
Abstract
Triplication of the ureter is a rare urologic finding that has been well described in the literature. Patients can present with urinary tract infections, incontinence, and calculi. We present the case of a patient with extensive stone burden with right trifid and left bifid collecting systems. Stone management was performed with a multimodal approach using a combination of endoscopic and percutaneous approaches. Our systematic and staged approach highlights a method for efficacious stone treatment in a complex endourologic case.
Introduction
Ureteral triplication is a rare congenital phenomenon that has been associated with >100 cases since it was first reported by Wrany in 1870 and classified by Smith in 1946. Smith classified ureteral triplication into four types as follows: Type I—complete ureteral triplication with three ureteral orifices (35%), Type II—incomplete triplication with three ureters and two ureteral orifices (21%), Type III—trifid ureters with ureters draining into one orifice (31%), and Type 4—with two ureters from the kidney and one bifurcated leading to three draining orifices (9%). 1 The patient may present with unilateral or bilateral triplication, and those with unilateral triplication can have contralateral complete duplication, partial duplication, and even quadruplication. Patients can be asymptomatic (8%) or present with urinary tract infections, urinary incontinence, or renal colic. 2
Here we present a case of right-sided complete triplication and left-sided duplication to the level of the ureteral orifice. A multimodality approach was used on this patient's bilateral stone burden.
Case Report
We present a case of complex stone management in a patient with multiple ureteral anomalies. He is a 50-year-old male with a medical history of diabetes mellitus and hypertension and no history of nephrolithiasis who presented to our clinic with gross hematuria. A CT urogram was performed that revealed a completely trifid collecting system on the right side and a bifid system on the left side (Fig. 1). The patient denied a history of any congenital abnormalities and none were evident on physical examination. His stone burden was as follows: right upper pole (3.0 cm calculus), right lower pole (1.6 cm and 6 mm calculi), and left lower pole (1 cm, 1.5 cm, and 8 mm calculi). Preoperative urine cultures were negative.
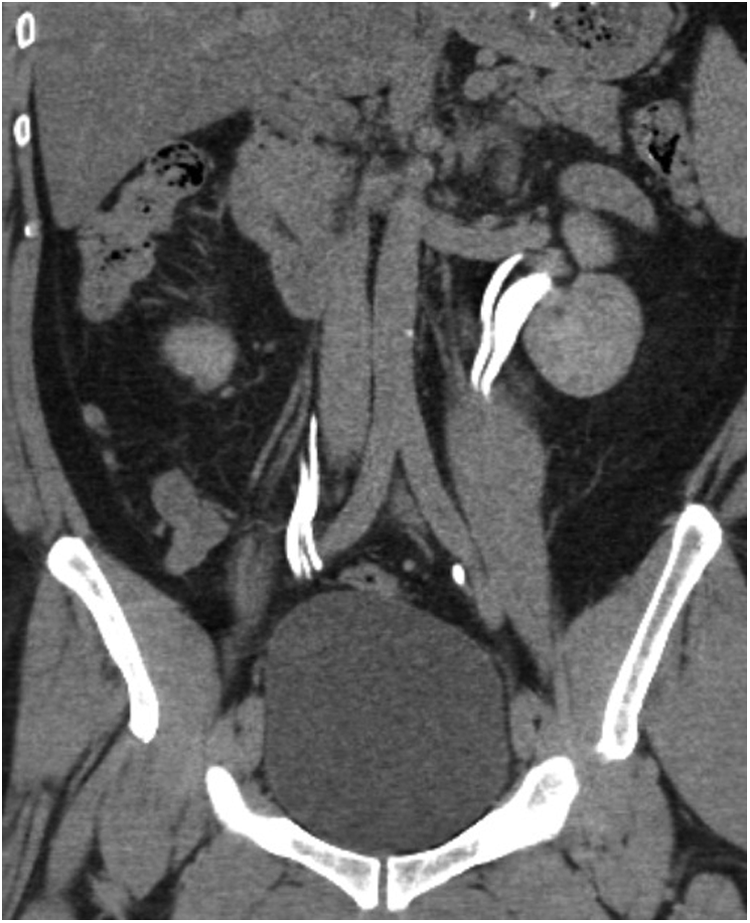
CT urogram delayed phase showing right trifid and left bifid collecting systems.
Given the complex anatomy and high stone burden, ureteroscopy was initially employed to treat the small stone burden on the left and also to investigate the collecting systems bilaterally with retrograde pyelograms. Upon inspection, with cystoscopy, three separate ureteral orifices (Fig. 2) were seen on the right side. Performing retrograde pyelograms outlined the right side as follows: the most superior and lateral orifice led to interpolar moiety (A), the second orifice slightly distal and medial led to the upper pole moiety (B), and lastly, the most distal and lateral orifice led to the lower pole moiety (C). The right trifid collecting system is well appreciated on retrograde pyelograms (Fig. 3). The left side of the bladder had only one ureteral orifice and ureteroscopic examination revealed a bifid system that joined to a common intramural tunnel. Using a flexible ureteroscope and 200-μm laser fiber, laser lithotripsy was able to fragment the left lower pole stones to small 1–2 mm passable fragments and the patient was left with a stent. The right upper pole moiety was stented with a 6F × 24 cm Double-J stent to help dilate the ureter and provide access for percutaneous nephrolithotomy (PCNL).
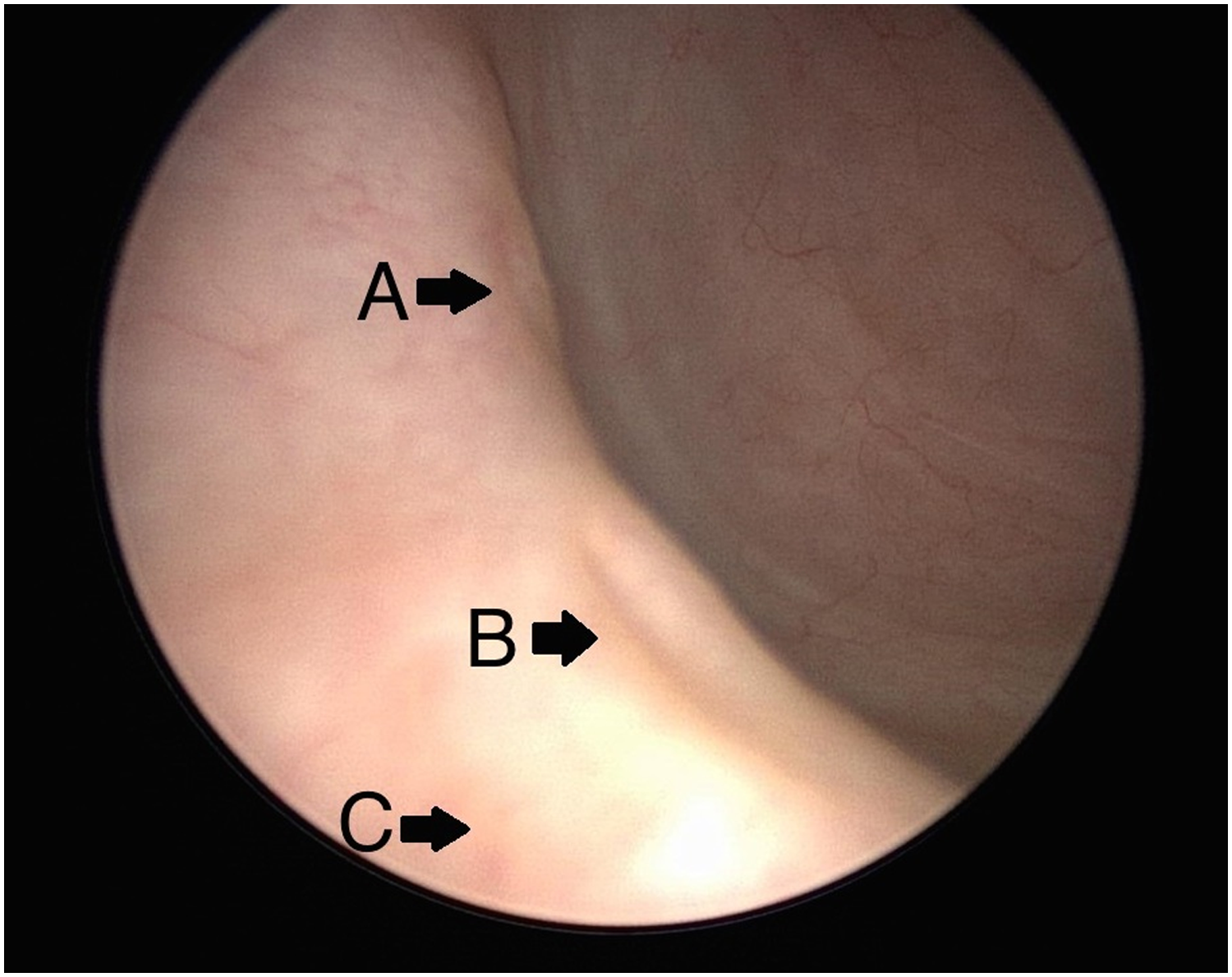
Three ureteral orifices seen during cystoscopy on the right side. Arrow A, interpolar moiety; arrow B, upper pole moiety; arrow C, lower pole moiety.

Retrograde pyelogram showing trifid right-sided collecting system (Type I).
Next, 2 weeks later, a right PCNL was performed. Supracostal access was utilized because of a separate upper pole system and performed with deep inspiration using triangulation and the bulls eye technique with 0° and 30° angles. A 26F nephroscope was used after access and the ultrasonic lithotripter was used to fragment and suction the entire stone burden. Once all visible stone burden was removed, we placed a 24F Malecot re-entry tube. No pleural injury was noted during the postoperative period.
Finally, a third procedure was performed to evaluate bilateral collecting systems and treat the remaining right lower pole stone burden using a flexible ureteroscope and 200-μm laser fiber. A right nephrostogram showed no residual fragments or extravasation and the Malecot re-entry tube was removed. At the termination of our third procedure, the patient was left without any nephrostomy tubes or ureteral stents and was cleared of all stone burden. Postoperative follow-up 1 week after the final procedure revealed that the patient was comfortable, in no distress and without pain, had no evidence of fevers or infection, and was voiding comfortably. Stone analysis revealed a composition of 100% calcium oxalate monohydrate.
Discussion
Ureter development can begin as early as the fourth week of gestation. The ureteral bud arises from an outpouching of the Wolffian or mesonephric duct and invades the metanephric mesenchyme. The ureteral bud divides and branches to form the renal collecting system from the ureteral orifice to the collecting system of the kidney. 3 In triplication of the ureter, three ureteral buds could arise independently from the mesonephric duct or from early fission of one or more ureteral buds to join the metanephros. In this case, we presented a patient with Type I ureteral triplication on the right side based off the Smith classification system and a bifid system on the left side for a total of five ureters.
Given the complex nature of the stone burden and rare anatomy, we proceeded in a systematic and step-wise manner to treat the patient's stone burden. Our multimodal approach utilized ureteroscopic and percutaneous stone techniques in a staged manner. Given the ureteral anomalies that were demonstrated on preoperative CT urogram, we decided to start ureteroscopically to allow us to better understand the anatomy and perform retrograde pyelography. We were able to perform ureteroscopy and laser lithotripsy in a single setting to clear the majority of the stones on the left side in one setting while at the same time also placing a stent in the right upper pole moiety.
Once we had cleared the stone burden on the left side, the next staged procedure was PCNL, which effectively cleared the 3 cm right upper pole moiety. The supracostal access did create concern for increased risk of pleural injury; however, this risk ranges between 1.6% and 2.2% and can offer excellent stone clearance rates. 4 Our final staged procedure involved bilateral ureteroscopy to assess clearance of stone burden after prior procedures and treat the residual lower pole calculi seen on imaging. Ureteroscopy of the right upper pole moiety demonstrated excellent stone clearance with PCNL as there was no residual burden seen. Given the position and that relocalization of the stones to a more favorable calyx could not be performed in a trifid system, our approach highlights the importance of a “second-look” in a setting with extensive overall and lower pole stone burden. Our combination of PCNL and ureteroscopy allowed us to eliminate this patient's stone burden with a minimal number of procedures.
Conclusion
Our report demonstrates a rare presentation with complex ureteral anatomy and highlights the importance of a staged approach to ensure stone clearance. In addition, a combination of different treatment modalities may be required as both ureteroscopic and percutaneous management were performed to increase efficacy and minimize any further procedures for this patient.
Footnotes
Disclosure Statement
No competing financial interests exist.