
Abstract
Abstract
Background:
Littre's hernia is the type of hernia where the sac contains Meckel's diverticulum, which is associated with various complications. Strangulation of Meckel's diverticulum and consequent rupture represents a serious and life-threatening condition.
Methods:
A 62-year-old female, with a 10-d history of abdominal pain, presented in the emergency department with abdominal pain in the past 48 h, accompanied by fever and vomiting. Clinical examination revealed diffuse abdominal pain and an inflamed mass on the right groin. Given the clinical and laboratory findings the patient was taken in the operating room.
Results:
Diagnostic laparoscopy revealed Littre's hernia accompanied by rupture of Meckel's diverticulum and abscess formation. Because of multiple adhesions and distension of the small bowel, the operation proceeded with open laparotomy, including a sub-umbilical midline incision. Enterectomy and side-to-side anastomosis was performed and the abscess was drained. The post-operative period was uneventful and the patient was symptom free at the two-month follow-up.
Conclusions:
An inguinal abscess can represent the first manifestation of a strangulated Meckel's diverticulum in Littre's hernia. It should be taken into account in the differential diagnosis of acute abdomen symptoms. Prompt diagnosis and therapy is essential. The preferred treatment is an operation consisting of enterectomy and primary anastomosis.
Littre's hernia is the protrusion of Meckel's diverticulum through an abdominal opening [1,2]. Meckel's diverticulum is the most common congenital malformation of the gastrointestinal tract, occurring in 2%–3% of the population [2]. Despite the availability and wide use of modern imaging techniques, the diagnosis of Meckel's diverticulum remains elusive [3,4].
This is the case of a female patient who presented in the emergency department with an inflammatory mass in the right groin and, intra-operatively, she was diagnosed with Littre's hernia accompanied by rupture of Meckel's diverticulum and abscess formation.
Case Presentation
A 62-year-old female presented in the emergency department with acute abdominal pain accompanied by fever and vomiting. According to her medical history, she had mild abdominal pain the past 10 days, which deteriorated within the past 48 h. There was no history of chronic disease or previous operations on the abdomen.
Physical examination revealed abdominal distention, tympany, and reduced bowel sounds. A tender mass was detected in the right inguinal area and it presented inflammatory characteristics. The patient had a temperature of 39°C, blood pressure of 120/80 mmHg, 110/min pulse, and the oxygen saturation was 97%. The laboratory exams ordered were: Hct: 49%, Hb: 16g/dL, plt: 363.000/μL, wbc: 25.800/μL (neu: 90%), c-reactive protein: 280. Urine examination revealed leukocytouria. Chest radiography did not reveal any pathologic findings while the abdominal X-ray revealed multiple air fluid levels (Fig. 1).

Multiple air fluid levels in abdominal radiograph.
The patient was admitted to the hospital and was supported with intravenous fluids and antibiotics. Given the anatomic position of the mass, an incarcerated inguinal hernia was posed as more probable in the differential diagnosis and the patient was taken to the operating room. A diagnostic laparoscopy was performed in order to verify the initial diagnosis. The intra-operative findings revealed a distended small bowel. While inspecting the peritoneal cavity, a portion of the ileum was discovered to be incarcerated on the right internal inguinal ring, approximately 60 cm from the ileocecal valve.
The operation proceeded with a sub-umbilical midline incision. A portion of the incarcerated ileum was restored and Meckel's diverticulum was discovered to be herniating into the right internal inguinal ring (Fig. 2). While replacing Meckel's diverticulum, pus was released from the internal inguinal ring, and consequently, extended rinsing of the peritoneal cavity was performed with normal saline solution. The segment of ileum that contained Meckel's diverticulum was resected and the intestinal continuity was re-established with a side-to-side anastomosis using a GIA stapler (Fig. 3). A drain was placed in the right groin and the abdomen was sutured. A right inguinal incision was performed on the inflammatory mass and a great amount of pus was released. The underlying cavity was rinsed and the wound was left open to heal by secondary intention. The post-operative course was uneventful and the patient was discharged from hospital on the post-operative day 6. At two-months follow-up the patient was symptom free.
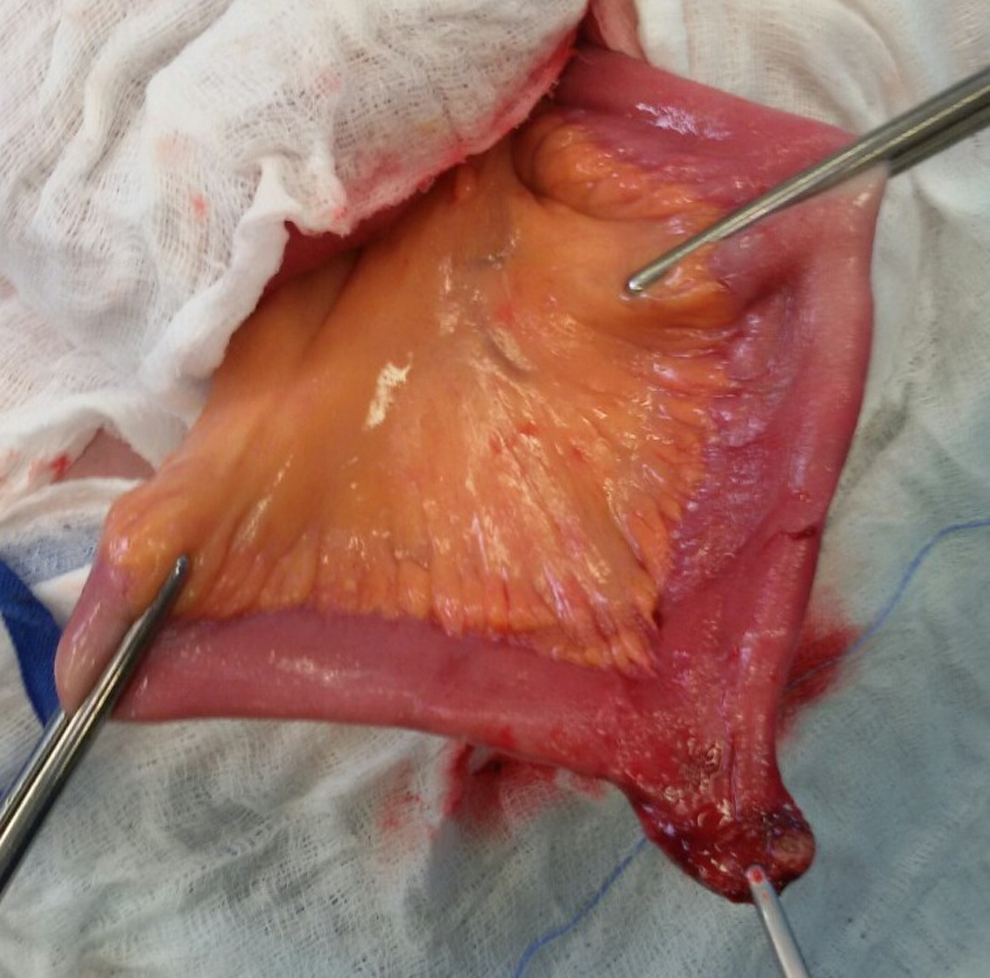
Meckel's diverticulum herniating into the right inguinal ring.

Surgical specimen including segment of ileum and Meckel's diverticulum.
Discussion
In 1700, Alexis Littre, a French surgeon, was the first to report two cases of inguinal hernia in which an intestinal diverticulum was the sole occupant of the sac. In 1841, Rieche suggested that the name that should be given to the hernias was Littre's hernias [1]. When the sac contains a Meckel's diverticulum alone, the hernia is called true Littre's hernia, but a mixed Littre's hernia contains ileum or other abdominal viscera as well [1].
Littre's hernia occurs in 50% of the inguinal region, in 20% of the umbilicus, in 20% of the femoral area, and in 10% of the remaining locations [2]. In this case report, the hernia occurred in the right inguinal groin.
In symptomatic Littre's hernia the patient presents with a mass and the pre-operative diagnosis is difficult to establish even with computerized tomography (CT). Pain, fever, and vomiting are the main symptoms when intestinal obstruction is present [2]. The female patient in this case had pain, fever, and vomiting as the principal symptomatology that led her to the hospital. Imaging consisted only of an abdominal X-ray because computerized tomography was not available due to technical problems. The management of Littre's hernia consists of Meckel's diverticulum excision. In presence of edema or inflammation at the base of the diverticulum, resection and anastomosis of this segment of the ileum is necessary [2]. In this case report, enterectomy and anastomosis were performed because of necrosis, perforation, and inflammation of the diverticulum.
Meckel's diverticulum is a true intestinal diverticulum that is created by improper closure of the omphalomesenteric duct [2,3]. In intra-uterine life this structure connects the primitive gut with the yolk sac of the embryo and normally regresses between the fifth and seventh week of fetal life [2–4].
Meckel's diverticulum was first described by Fabricius Hildanus in 1598, but the name was given by the German anatomist Johann Fredrich Meckel, who described the embryological and pathological features of this structure in 1809 [3,4]. The true incidence of Meckel's diverticum is unknown, but most studies suggest an incidence of between 0.6% and 4% [4].
Meckel's diverticulum is located on the anti-mesenteric border of the ileum, 10 cm to 150 cm proximal to the ileocecal valve and is usually 3–5 cm long [2,3]. In this case report, the diverticulum was located approximately 60 cm from the ileocecal valve.
As mentioned previously, Meckel's diverticulum is a true intestinal diverticulum, meaning that it has all normal layers of the intestinal wall [3]. However, ectopic tissue can also be found, such as gastric mucosa (50%), pancreatic mucosa (5%), and less commonly, colonic mucosa, endometriosis, and hepatobiliary tissue [2].
As far as the characteristics of Meckel's diverticulum are concerned, some surgical textbooks quote the “rule of 2s”: 2% of the population have the abnormality, it is often found in children under 2 years of age, it affects males twice as often as females, it is usually found within 2 feet (60 cm) of the ileocecal valve, and it is approximately 2 inches (5 cm) in length [3,4].
In the majority of cases, Meckel's diverticulum remains silent and is usually diagnosed incidentally during laparoscopy or laparotomy performed for non-related conditions [2,3]. However, this entity can cause life-threatening complications [2]. According to Meckel, the incidence of complications due to Meckel's diverticulum was 25%, but in the recent literature it ranges from 4%–16% [4]. Complications are much more common in males (males/females: 1.8–4/1) [3]. Complications decrease with the age, with the majority of them occurring in the pediatric population [2,3]. The most common complications are obstruction (36.5%), intussusception (13.7%), diverticulitis (12.7%), hemorrhage (11.8%), perforation (7.3%), neoplasm (3.2%), and fistula (1.7%) [2]. In the differential diagnosis of a complicated Meckel's diverticulum, appendicitis must always be considered and should be excluded [3].
Conclusion
A complicated Littre's hernia can be rare but it can represent a serious clinical disorder, because it can lead to life-threatening conditions, such as bowel obstruction, intestinal ischemia with consequent necrosis, and peritonitis. It should always be taken into account in the differential diagnosis of an inguinal abscess. The preferred treatment is an operation, primarily enterectomy and primary anastomosis. In cases of concomitant presence of abscess, an incision and drainage should always be performed.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest.