
Abstract
Abstract
Background:
Percutaneous nephrolithotomy (PCNL) is a procedure typically performed under general anesthesia (GA); however, many patients might be considered unfit for GA and locoregional anesthesia is their only chance to have the procedure done.
Case Presentation:
A 60-year-old Middle-Eastern female with end-stage lung disease underwent evaluation for lung transplant; she was found to have severe restrictive pattern on steroid and continuous oxygen therapy, pulmonary hypertension with dilated right ventricle, chronic anemia, and asthma. She had kidney stones for 10 years, having spontaneously passed several in the past. During work-up for a lung transplant, she was found to have bilateral staghorn calculi and was referred to urology for stone management before lung transplant. After insertion of a Double-J stent for management of worsening right hydronephrosis, antibiotic therapy for extended spectrum beta-lactamases Klebsiella pneumoniae, and optimization after two procedure cancellations because of new onset of cardiovascular issues, she had a simultaneous bilateral PCNL under thoracic epidural anesthesia in two stages within 48 hours without significant complications. She was rendered stone-free and a candidate to be added to the lung transplant list.
Conclusion:
Bilateral prone PCNL under epidural is a safe and effective option in high anesthetic risk patients.
Introduction and Background
Percutaneous nephrolithotomy (PCNL) is the gold standard treatment for renal stones >2 cm. Although typically performed under general anesthesia (GA), many patients are considered unfit for GA and locoregional anesthesia is their only option to have the procedure done. Here we describe a case of simultaneous bilateral PCNL performed under epidural anesthesia in a very high-risk patient.
Presentation of Case
We present a case of a 60-year-old Middle-Eastern female with end-stage lung disease because of history of interstitial lung disease (Fig. 1), undergoing evaluation for lung transplant; she had a severe restrictive pattern (FEV1 = 25%, FVC = 24%), and was on steroids and continuous oxygen therapy (2 L/min at rest). She also had right ventricle severe pulmonary hypertension (RVSP = 84 mm Hg) with right ventricle (RV) dilation, gastroesophageal reflux disease, chronic anemia, and asthma. She had normal BMI (23.4). She reported a history of nephrolithiasis for 10 years, previously passing stones without urologic intervention. She had two urinary tract infections in the past but was asymptomatic at the time of our evaluation. During work-up for lung transplant, she was found to have bilateral staghorn calculi. This was considered an infectious risk that would preclude her from proceeding with lung transplantation, particularly considering the need for post-transplant immunosuppression, and she was referred to urology for stone management before transplant.
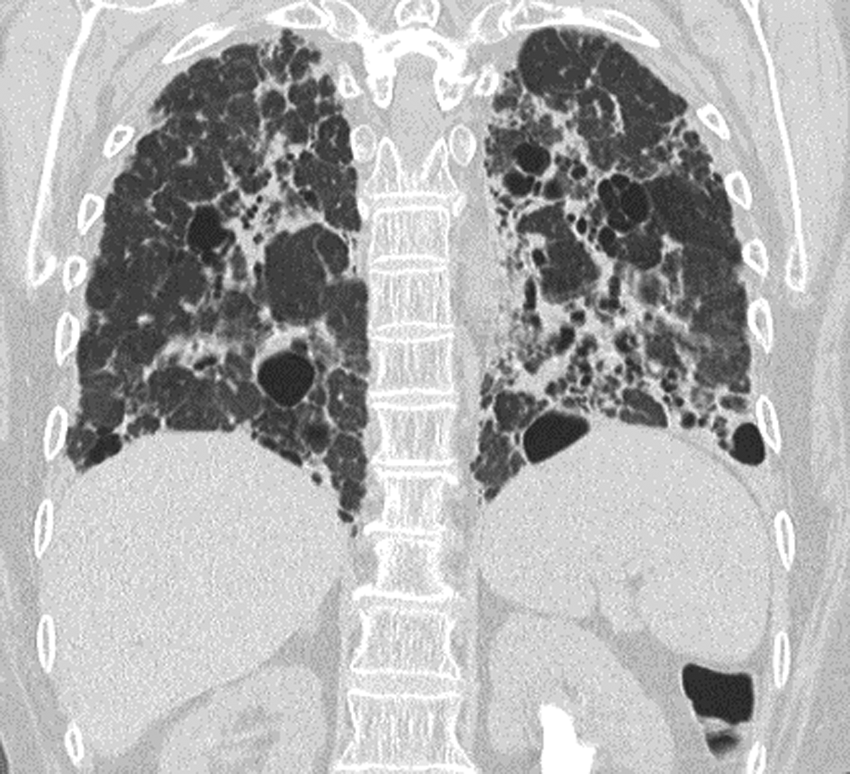
Chest CT showing severe pulmonary fibrosis.
In the urology clinic, she was found to have significant pyuria and bacteriuria on urinalysis. CT imaging confirmed bilateral staghorn renal calculi (right: 4 cm; left: 3 cm) (Figs. 2 and 3). There was also a 2.2 cm cystic lesion on the right kidney; subsequent ultrasonography confirmed a hyperdense cyst. At this time, the patient was considered for bilateral PCNL but surgery was deferred as the patient was not cleared for GA. She was treated with ciprofloxacin for extended spectrum beta-lactamases (ESBL) Klebsiella pneumoniae, but infection persisted.
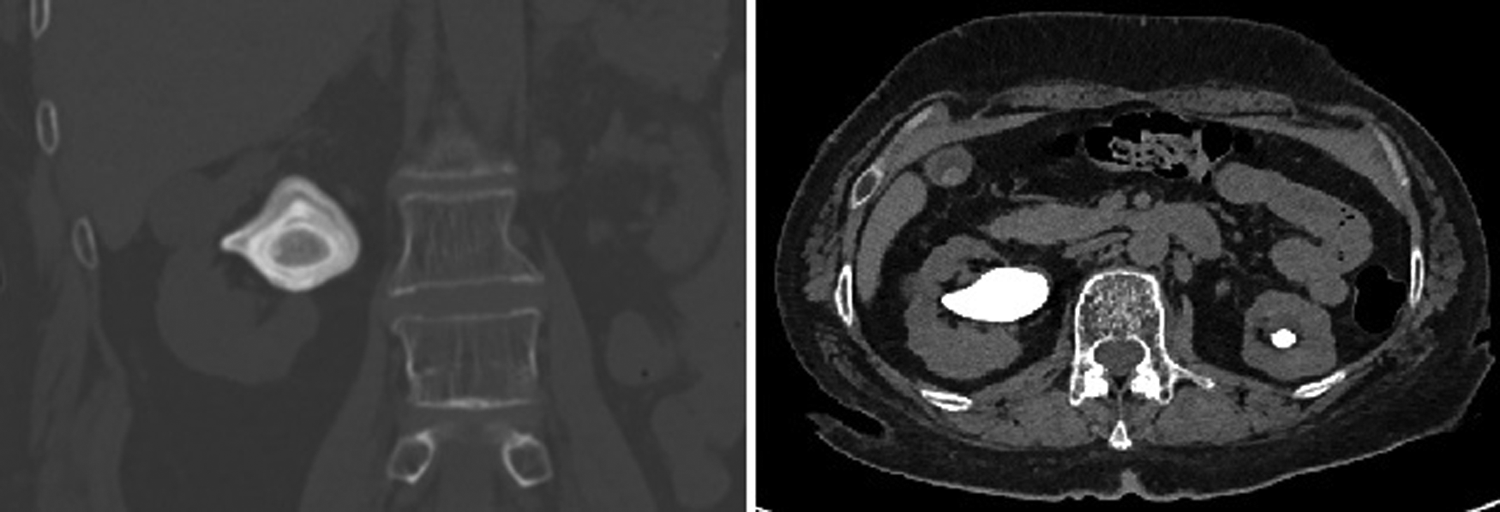
Right kidney stone on CT.
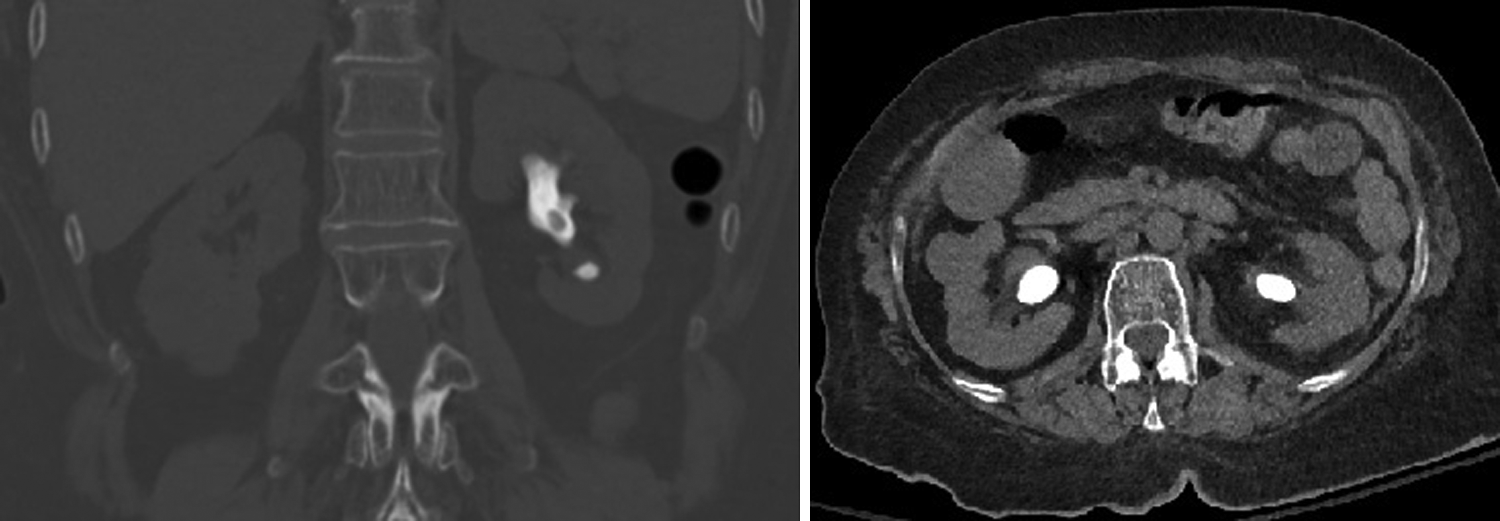
Left kidney stone on CT.
Three months after initial referral, she was seen in the emergency department with worsening shortness of breath. She was found to be in septic shock (febrile, tachypneic, tachycardic 150 bpm, hypotensive with systolic BP of 70 mm Hg, and with increased O2 requirement). She was admitted to the medical intensive care unit and treated with intravenous (IV) meropenem. Transthoracic echocardiogram (TTE) showed increased LVEF 68%, concentric hypertrophy of left ventricle, RVSP 84 mm Hg, and flattening of interventricular septum caused by RV overload. After recovery, she was discharged back to her rehabilitation institution. However, 2 weeks after discharge, she noticed increased urinary frequency, right flank pain, and low-grade temperature (100.4F). She was again admitted to the medical intensive care unit and treated with broad-spectrum antibiotics. CT imaging showed new right hydronephrosis. After stabilization with vasopressors, she underwent emergent cystoscopy and right Double-J stent insertion under IV sedation with propofol (12.6 mg) and ketamine (10 mg). Within a week, she had recovered of her septic shock and was considered for bilateral PCNL. However, the procedure was cancelled because of new onset of T-wave inversions on electrocardiogram (EKG). Subsequent TTE showed new onset diastolic dysfunction and was followed by a sestamibi dobutamine rest stress, which showed no cardiac ischemia. Transient hyperkalemia was treated. Antibiotic therapy was changed to meropenem after urine culture with ESBL K. pneumoniae. The procedure was again cancelled because of a 5.5-second pause on EKG monitoring, which was later attributed to vasovagal stimulation.
She was evaluated in a multidisciplinary manner by the medical intensive care unit, cardiology, pulmonology, transplant surgery, infectious diseases, anesthesia, and urology. She was considered unfit for a GA because of cardiopulmonary concerns and her end-stage lung disease. Therefore, PCNL was planned under epidural anesthesia.
Two weeks after stent insertion, she underwent bilateral PCNL under thoracic (T8-9) epidural anesthesia with 45 mg of lidocaine as a test dose, followed by loading dose of bupivacaine 15 mg and subsequently started on bupivacaine 12.5 mg/h infusion and tapered to 5 mg/h during the surgery. Two teams operated simultaneously on the two kidneys, minimizing surgical time to 195 minutes (Fig. 4). Lower pole access was chosen to avoid lung complications. The access tract was dilated with NephroMax™ balloon with Encore™ 26 inflator (Boston Scientific, Boston, MA) up to 30F. Stone fragmentation was performed with Olympus ShockPulse-SE ultrasonic lithotripsy through a rigid nephroscope. Intraoperatively, she experienced hypotension requiring vasopressors, and was given 1 U of blood intraoperatively. Oxygen saturation was stable >96% with O2 at 3 L/min. Bilateral 7.1F ureteral stents and 22F Councill-tip nephrostomy tubes were left for access. Postoperatively, the epidural was removed and the patient did well with mild pain managed with IV hydromorphone. Stone analysis revealed stone composition as 80% uric acid and 20% calcium oxalate monohydrate. CT on postoperative day 1 showed residual stone fragments bilaterally with a maximum of 10 mm on the right and 8 mm on the left. There were also fragments in the proximal right ureter and a 4 mm calculus at the right ureterovesical junction.
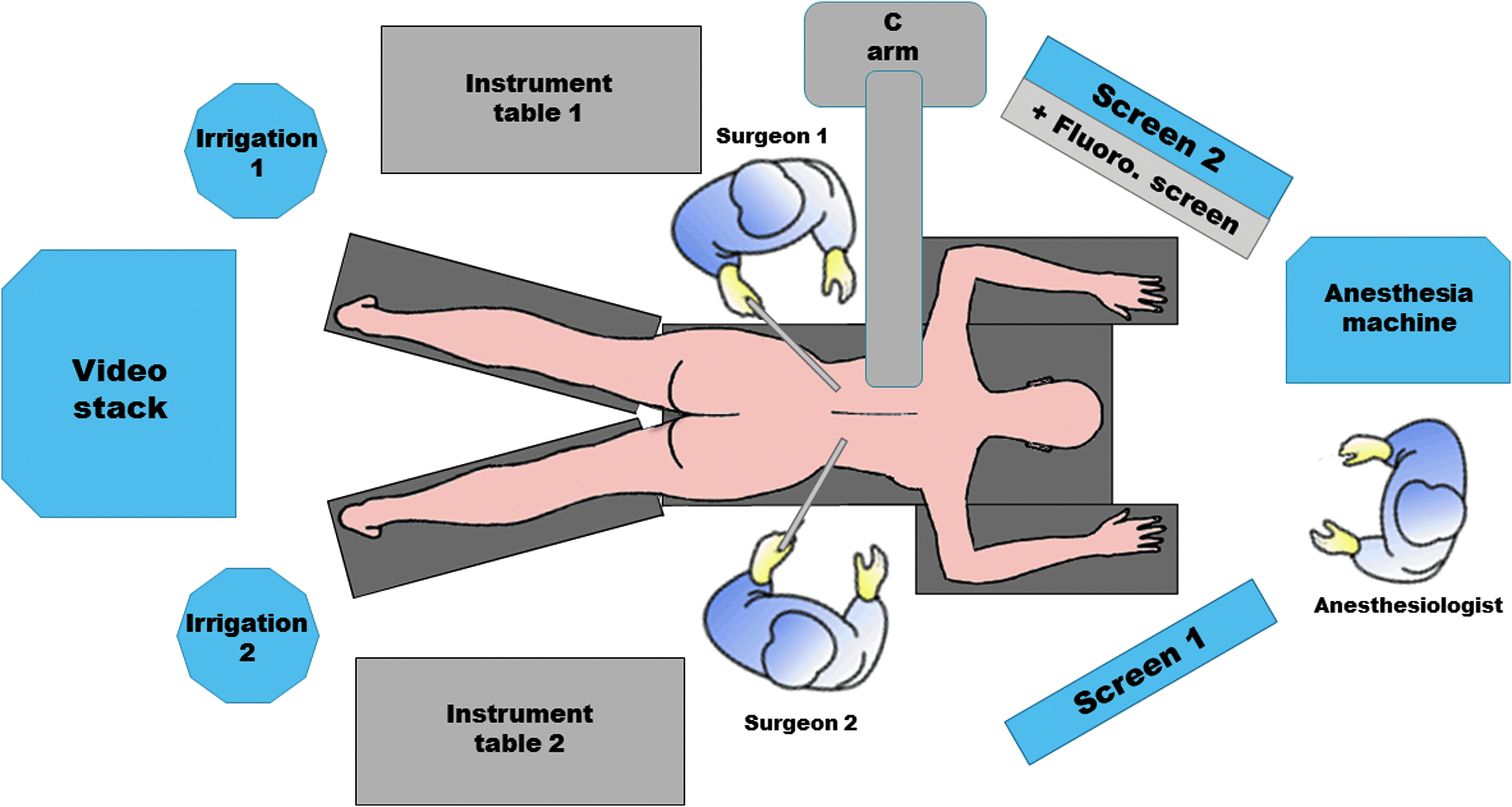
Operating room set-up for simultaneous bilateral PCNL. PCNL, percutaneous nephrolithotomy.
Three days after first PCNL, she underwent a second look PCNL again using thoracic epidural anesthesia with a similar anesthetic technique as the initial surgery. Again, simultaneous flexible nephroscopy was performed on both kidneys to reduce operative time, and antegrade flexible ureteroscopy was used to remove ureteral stones. Only a right 22F nephrostomy tube was left in place. Stone analysis from the second look revealed 80% calcium oxalate monohydrate and 20% ammonium hydrogen urate. The patient recovered well without issues, and on the second postoperative day, the right nephrostomy was removed and meropenem discontinued. Follow-up CT after discharge showed only small fragments <2 mm bilaterally in each renal collecting system present.
Discussion and Literature Review
PCNL is typically performed under GA and, at our institution, prone position is preferred. However, this position may lead to elevated intra-abdominal pressure and resulting in decreased functional residual capacity, end-expiratory lung volume, and total lung capacity, particularly in morbid obese patients.
Previous studies have shown the feasibility of PCNL under locoregional anesthesia, taking advantage of the fact that most of the pain seems to come from renal capsule distention. Ecke et al. reported 439 cases of PCNL under local anesthesia (LA) of the nephrostomy tract with 15–20 mL of ropivacaine. 1 However, 48.5% of patients required conversion to intravenous analgesia, sedation, or endotracheal intubation.
Regional anesthesia has been found to be very efficient in pain control as we can infer from the Bucholz group report of 22 PCNLs in high-risk patients (ASA score ≥3) under spinal and/or epidural anesthesia (T12-L1). 2 These PCNLs were performed in lateral decubitus position in an attempt to improve pulmonary function in obese patients and avoid complications from nausea and vomiting. None of the patients required conversion to GA and even upper pole access was managed with the addition of more LA.
Although perhaps not sufficient by itself, LA seems to improve pain control when associated with regional anesthesia as Sharifi and colleagues reported in a randomized trial of nephrostomy tract instillation with bupivacaine after PCNL under spinal anesthesia; LA was found to decrease the need for more systemic narcotics and provide acceptable analgesia in the postoperative period. 3
The feasibility of simultaneous bilateral PCNLs has been described before by Nadler et al., resulting in less postoperative discomfort, less morbidity, and quicker recovery, particularly with the addition of spinal subarachnoid morphine sulfate to GA. 4
The greatest concern in these high-risk patients is that the already high complication rate of a PCNL is aggravated by their extensive comorbidities, resulting in longer rehabilitation or even death. 2 The aforementioned studies did not show any increased risk of complications with LA 1 or regional anesthesia. 2
Conclusion
Traditionally performed under GA, PCNL has been reportedly done under locoregional anesthesia in several studies for diverse reasons, but high anesthetic risk remains the strongest indication. To our knowledge, this is the first reported case of simultaneous bilateral prone PCNL under regional anesthesia. This was an extremely frail patient with end-stage lung disease who could only be considered for lung transplantation after management of her stones. Our technique of bilateral PCNL under thoracic epidural anesthesia was a safe and effective option for this very high anesthetic risk patient and should be considered in extreme cases like this.
Footnotes
Disclosure Statement
No competing financial interests exist.