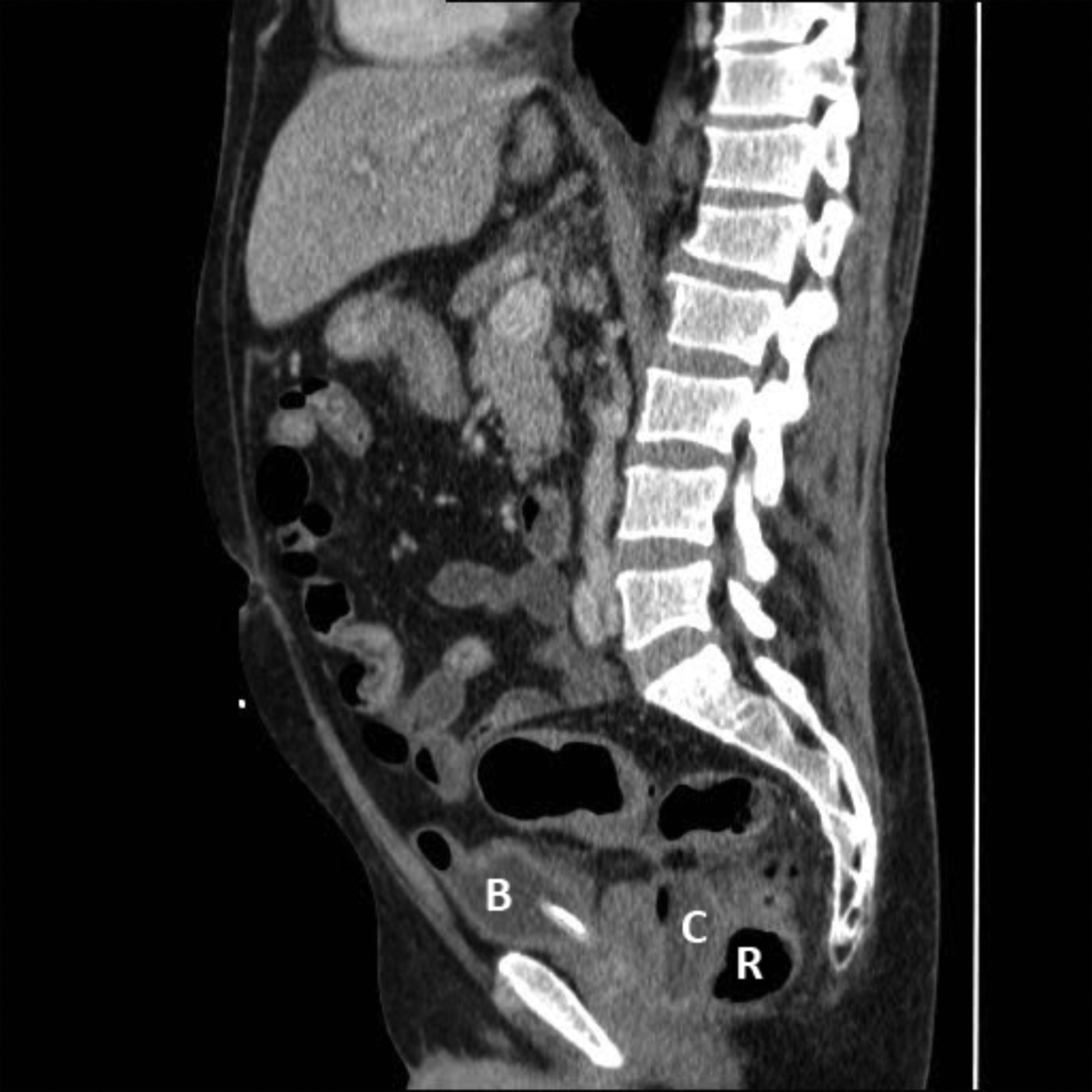
Sagittal view of a computer tomographic scan of the patient (B: bladder; C: collection; R: rectum).

Axial view of a computer tomographic scan of the patient (B: bladder; C: collection; R: rectum).
Intervention
The patient responded well following initial fluid resuscitation and empiric antimicrobial therapy (piperacillin-tazobactam 4.5 g) and was managed conservatively. Interventional radiological expertise to drain the pelvic abscess percutaneously under image guidance was not available at this facility.
Increasing abdominal pain and inotropic requirement in the setting of ongoing sepsis prompted operative management on day two. Initial diagnostic laparoscopy was converted to laparotomy following identification of fecal contamination of the peritoneum. Intra-operatively, an abscess cavity was identified between the upper rectum and posterior bladder wall. This was surrounded by dense fibrous tissue and adhesions, involving the left seminal vesicle and closely abutting the left ureter. A visible perforation was noted in the anterior wall of the middle third of the rectum. A Hartmann's operation with the lower border of resection extending to the middle rectum and a diverting colostomy was completed to limit the contamination. Histologic examination revealed multiple rectal diverticulae, one of which demonstrated a macroscopic perforation. Microscopically, extensive organizing peritonitis, fibrosis, and fibrous adhesions were observed on the operative specimen.
Outcomes
The patient was extubated on day four and subsequently discharged home on post-operative day nine. The prostate biopsy histology demonstrated benign prostatic glands and stroma. The patient was referred to a tertiary hospital where he underwent a laparoscopic assisted reversal of Hartmann's stoma approximately eight months after his initial operation.
This novel case of rectal diverticulum perforation following TRUS-PB resulting in pararectal abscess and sepsis illustrates the substantial morbidity suffered by a small proportion of patients undergoing this procedure [1,2,3]. Unlike colonic diverticula, rectal diverticula are uncommon, with only sporadic reports in the medical literature since 1911 [4], and may predispose to infection as a result of this procedure.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflict of interest regarding the publication of this paper. No funding was received for the purpose of this case report.