
Abstract
Abstract
Background:
Abdominal hernia repair with polypropylene mesh is common because of the decreased risk of recurrence. The major risk after surgery is mesh infection, which is associated significant morbidity.
Case Presentation:
We report a case of delayed mesh infection secondary to a suture granuloma that presented 11 years after umbilical hernia repair.
Conclusion:
When performing hernia repairs it is important to remember that when complications do occur that the presence of foreign material such as mesh has the potential for increased morbidity, potentially even decades after the repair.
In the United States there are more than 350,000 ventral hernias repaired annually [1]. Repair with polypropylene mesh has become the standard because of decreased rates of recurrence and post-operative pain, however, this comes at the increased risk of seroma formation and surgical site infection [2]. Surgical site infection involving mesh can be early or delayed and have devastating consequences, frequently requiring mesh explantation [3]. The patient presented developed an infected mesh 11 years after umbilical hernia repair for symptomatic incarcerated umbilical hernia.
Case Presentation
A 57-year-old male presented to the surgical clinic reporting two weeks of worsening erythema and pain around his umbilicus. At presentation he denied fever or other constitutional symptoms but did admit to serous drainage from the area. Eleven years previously the patient had had an open umbilical hernia mesh repair for an acutely incarcerated hernia containing peritoneal fat. The hernia was repaired with a polypropylene and polytetrafluoroethylene mesh secured with polypropylene suture. He received 1 g of cefazolin intravenously pre-operatively and was re-dosed post-operatively. There was no evidence of surgical site infection at his post-operative clinic appointment.
The patient had a past medical history significant for type 2 diabetes mellitus controlled by oral therapy and hyperlipidemia. The umbilical hernia repair was his only other abdominal surgery. There was no history of tobacco abuse or immunosuppressive medications and/or disease. On examination, the patient was found to be afebrile with a regular heart rate and in no acute distress. His abdomen had a 3×3 cm circumferential area of erythema and induration that was tender and warm to the touch. At the most inferior aspect of his umbilicus there was a pinhole epidermal defect from which seropurulent fluid drained, which was sent for culture. Upon probing the area a polypropylene suture could be identified in the subcutaneous tissue. The patient was begun initially on amoxicillin-sulbactam, until the fluid culture grew methicillin-resistant Staphylococcus aureus (MRSA) at which time he was switched to vancomycin for the peri-operative period. The patient was then scheduled for surgery for mesh excision promptly after computed tomography (CT) results were obtained. A CT scan with oral and intravenous contrast revealed an ill-defined anterior abdominal wall collection at the level of the umbilicus measuring 2.6×3.1 cm with nearby fat stranding consistent with abscess (Fig. 1).
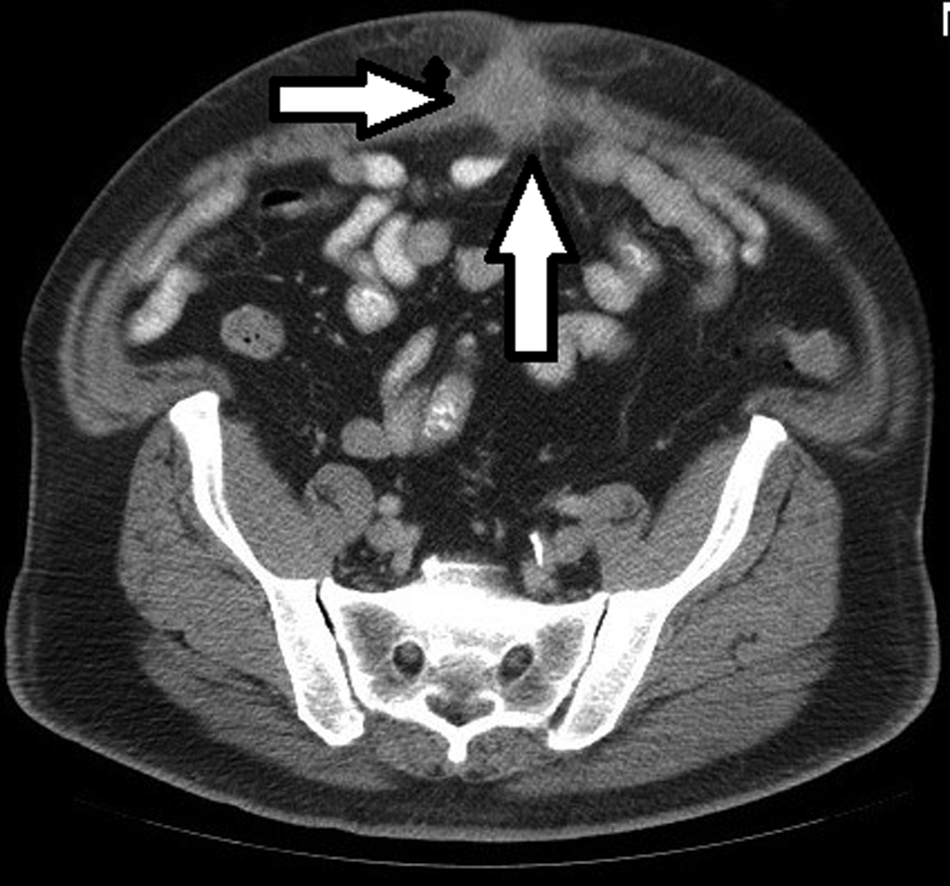
Computed tomography demonstrates abscess involving ventral wall mesh (arrows).
The patient underwent open surgery with excision of the mesh. There was a severe fibrotic reaction around the mesh and purulence. The fluid was drained and re-cultured. A suture granuloma and sinus was observed connecting the skin to the mesh. The mesh was densely incorporated into the fascia but was removed in its entirety. Because a bowel injury from the extensive dissection of the mesh could not be ruled out, a second low mid-line laparotomy incision was made to run the small bowel along its length. There was no damage to the intra-abdominal contents. The abdominal cavity and infra-umbilical incision was irrigated copiously with sterile saline. The hernia defect was closed with figure-of-eight #1 polydioxanone (PDS) sutures, and a one-fourth–inch Penrose drain placed to the subcutaneous tissue with skin loosely closed with staples. The laparotomy was closed separately with running looped #0 PDS and the skin was stapled closed.
Post-operatively the patient did well. He was discharged and the drain was removed on post-operative day two without leukocytosis or fever. Operative cultures confirmed MRSA. The patient was maintained on intravenous vancomycin throughout his hospital stay and was discharged on oral clindamycin 300 mg four times per day for a total course of seven days. He was observed in the clinic one week later without symptoms and cellulitis had resolved.
Discussion
Repair of umbilical hernias using mesh is performed by some surgeons because of the decrease in rate of hernia recurrence with similar short-term complications (such as seroma, hematoma, and incision infection). One randomized control trial demonstrated an 11% chance of recurrence with tissue repair and only a 1% recurrence with a tension-free mesh repair, whereas other reports demonstrate near-identical risk of recurrence [3,4]. Larger hernias with a defect larger than 2 cm in size are associated with a greater risk of recurrence in tissue repair [4].
Tempering many surgeons' preference for mesh implantation during umbilical herniorrhaphy is the potentially severe morbidity associated with infection of the implanted mesh. These complications include re-operation, explantation of mesh, re-infection of the subsequent repair, and recurrent hernia [5,6]. Indeed, risk of a surgical complication unrelated to hernia recurrence in tissue repair is less than that of mesh hernia repair [4].
Delayed surgical site infections can be caused by a number of factors. It is possible that the combination of synthetic mesh and non-absorbable suture caused a violation of the overlying epidermis leading to a retrograde infection (from the skin to the mesh) or contamination of the mesh at the time of surgery 11 years prior evolved slowly because of local immune dysfunction is merely conjecture. Delayed surgical site infections such as this have been studied and analyzed. In a university-based retrospective study, 46% of patients undergoing any surgical procedure with surgical site infections occurring more than six months after the index operation were associated with suture abscesses. Of these cases, 75% of the cultures grew Staphylococcus aureus [7].
Conclusion
The risk of a delayed infection after placement of a foreign body contains a small but ongoing risk of infection even years after surgery.
Footnotes
Author Disclosure Statement
No competing financial interests exist.