
Abstract
Abstract
Background:
De Garengeot hernias are defined by the presence of the vermiform appendix within a femoral hernia. The incidence of such hernias is low and their pre-operative diagnosis is challenging.
Case Presentation:
An 85-year-old Caucasian female presented to the hospital with three-day history of tender and erythematous inguinal mass. A computed tomography (CT) scan of the area showed a hernia sac containing a tubular structure resembling the appendix. The patient was taken to the operating room for exploration of the inguinal mass with the goal of managing the hernia and its contents. At surgery, the diagnosis of a De Garengeot hernia was made. Here we discuss the diagnostic and surgical approaches to treating this patient.
Conclusion:
The majority of De Garengeot hernias present in the context of incarcerated femoral hernia. The pre-operative diagnosis of this type of hernia is challenging and CT imaging is the most effective modality to make the diagnosis.
A De Garengeot hernia is defined by the presence of a vermiform appendix within a femoral hernia sac. This type of hernia was first described by the Parisian surgeon Rene Jacques Croissant De Garengeot in 1731, five years prior to the first reported appendectomy [1]. The incidence of De Garengeot hernias is low. Less than 1% of femoral hernias contain the appendix and even a smaller fraction (less than 0.5%) contain an actively inflamed appendix [2]. There have been fewer than 70 cases of De Garengeot hernias reported in the past 20 years. De Garengeot hernias must be distinguished from the more commonly encountered Amyand hernias, which are defined by the presence of an appendix within an inguinal hernia [2,3]. The rate of incarceration is greater in femoral compared with inguinal hernias. This has been attributed to the anatomy of the femoral canal, which forms a narrow and rigid ring around the herniated organs, increasing the likelihood of incarceration and strangulation [2,3].
Because of the paucity of reports on surgical management of De Garengeot hernias, no standard management guidelines have been developed. Here we describe a case of De Garengeot hernia and our surgical approach to treating the patient.
Case Presentation
An 85-year-old Caucasian female presented to the emergency department with a three-day history of right inguinal mass. Upon presentation the patient was hemodynamically stable with a blood pressure of 135/82 mm Hg, pulse of 89, and temperature of 37.3°C. She denied fever, chills, nausea, or vomiting. She also denied any diarrhea or constipation, blood in the stool, or distention. Upon examination in the emergency department a 2×3 cm mass that was warm and tender to palpation was noted immediately below the inguinal ligament. Attempts to reduce the mass were unsuccessful. The remainder of the abdominal examination was unremarkable and the abdomen was soft, non-tender, and non-distended without rebound or guarding. Normal bowel sounds were present without any abdominal organomegaly. No cervical, inguinal, or axillary lymphadenopathy was detected. Complete blood count and comprehensive metabolic panel were unremarkable without leukocytosis, left shift, or electrolyte imbalances. A computed tomography (CT) scan done in the emergency department showed a right inguinal hernia containing a portion of the appendix. There was also a 2.6×1.8 cm rim-enhancing fluid collection within the hernia sac, with peripheral, non-dependent calcification, and surrounding fat stranding (Fig. 1). This was interpreted as an Amyand hernia with acute appendiceal inflammation and likely perforation. The patient was therefore admitted to the hospital and taken to the operating room.

This image demonstrates an abdominal computed tomography (CT) scan with the femoral hernia sac marked with an arrow. Notice the femoral vein lateral to the hernia sac. A tubular structure containing a calcified mass, likely a fecalith, can be observed within the hernia sac.
An inguinal incision was performed and the external oblique aponeurosis was opened to examine the inguinal canal. The groin mass was determined to be a femoral hernia and the neck of the hernia was widened by dividing the medial inguinal ligament toward the lacunar ligament. The inflamed hernia sac was then digitally reduced and the sac opened. However, the appendix observed on CT scan pre-operatively could not be found. Through the opened sac a loop of small bowel was grasped, and run distally to the cecum, allowing the appendix to be visualized and brought into the sac. The appendix was clearly gangrenous in its distal one-third, but otherwise normal in appearance (Fig. 2). An appendectomy was performed and the femoral hernia repaired using the McVay technique.
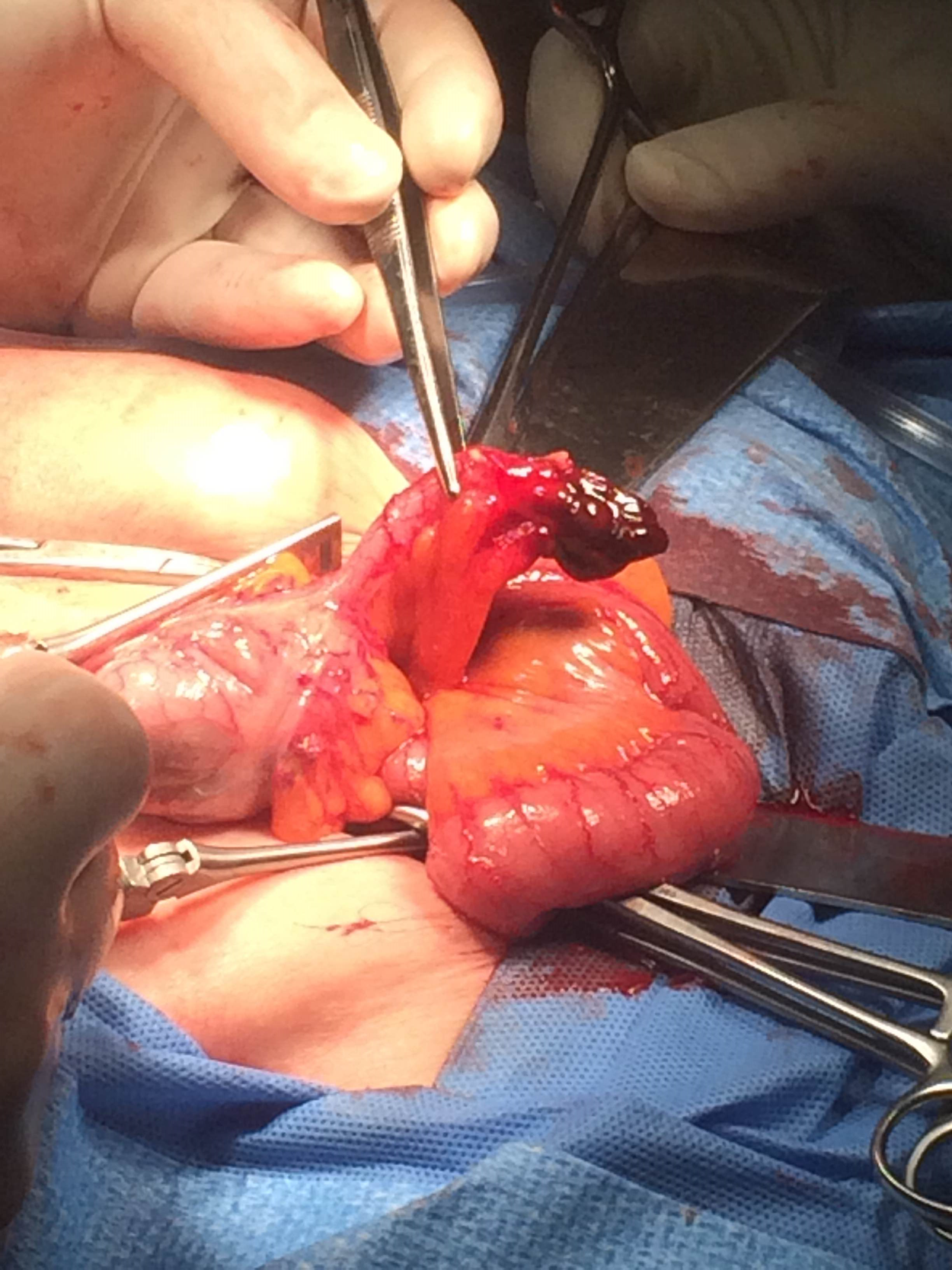
The gangrenous tip of the appendix can be observed in this image obtained during the surgery. The body of the appendix shows no signs of necrosis.
Discussion
A femoral hernia containing the vermiform appendix, eponymously named the De Garengeot hernia, is a rare occurrence with an incidence of less than 1%. A De Garengeot hernia is often an incidental finding at the time of surgery, usually after a provisional diagnosis of strangulated bowel in a femoral hernia. The majority of femoral hernias contain omentum, small bowel, colon, or ovaries. Femoral hernias form more commonly in females but are less common than inguinal hernias in both genders and only constitute 4% of all groin hernias [3].
Physical examination findings are important in diagnosing an incarcerated hernia, but play a minimal role in the specific diagnosis of De Garengeot hernias. Erythema over the hernia site is a common finding in De Garengeot hernias but it is not specific to them. Ultrasound and CT imaging have proved valuable in diagnosing De Garengeot hernias, however, the rate of misdiagnosis remains high [4–6]. In our case the pre-operative diagnosis was that of an Amyand hernia, which occurs more commonly and is better known to surgeons and radiologists than De Garengeot hernias. Typical CT scan findings associated with De Garengeot hernias include a hernia medial to the femoral vein containing a tubular structure and a low-positioned cecum [5,7].
The pathogenesis of De Garengeot hernias is not well understood. It has been suggested that abnormal intestinal rotation during embryogenesis leading to an atypical appendicocecal attachment can increase the likelihood of appendiceal herniation through the femoral canal. Furthermore, an abnormally enlarged cecum extending into the pelvis can further displace the appendix into the canal [8]. Similarly the pathophysiology of De Garengeot appendicitis is controversial. It has been suggested that appendiceal inflammation starts within the peritoneum and then the inflamed appendix gradually descends into the femoral canal. Others suggest that the appendix migrates initially into the hernia sac and the rigid femoral neck subsequently strangulates the appendix causing appendicitis [8].
The narrow opening of the femoral hernia sac into the peritoneal cavity is believed to contain the inflammation within the sac, preventing the spread of inflammation into the rest of the peritoneal cavity and development of peritoneal signs [8]. In our case, the patient had a gangrenous appendix but no peritoneal signs. This can complicate the management of these patients further as the development of peritonitis as a sign of appendix perforation and abscess formation in intra-abdominal appendicitis changes the surgical approach to treating the patient.
No standard surgical approach has been established to treat De Garengeot hernias. The approach should be based the anatomic and clinical findings during the surgery, particularly the presence or absence of appendicitis, and should take into account the patient's clinical status including comorbidities. In presentations such the one reported here, patients are treated with inguinal exploration with appendectomy and femoral herniorrhaphy once the diagnosis is confirmed. The use of mesh in cases in which a perforation/gangrene of appendix is present has potential to increase the likelihood of post-operative infection and is therefore not recommended. Some authors have suggested that an appendectomy is only necessary if appendicitis is present. Simple laparoscopic reduction of the normal appendix with hernia mesh repair might be appropriate [9].
Conclusion
De Garengeot hernia is a rare, yet serious medical condition. Most cases of De Garengeot hernia are found incidentally during femoral herniorrhaphy operations. Although the majority of De Garengeot hernias contain an un-inflamed appendix, appendicitis with perforation/gangrene may complicate these cases [2]. The tight ligaments at the neck of the femoral canal can contain inflammation and prevent the formation of intra-abdominal abscess or peritonitis [8]. In the setting of an acute inguinal mass, prompt surgical repair is recommended upon finding De Garengeot hernia on CT or ultrasound imaging.
Footnotes
Author Disclosure Statement
No competing financial interests exist.