
Abstract
Abstract
Background:
Nosocomial infections play a major role in the morbidity and mortality of surgical patients. Nosocomial fungal infections are particularly difficult to treat and may present in a cryptic manner. We report a case of iatrogenic Candida glabrata necrotizing adrenalitis after endoscopic ultrasound (EUS) retroperitoneal cyst aspiration.
Case Presentation:
A 43-year-old female with history of hepatitis C presented with an incidental 6.0 cm retroperitoneal cyst found on magnetic resonance imaging (MRI) believed to be arising from the pancreas. The patient underwent EUS-assisted cyst aspiration for tissue diagnosis, however, these results were inconclusive. She underwent laparoscopic resection of the left retroperitoneal cyst along with the attached left adrenal gland. Histopathology revealed no malignant disease or pancreatic cyst; instead, the cyst originated from the adrenal gland and budding yeast was discovered in the cyst. 28S ribosome polymerase chain reaction (PCR) sequencing revealed C. glabrata adrenalitis. The patient was treated with micafungin for two weeks and had no complications.
Conclusion:
This case demonstrates that introduction of fungal species through endoscopy can occur and also highlights the problem with iatrogenic introduction of micro-organisms with EUS cyst aspiration.
Nosocomial infections have become one of the most problematic scenarios in the field of surgery. With the ever-increasing issue of microbial resistance to antibiotics, nosocomial infections play a role in the morbidity and mortality of surgical patients. In the subset of nosocomial infections, nosocomial fungal infections (NFI) are particularly important. Patients who present typically with either frank fungal infection or colonization are usually immunosuppressed individuals such as patients infected with the human immunodeficiency virus (HIV), patients with neutropenia, patients who are hospitalized long term, and patients receiving total parenteral nutrition (TPN) therapy. Nosocomial fungal infections remain one of the most difficult entities to treat. This is in part because of emerging drug-resistant Candida spp. that are less responsive to traditional systemic anti-fungal therapy. Three major mechanisms of anti-fungal resistance exist. These include decreasing the effective drug concentration by means of increased drug efflux, drug target alteration methods, and metabolic bypasses [1].
The Candida sp. genus remains the most common NFI occurring in the United States [2]. Candida sp. nosocomial infections range from urinary tract infections to central line blood stream infections. Although Candida albicans is the most common species of NFI, its two “evil stepsisters” C. glabrata and C. tropicalis have become important fungal infections especially in terms of increased drug resistance of fungal species. An increase in resistance to azole therapy has made these two species of Candida difficult to treat. We report a patient who underwent endoscopic ultrasound (EUS) retroperitoneal cyst aspiration and subsequent left retroperitoneal cyst/adrenal gland resection who was found on pathology to have necrotizing C. glabrata adrenalitis confirmed via 28S ribosome polymerase chain reaction (PCR) sequencing. This was likely caused by the introduction of Candida species from the EUS instrumentation.
Case Presentation
We report a 43-year-old female with a history of hepatitis C who was found to have a left retroperitoneal cyst on her workup for hepatitis C. Magnetic resonance imaging (MRI) revealed a 6.0 cm cyst near the tail of the pancreas. (Fig. 1) After full evaluation by her gastroenterologist, the patient underwent EUS cyst aspiration to obtain a possible diagnosis. The cyst aspiration results showed abundant proteinaceous material with scattered macrophages. There was no evidence of malignant cells or thick mucin pools. At the recommendation of the multi-disciplinary gastrointestinal tumor board, surgical excision of the retroperitoneal cyst was performed. Pre-operatively, the patient was not on any immune-altering therapy. Intra-operatively, it was found that the retroperitoneal cyst was attached to the adrenal gland. The retroperitoneal cyst and attached left adrenal gland were taken as one specimen. There was no evidence of gross necrosis or unique pathology to the adrenal cyst/gland.

T2 magnetic resonance image (MRI) showing 6.0 cm adrenal cysts.
On histopathologic examination of the cyst, it was found to be adrenal in origin and infected with a budding yeast specimen; necrotizing adrenalitis was also reported (Figs. 2 and 3) At this time, the infectious disease department was consulted and recommended β-D-glucan assay, HIV testing Histoplasma titers, and itraconazole. The Fungitell® assay (Associates of Cape Cod, Inc., East Falmouth, MA) value was 39 pg/mL (normal value, <90 pg/mL). The patients was HIV negative and her Histoplasma titers were also negative. The patient underwent an echocardiogram, which was negative for any valvular lesions. She was discharged home on post-operative day 10 with itraconazole therapy. 28S ribosomal molecular testing revealed the presence of Candida glabrata genes and was consistent with a diagnosis of iatrogenic fungal adrenalitis from EUS manipulation. The patient was switched from itratroconazole to micafungin for an additional two weeks. She had no complications or clinical evidence of fungemia. The previous initial aspirate cytology specimen was stained for fungal Gomori methenamine silver/periodic acid-Schiff (GMS/PAS), which were negative.

Hematoxylin and eosin stain of the pseudocyst cavity is lined by a proteinaceous and fibrinopurulent inflammatory exudate with scattered foamy histiocytes, and clusters of fungal yeast.
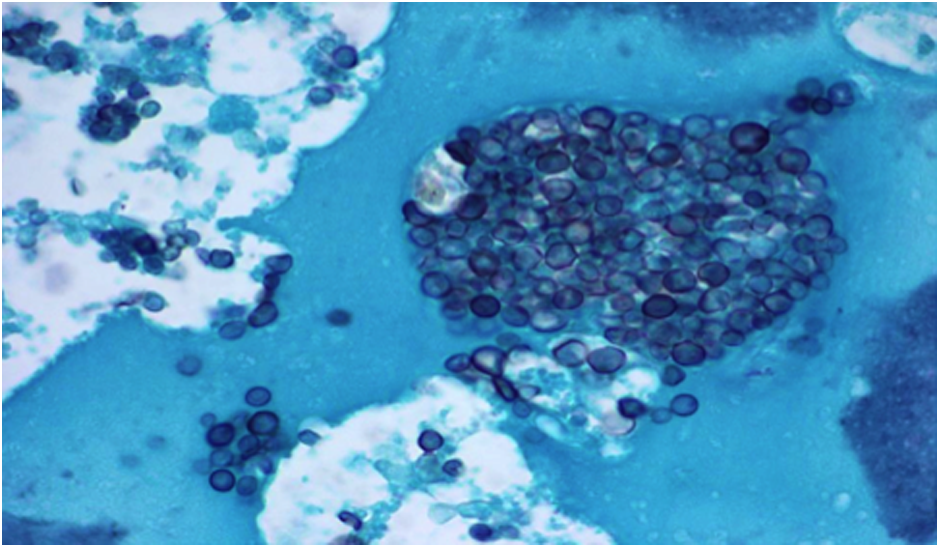
Gomori methenamine silver (GMS) stain showing fungal cysts.
Discussion
Fungal adrenalitis is an uncommon diagnosis. Patients who develop fungal adrenalitis are usually immunosuppressed patients, however, there have been reports of bilateral adrenal Histoplasma sp. infection in immunocompetent patients [3]. Endocarditis can also seed infection to the adrenal glands by means of septic emboli. Our case demonstrates two unique features. First, reports of fungal adrenalitis with Candida sp. are limited in the literature. Second, the iatrogenic nature of the infection highlights the ever growing prevalence of noscomial infections with endoscopy.
In regards to achieving a diagnosis of fungal adrenalitis, we used 28S ribosome PCR sequencing to confirm the pathogen. Mutiple laboratory methods exist to identify Candida sp. These include routine blood and laboratory cultures, β-D-glucan detection, multi-locus sequence typing, pulsed field gel eletrophoresis, microsatellite analysis, and random amplication of deoxyribonucleic acid (DNA) [4]. Multiple articles have outlined the poor yield of routine blood culture and β-D-glucan blood tests. Karageorgopoulos et al. [5] demonstrated the overall sensitivity and specificity of β-D-glucan blood test was 75.3% and 85.0%, respectively. Our case demonstrates the variable diagnostic utility of β-D-glucan because our patient's value was normal. However, the use of PCR-based molecular tests allowed us to identify the organism correctly and treat the patient accordingly.
Advances in endoscopic management of achieving tissue diagnosis in cases including thoracic tumors, pancreatic pseudocysts, and foregut masses have made the use of EUS a viable option for diagnostic purposes. The use of these endoscopic techniques spares the patient from open surgical biopsy, which may cause more morbidity, increase hospital length of stay, and may increase pain to the patient. However, complications of EUS include esophageal perforation, infections, and failure to achieve diagnostic result as a result of sampling [6]. Although Eloubeidi et al. [7] calculated the sensitivity and specificity of endoscopic-guided fine-needle aspiration of 91.7% and 97.1%, respectively, we were unable to achieve accurate diagnostic results with EUS fine-needle aspiration.
Whereas there have been numerous case reports detailing infections after EUS and endoscopic techniques, the emerging concern for transmission of resistant micro-organisms such as carbapenem-resistant Enterobacteriecae (CRE) and extended spectrum β-lactamase (ESBL)-producing organisms has become a problem worldwide. Common instruments used in clinical medicine have now become the nests of these organisms. Recently, Jorgensen et al. [8] demonstrated an infection with a heat-resistant ESBL Klebsiella pnuemoniae in multiple patients who underwent intubation with a contaminated GlideScope® (Verathon, Seattle, WA).
Recent reports of duodenoscopes contaminated with CRE have heightened the concern of transmission of nosocomial superbugs through endoscopy. The current concern over possible contamination of endoscopic equipment is amplified with this case report. In a recent retrospective review, risk factors contributing to the development of CRE after endoscopic manipulation were active hospital stay, the presence of cholangiocarcinoma, and infected duodenoscopes [9]. In our case, our patient did not have any of these characteristics because her endoscopic procedure was performed as an outpatient and she had no history of cancer. However, her history of hepatitis C does raise a question of whether her retroperitoneal cyst was infected with C. glabrata prior to instrumentation with endoscopy. However, she had no symptoms to suggest infection or pain related to her cyst, and after having histopathologic evidence of C. glabrata, the previous cytology specimen was negative for fungal stains. We believe that manipulation with either an infected endoscope or seeding from the gut after manipulation led to the introduction of C. glabrata into the adrenal cyst.
In conclusion, this case represents part of the growing concern of innately resistant organisms slowly inching ahead of the medical community. Although our patient did not have any complications from her adrenalitis, this case demonstrates the possibility of seeding any micro-organisms from procedure-based biopsies. The use of endoscopic equipment—while continuing to gain favor in gastroenterology and surgery—may act as a portal for resistant micro-organisms.
Footnotes
Author Disclosure Statement
No competing financial interests exist.