
Abstract
Abstract
Background:
Enterobius vermicularis infection is one of the most common causes of parasitic infection of the gastrointestinal tract, affecting almost 30% of the pediatric population worldwide.
Conclusion:
Although it is unclear whether E. vermicularis mimics acute appendicitis by occluding the lumen of the appendix, we present a case of acute appendicitis in a patient with clinical and radiologic signs of appendicitis confirmed by microscopic acute inflammatory changes of the appendix and the presence of an intra-peritoneal granuloma.
Enterobius vermicularis infection is one of the most common parasitic infections in the gastrointestinal tract with an incidence of 4%–28% in the pediatric population [1]. Enterobius vermicularis is a parasite that lives exclusively in human beings and has been associated with surgical pathologies and infections such as colitis, peri-anal abscesses, intra-abdominal granulomas, pelvic inflammatory disease, and appendicitis [2]. Its presence on the lumen of the appendix can cause obstruction and simulate signs and symptoms of appendicitis in 0.2%–41.8% [1]. Some series indicate that it does not cause appendicitis [3]. Intra-abdominal granuloma secondary to E. vermicularis has been reported once in a 32-year-old female at the fallopian tubes [4]. Here, we present a 12-year-old female with eosinophilic acute appendicitis and intra-abdominal granuloma caused by E. vermicularis with histopathologic confirmation.
Case Report
A 12-year-old female presented to the emergency department with a three-day history of abdominal pain that started at the epigastrium and migrated to the right lower quadrant; the pain was associated with anorexia and nausea. The patient received three doses of azithromycin from her primary care physician before presenting at the emergency department. Physical examination revealed McBurney and Rovsing positive signs.
Complete blood count (CBC) showed the presence of eosinophilia without elevated white blood cell count. An abdominal ultrasound showed the presence of a tubular structure 10 mm in diameter confirming appendicitis (Fig. 1).

Transverse ultrasound of the right lower quadrant with a non-compressible 10-mm tubular structure compatible with appendicitis.
The patient underwent a laparoscopic appendectomy. The appendix was identified as edematous and an inflammatory process was found incidentally adhered to the anterior abdominal wall.
The laparoscopic appendectomy was completed using endoloops, and immediately after the incision of the base of the appendix with laparoscopic scissors the presence of E. vermicularis (pinworms) was observed; these were removed surgically with suction (Fig. 2). The appendix was then removed through the umbilical port.

(
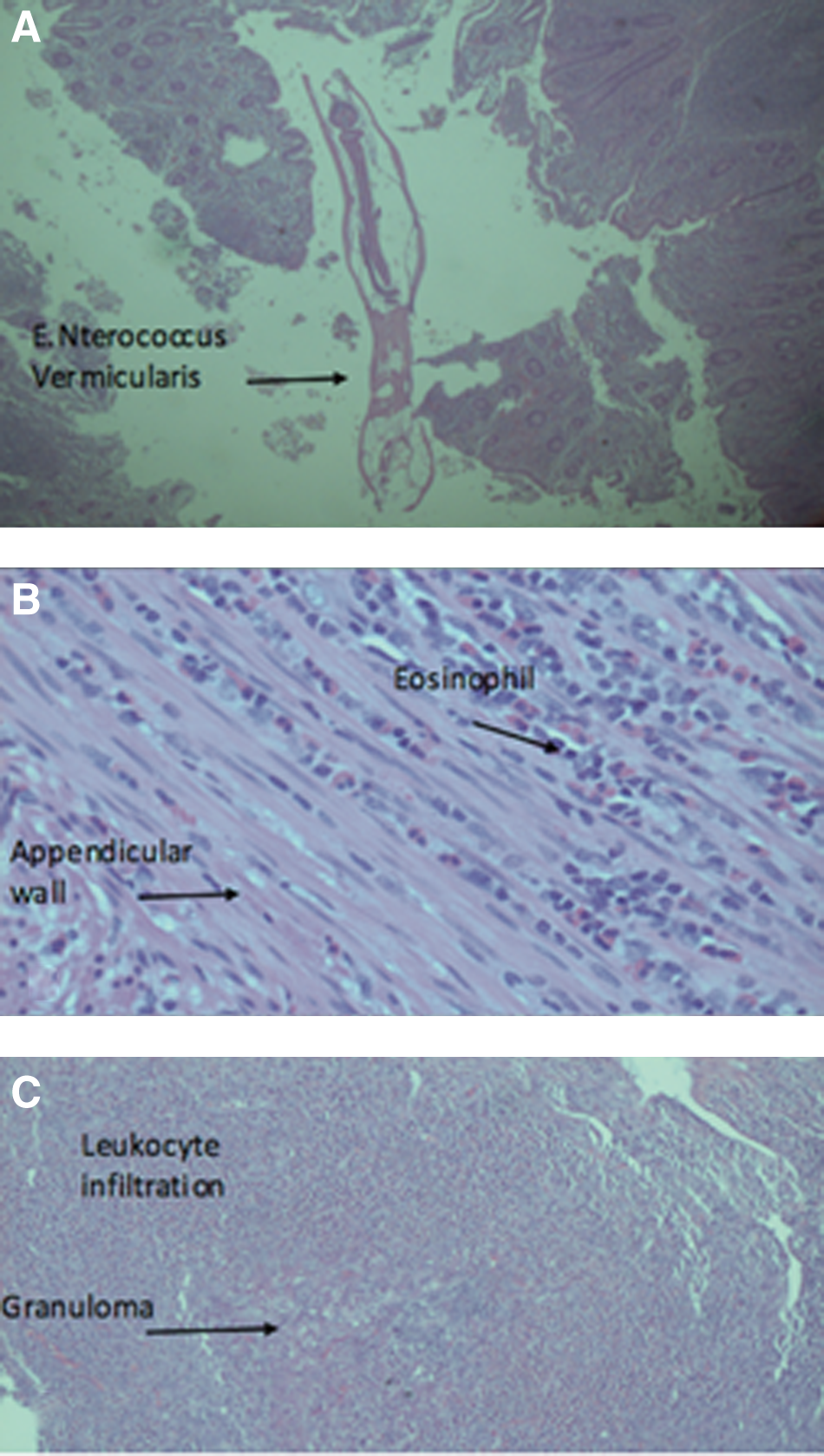
Pathology confirmed the presence of appendicitis with eosinophils and the presence of nematodes Oxyuroidae (E. vermicularis); the abdominal wall lesion with abscess, eosinophils and granulomatous tissue was caused by Oxyuroidae (Fig. 3). The patient was discharged with anti-parasitic medication, which was also provided for all close relatives.
(
Discussion
Appendicitis and E. vermicularis are common in the pediatric population and have been associated since the first description in 1970 [5]. Appendicitis and E. vermicularis can coexist without presenting any clinical signs or symptoms and have been described as incidental findings at microscope evaluation, as well as other parasites such as Ascaris and Trichuris trichiura [6–8] even in the adult population [9].
The episodic symptoms can be caused by intestinal infestation of E. vermicularis that temporarily occlude the lumen of the appendix and simulate appendicitis [10]. In some series this has been described as chronic appendicitis [1] with an elevated count of eosinophils without elevation of the expected white blood cell count [1,10], and can even present as an acute abdomen [11].
The spectrum of appendicitis can be infectious or not, and it is important to identify which one can be caused by parasites, with special attention to those who have episodic symptoms at presentation, without elevation of the white blood cell count, and can benefit of fecal analysis or even from an antiparasitic empiric treatment [10,12,13]. The patient did have antibiotic treatment with azithromycin starting three days before her arrival at the emergency department. Although not the first-line treatment for appendicitis, azithromycin has coverage for gram negative bacteria Enterobacteriaceae [14], which might explain the unresponsiveness to the treatment in this patient. The presence of eosinophilic intra-abdominal granuloma secondary to pinworms is rare [15,16], but it has had been associated with the histologic presence of E. vermicularis in the appendix [4,7].
The laparoscopic surgical approach has the advantage of identifying the presence of the intra-abdominal granuloma that can be associated with appendicitis secondary to parasites. It can also identify those parasites that can be free inside in the peritoneal cavity at the time of the base cut of the appendix and remove them from the abdomen [17].
Conclusion
Acute appendicitis can be caused by parasites. Patients who have episodic symptoms of appendicitis and elevation of eosinophils should increase the suspicion of having E. vermicularis and a fecal analysis might be warranted. Treatment should be surgical in positive physical and radiologic signs of appendicitis, and anti-parasitic medication must be started for the patient and all close relatives. The use of antibiotics might not be needed in acute eosinophilic appendicitis caused by parasites.
Footnotes
Author Disclosure Statement
No competing financial interests exist.