
Abstract
Abstract
Background:
Cytomegalovirus (CMV) causes the most common post-transplant systemic viral infection. During infectious epidemics, such as the outbreak of novel influenza A (H1N1), immunocompromised hosts including transplant recipients may be at greater risk for acquiring disease and may have a more serious course.
Case Report:
We report on a 65-year-old female renal transplant recipient who underwent pre-transplant desensitization with whole plasma exchange, intravenous immunoglobulin (IVIG), and rituximab and developed simultaneous CMV disease and H1N1 pneumonia. With accurate diagnosis (CMV polymerase chain reaction [PCR] and H1N1 isolation from bronchoalveolar lavage), ganciclovir, oseltamivir and IVIG therapy, and temporary withdrawal of immunosuppression, the patient recovered from the life-threatening infection with preservation of graft function.
Discussion:
Co-infection with multiple pathogens should always be considered in transplant recipients receiving intensified immunosuppression, especially during outbreaks of large epidemics.
In 2009 novel influenza A (H1N1) virus spread throughout the world causing a pandemic [1]. Although this disease has been found to be no more severe than seasonal influenza in the general population [2], certain populations including children [3], pregnant women [4], and immunocompromised individuals such as solid organ recipients [5] were found to be at greater risk for severe illness caused by novel H1N1 influenza [6]. Because H1N1 has emerged as a major complication in transplant recipients, the Transplant Infectious Diseases Section of The Transplantation Society and the American Society of Transplantation Infectious Diseases Community of Practice published guidelines for prevention and management of this disease [6]. This publication also serves as a guide for potential future epidemics by other pathogens. Outbreaks with primary pathogens such as seasonal influenza add a significant challenge to the already complex issue of infections in renal transplant (RT) recipients [7]. The intensity of immunosuppression has increased during the past decade, which has facilitated renal transplantation in individuals who have high concentrations of panel reactive antibodies (PRA). These protocols include intravenous immunoglobulin (IVIG), whole plasma exchange (WPE), and the anti-CD20 antibody rituximab, which blocks antibody production for an extended period of time. Because RT recipients also receive powerful anti-T-cell agents, patients who undergo such desensitization protocols at high risk for infection. Among opportunistic pathogens, cytomegalovirus (CMV) is the most common virus causing systemic disease in RT recipients [8] and exhibits direct and indirect effects in transplant recipients and their allografts [9–12]. These effects increase graft rejection and chronic dysfunction and are predisposing to other infections including influenza [13]. An increasing number of reports describe late onset CMV disease after ganciclovir (GCV) prophylaxis has been stopped, with up to 50% of high-risk patients (mainly CMV-seronegative recipients of CMV-positive allografts) developing this complication [12,14].
Case Report
A 65-year-old female developed end-stage renal failure because of diabetic nephropathy. She was found to have high concentrations of PRA and underwent desensitization using WPE, IVIG, and rituximab. She was started on mycophenolate mofetil (MMF; 2 g daily) and had a splenectomy. Cadaveric RT was performed without difficulty; cold ischemia was 30 h and 50 min. Immunosuppression included antithymocyte globulin (1.5 mg/kg on three consecutive days), continued MMF, tacrolimus (TAC) with trough concentrations of 8–12 ng/mL, and a steroid taper. Donor and recipient tested positive for anti-Epstein-Barr virus (EBV) and anti-CMV antibodies. Infectious prophylaxis included trimethoprim-sulfamethoxazole (80/400 mg) twice weekly and GCV intravenously at a dose of 5 mg/kg followed by oral valganciclovir (valGCV) at a dose of 900 mg daily adjusted to the renal function. New-onset atrial fibrillation was managed with amiodarone. She was discharged after 14 d with delayed graft function and a serum creatinine of 3.8 mg/dL on hemodialysis. She was re-admitted a week later with persistent graft dysfunction. Renal biopsy showed significant arteriosclerosis with moderate interstitial fibrosis. A 99mTc-mercaptoacetyl-triglycine (MAG3) renal scan demonstrated markedly delayed and decreased perfusion of the renal allograft, with the nephrogram showing a non-uniform band-like distribution; no parenchymal clearance was identified. Magnetic resonance imaging/magnetic resonance angiogram (MRI/MRA) showed non-anastomotic 50%–60% vascular stenosis between the transplant renal artery and the native external iliac artery. Renal arteriogram with successful percutaneous transluminal angioplasty (PTA) of the graft artery was performed 4 wks after RT and she was started on coumadin; her creatinine decreased to 2.2 mg/dL.
Seven weeks post-RT, the patient developed malaise, watery diarrhea, a non-productive cough, and a fever (temperature, 39°C). She had not received H1N1 influenza vaccination because of vaccine unavailability but reported no known exposure to influenza. Her last dose of valGCV prophylaxis was a week earlier. She was admitted to an outside hospital where a chest radiograph showed multi-focal pneumonia and ceftriaxone was started. It was advised to start empiric oseltamivir (75 mg twice daily) and to temporarily stop MMF and TAC. A rapid flu test was negative. She was transferred to our hospital the next day and repeat chest radiograph revealed left lower lobe infiltrate and interstitial edema (Fig. 1). Chest CT scan showed bilateral patchy lung opacities consistent with multi-focal pneumonia (Fig. 2). Laboratory values revealed acute kidney injury with a creatinine of 2.9 mg/dL and a white blood cell (WBC) count of 4,700/mm3, a C-reactive protein of 10.4 mg/dL; TAC trough concentration was 4.5 ng/mL. Vancomyin, piperacillin-tazobactam, and metronidazole were started emperically; immunosuppression was held. Rapid influenza antigen testing and reverse transcription-polymerase chain reaction (RT-PCR) of nasopharygeal swabs (the latter performed twice) remained negative as were sputum culture and urinary Legionella antigen. Blood PCR revealed a CMV viral load of 21,000 copies per milliliter and EBV viral load was 1,000 copies per milliliter. It was assumed that pneumonia was caused by CMV, and therefore, oseltamivir was not continued and intravenous GCV (10 mg/kg per day adjusted to the renal function) was started. Diarrhea persisted and stool tested negative for acid fast bacilli, Campylobacter jejuni, Cryptosporidium spp, and Clostridium difficile toxin; metronidazole was stopped. With worsening non-productive cough, persistent fever, and increasing oxygen requirements, bronchoscopy with bronchoalveolar lavage (BAL) was performed on hospital day three, which grew influenza A virus. Stains for Pneumocystis carinii pneumonia (PCP) and Legionella and cultures for bacteria, mycobacteria, and fungi were unrevealing. A biopsy could not be done because of the severe coagulopathy (international normalized ratio [INR] of 3.8 because of coumadin therapy). She was transferred to the intensive care unit (ICU) for further monitoring in view of progressively worsening respiratory status and started on continuous positive airway pressure. Oral oseltamivir was given at a dose of 75 mg twice daily with significant clinical improvement within 72 h allowing transfer to the floor. Her creatinine remained stable at 2.5 mg/dL. Cytomegalovirus viral load decreased within two weeks to less than 600 copies per milliliter and she was discharged in good condition. At 12 wks after RT she was doing well with complete resolution of her respiratory illness, her creatinine decreased to 2.1 mg/dL. Cytomegalovirus PCR was negative, there were no signs of ongoing CMV disease, and she completed three months of valGCV. Immunosuppression had been increased gradually to a maintenance regimen including MMF (500 mg twice daily), TAC with trough concentrations of 4–8 ng/dL, and prednisone 10 mg daily. At her six-month evaluation she was free from rejection and infection with a serum creatinine of 2.3 mg/dL. She had good long-term graft function.

Chest radiograph shows widespread patchy airspace disease.
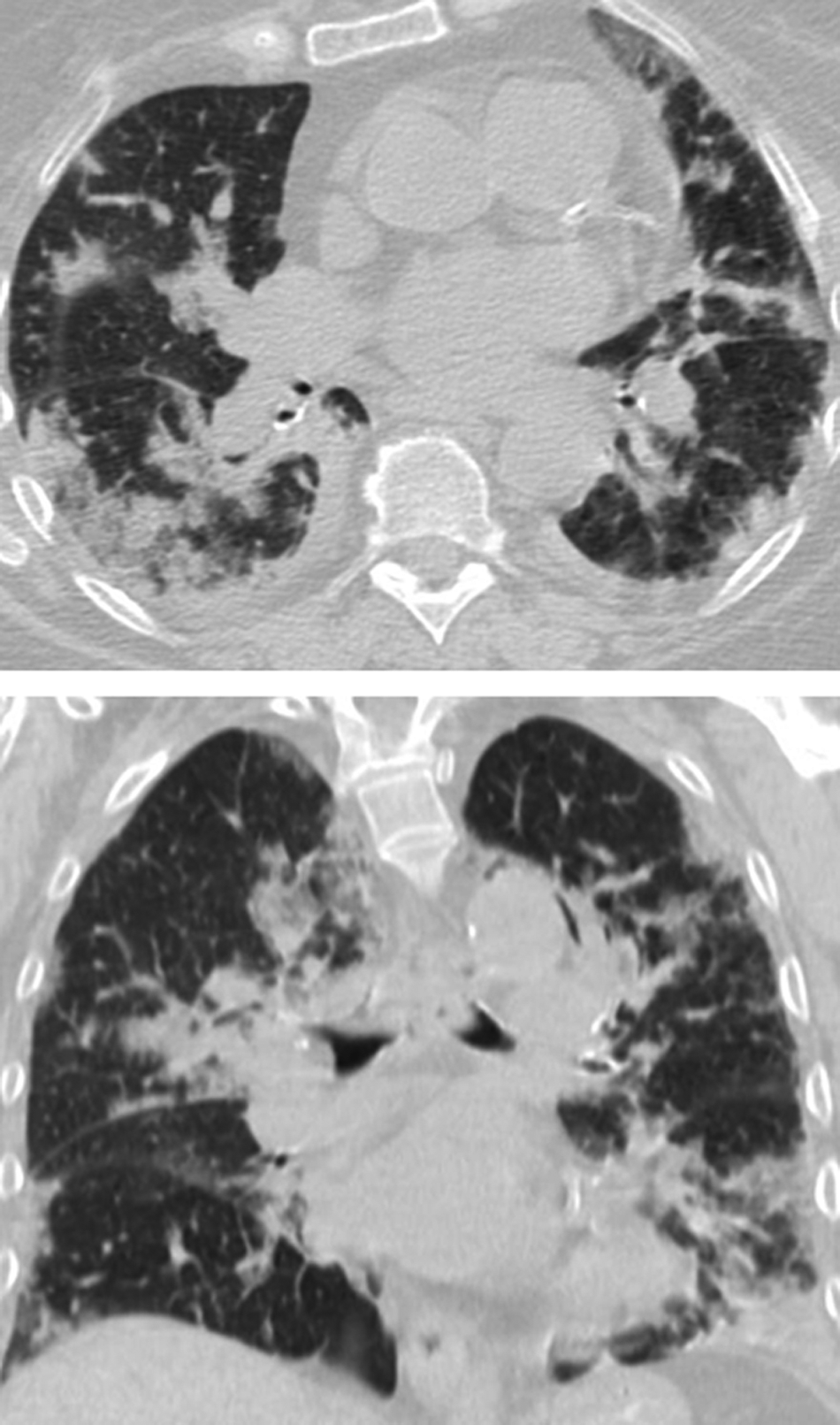
Axial and coronal reformatted images of chest computed tomography (CT) show bilateral patchy multifocal areas of consolidation both in central and peripheral location with slight lower lobe predominance.
Discussion
Our case illustrates that transplant recipients may develop multiple infections simultaneously. Even during pandemics such as H1N1 influenza, it is crucial to exclude other concurrent infections, particularly those known to be common in this patient population [15]. Our patient had received intense immunosuppression putting her at heightened risk to develop opportunistic infections. If untreated at an early stage, these infections have the potential to become life threatening. Once the patient had contacted us reporting symptoms compatible with influenza, she was immediately advised to reduce immunosuppression, be evaluated clinically, start emperic oseltamivir, and be tested for influenza virus. As the causative pathogen was unknown early in her course and with the history of recent exposure to rituximab with an admit immunoglogulin G concentration of 820 mg/dL and immunoglobulin M of 55.6 mg/dL, IVIG was added to our anti-infective therapy. Three influenza assays were performed and all were negative, however, at the same time CMV PCR was positive. Oseltamivir was held and GCV started assuming that this patient had CMV disease with pneumonitis and enteritis. However, as her clinical status worsened and CT scan showed interstitial pneumonia, we performed BAL. A CT scan cannot distinguish between pneumonia caused by H1N1 and by CMV [16–19], however, BAL revealed the correct diagnosis of H1N1. Oseltamivir was restarted, which led to clinical improvement within 24 h. Of note, influenza tests from nasopharygeal specimens had returned negative repeatedly, emphasizing that a low threshold to perform BAL in these patients is indicated. A lung biopsy could not be performed because of the severe coagulopathy. Only a biopsy could have definitively distinguished between pneumonia caused by CMV and H1N1. Therefore, we cannot determine clearly the contribution of each viral pathogen to the patient's respiratory illness.
To summarize, we present a highly immunosuppressed RT recipient who developed simultaneous infection with H1N1 and CMV presenting with pneumonia. As a result of timely oseltamivir and GCV therapy, along with judiciously reduced immunosuppression, IVIG, and supportive care, the patient was treated successfully and had preservation of graft function.
Footnotes
Author Disclosure Statement
No competing financial interests exist.