
Abstract
Iatrogenic ureteral injuries account for ∼75% of all ureteral injuries and occur primarily during urologic, gynecologic, general, and vascular surgery procedures. Ureteral injury during spine surgery is a rare complication with only occasional reports in the literature. In this case report, we present a case of unrecognized left ureteral injury during an open right lumbar discectomy with a delayed presentation, and discuss the steps required for diagnosis and management. This report highlights a rare complication during laminectomy and serves to better inform patients and surgeons about this potential complication and the management options.
Clinical History
The patient was a healthy 83-year-old male with a right L3–L4 lumbar disk herniation, resulting in right lower limb radiculopathy. He underwent an elective right lumbar microscopic discectomy with inferior L3 and superior L4 laminotomy through a posterior lumbar approach, performed at a tertiary care center. The procedure was uncomplicated and he was discharged home on postoperative day 6 after requiring intermittent bladder catheterizations for urinary retention. He had minimal pain and was ambulating well independently.
Within a few days of discharge, he noted new onset of pain in the left lower quadrant of the abdomen and the left thigh. This pain was similar in nature to his preoperative right-sided thigh pain and gradually increased until he presented to the emergency department on postoperative day 50.
On examination, his vital signs were within normal limits. He was lean and his body mass index (BMI) was 23 kg/m2. He had left-sided flank tenderness to percussion. The laboratory blood results were within normal limits. His urinalysis was negative for nitrites, blood, and leukocytes. Urine culture was negative.
Diagnosis
The patient underwent a CT scan of his abdomen and pelvis with intravenous contrast. This showed a large lobulated fluid-filled retroperitoneal mass surrounding the left psoas muscle with left hydronephrosis (Fig. 1a). Contrast was seen in the left renal pelvis and ureter with contrast entering the mass at the level of L3 (Fig. 1b). His right kidney appeared normal and no other abnormalities were identified.
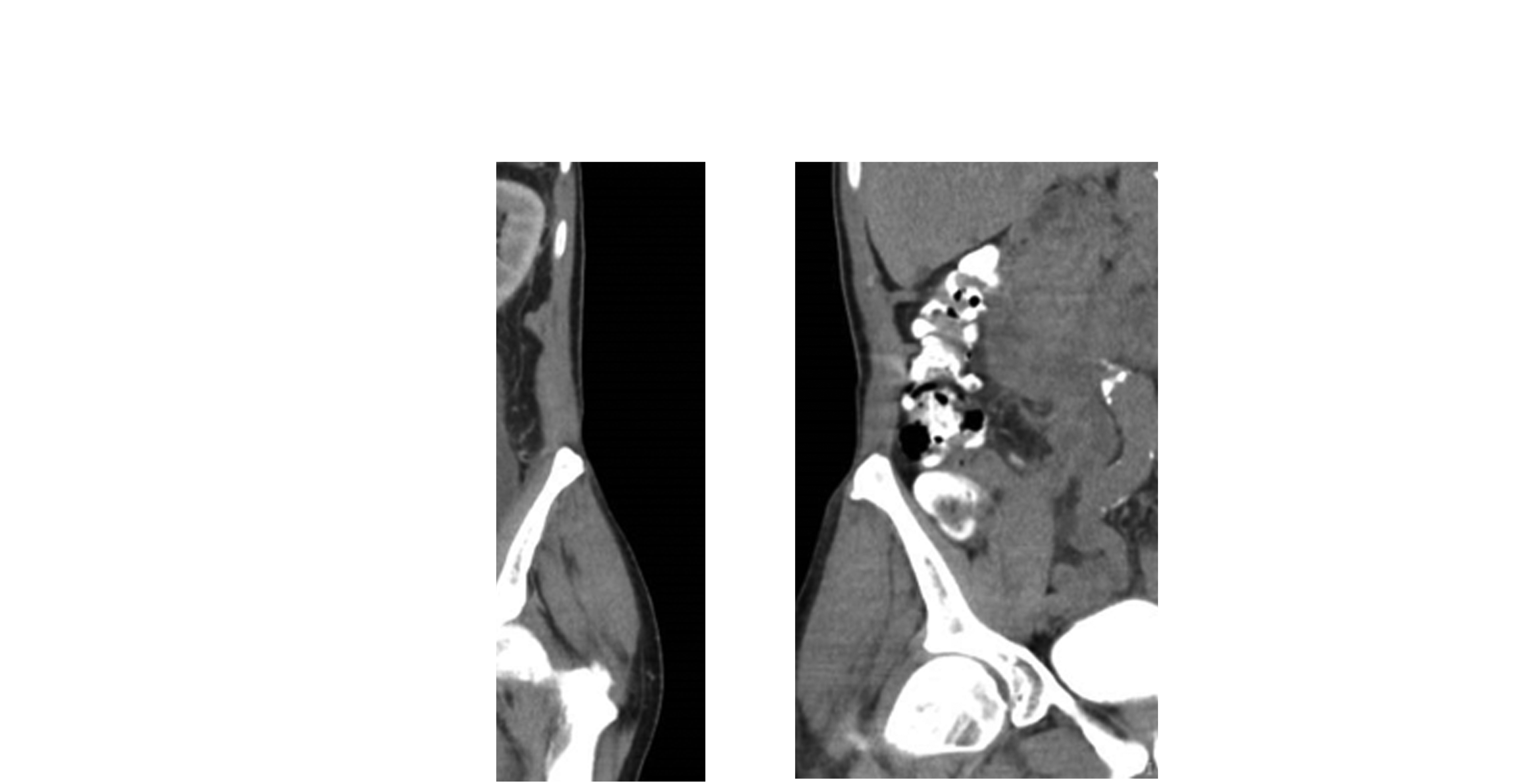
CT scan of abdomen and pelvis.
Intervention
A percutaneous drain was placed into the urinoma and a left-sided nephrostomy tube in renal pelvis. Antegrade nephrostogram shows a blind-ending proximal ureter (Fig. 2). Insertion of a nephroureterostomy tube (NUT) was not attempted at this time. The patient underwent cystoscopy and left retrograde ureterogram with simultaneous nephrostogram, which showed a retrograde left ureteral injury at the level of L3–L4 (Fig. 3a). The lack of contrast flowing between the proximal and distal ureter confirmed a complete ureteral disruption with a 5 cm defect (Fig. 3b). Attempts to simultaneously pass a retrograde hydrophilic guidewire and an antegrade NUT were unsuccessful.

Left nephrostogram showing a blind-ending ureter.
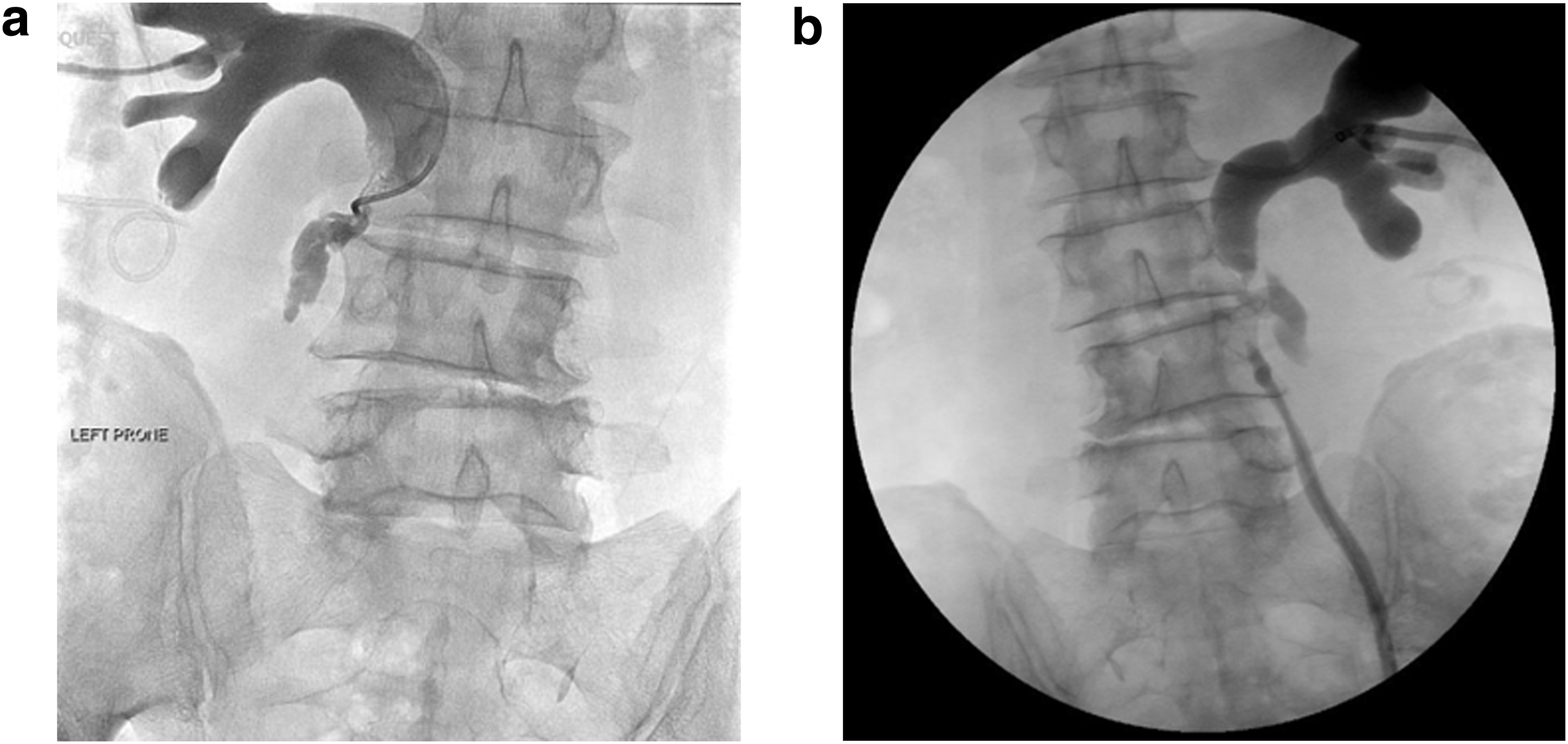
Left retrograde ureterogram with simultaneous nephrostogram.
He convalesced in hospital with nephrostomy tube to open drainage and his pain improved. Repeat CT scan showed complete resolution of the urinoma and the percutaneous drain was removed. Management options were discussed with the patient. An end-to-end ureteroureterostomy or distal ureterovesicostomy with psoas hitch/Boari flap was not considered to be feasible because of proximal location and long ureteral defect. The patient was offered permanent nephrostomy tube, ileal neoureter, autotransplant, or nephrectomy. The patient opted for a nephrectomy given his advanced age, normal renal function (creatinine 57 μmol/L), and normal contralateral kidney. The patient underwent effective and uncomplicated laparoscopic nephrectomy. He was discharged home on postoperative day 3 after the nephrectomy.
Follow-Up
His recovery was uneventful and postoperative creatinine was normal (72 μmol/L) in follow-up.
Discussion
Discectomy involves the surgical removal of a herniated disk. In the posterior approach, a vertical incision was made from the upper spinous process to the lower. The muscle and aponeurosis are incised and dissection is carried down until the ligamentum flavum is exposed and then opened. Fluoroscopy is performed to confirm accurate positioning. The dura is mobilized medially and partial laminectomy is performed, if needed, to expose the herniated disk and compressed nerve. The nerve root is moved off the hernia and the common vertebral ligament is incised. Disk excision is then performed. Care is taken not to cross the anterior vertebral ligament, and curettage of the plates should not be attempted. After lavage and assessing for hemostasis and cerebrospinal fluid leakage, the aponeurosis, fascia, and skin are closed. A drain can be placed if preferred. Typical postoperative course includes a 24–72-hour hospital admission. 1
Complications after discectomy commonly include recurrence of disk hernia, dural tear, injury to nerve root or thecal sac, and epidural bleeding. Ureteral injury is infrequently reported as a complication of discectomy. 2 Management options include stenting, ureteroureterostomy, autotransplantation, ilealneoureter, and nephrectomy. All of these options have been reported. 2
The ureter is a retroperitoneal structure coursing from ureteropelvic junction to the urinary bladder. It is located just lateral to the tips of the transverse processes of the lumbar vertebrae and is anterior to the psoas muscle. More distally, the ureter crosses the ventral surface of transverse processes of the third to fifth lumbar vertebrae and enters the pelvis over the bifurcation of the common iliac vessels. The proximity to lumbar vertebrae and disk places the ureter at a risk of injury during posterior lumbar discectomy, especially at the level of L4–L5. 2
Patient factors that can increase the risk of ureteral injury during posterior discectomy include absence of the anterior annulus that can provide another layer of protection to the ureter, previous retroperitoneal surgery with local scarring, and lean patient with lack of retroperitoneal fat where ureter will be even more proximal to the vertebral bodies. 3 Surgical factors increasing the risk of ureteral injury include misuse of rongeur type instruments, prone positioning, supporting pelvic bolsters that push the ureter more posteriorly closer to the vertebrae, and distal lumbar vertebrae surgical site where ureter courses more medially. 3
In the limited previous reports, ureteral injury tends to be on the contralateral side to discectomy. 4 This has been described because of tangential passage of instruments. In our case, the injury was also contralateral and at the level of L3–L4 where the ureter is anterior to the psoas muscle and moving medial toward the vertebrae. Also, our patient was lean with BMI of 23 kg/m2, placed in prone position with bolsters at the time of discectomy. Furthermore, preoperative MRI indicates a dilated ureter at this level, which would increase the likelihood of injury and possible mechanism contributing to continued leakage (Fig. 4). Factors such as large disk herniation and excessive bleeding likely further contribute to occurrence of this complication. 4 As with most iatrogenic ureteral injuries, these can be prevented with more experience, careful planning, and patient positioning, along with review of preoperative imaging.
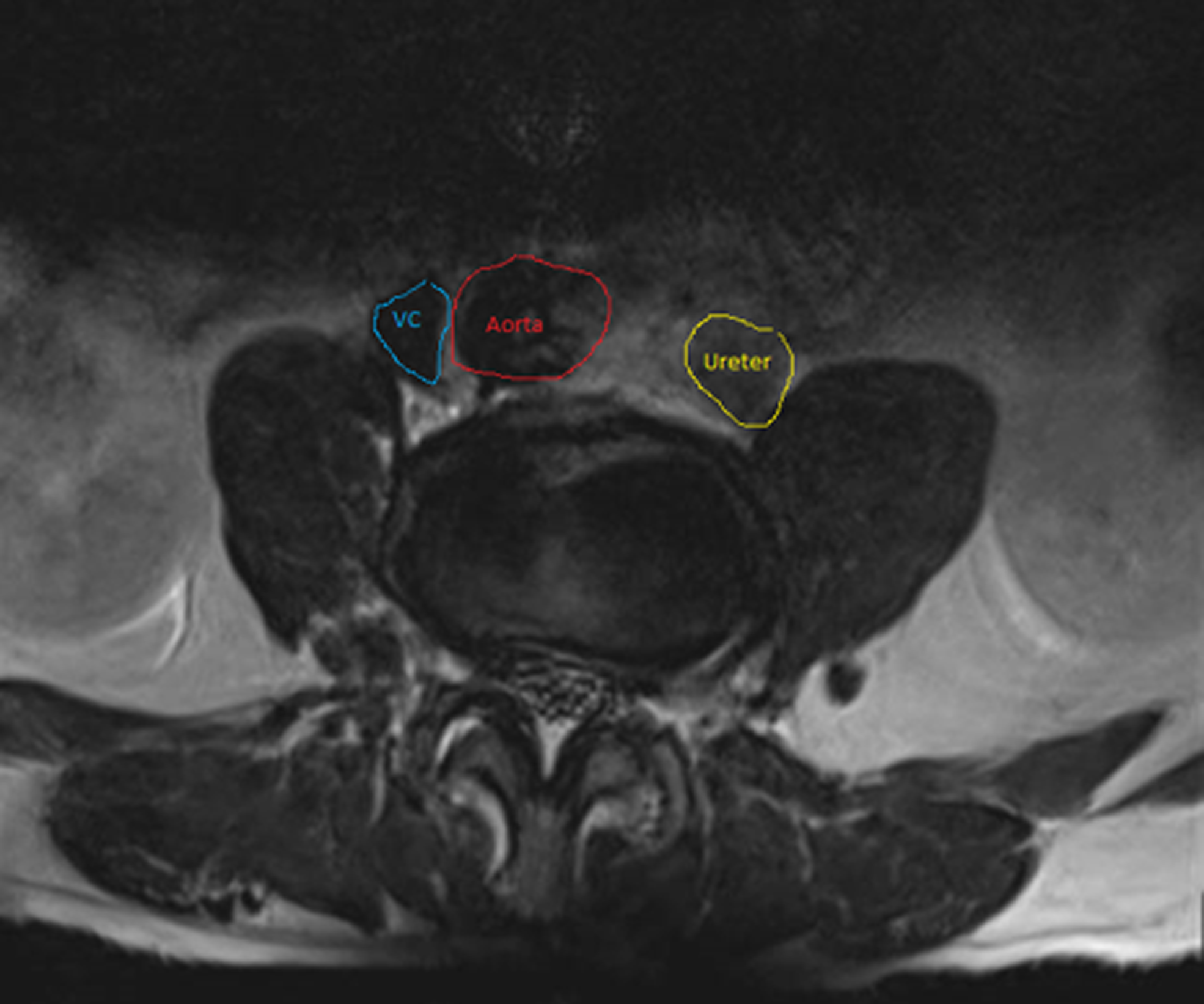
Preoperative MRI showing prone positioning of the ureter at the level of L3/L4 and dilated ureter at this level.
There is paucity of information with regard to diagnosis and management of ureteral injury related to posterior discectomy. Urologists can utilize their experience from management of other iatrogenic ureteral injuries more common with gynecologic and pelvic surgery in diagnosis and management of ureteral injury after discectomy. The timing of presentation in relation to index surgery can vary from days to months or years depending on severity of patient symptoms. 5 These symptoms can include flank pain, fever, ascites, ileus, urinary incontinence, anuria, azotemia, and nonfunctional kidney resulting from 5% of patients presenting late with hydronephrosis. 5 In the case of our patient, immediately postoperatively he had urinary retention with clear urine and minimal but increasing pain. His lack of specific symptoms and late presentation to the emergency department delayed diagnosis until 2 months after surgery.
The first step in the management of ureteral injury follows the general urologic principles, which include attempts at realignment and re-establishment of urinary drainage with a ureteral stent or, if not possible, a percutaneous nephrostomy tube. 6 Percutaneous drainage of any large urinoma is recommended as it can alleviate symptoms and allow more clear assessment of location and severity of injury. The placement of the drain is also crucial in managing patients presenting with sepsis. Location and extent of ureteral injury will determine the available options for definitive repair of ureteral injury.
In case of posterior discectomy, the location of ureteral injury is usually proximal ureter, which can be more challenging for definitive repair, especially if a large segment of the ureter is involved or diagnosis is delayed, resulting in significant local inflammation and scarring. In this case, given the proximal ureteral location, long segment of injury, and delayed diagnosis, the definitive repair options were limited. Therefore, because of advanced patient age, normal contralateral kidney, and normal renal function, more complex reconstructive options with increased risk of complications were less desirable. The patient in this case expressed a clear preference against any procedures with a higher risk of complications or secondary interventions, and so elected to proceed with nephrectomy.
Conclusion
Ureteral injury with posterior approach for lumbar discectomy is uncommon but should be suspected in any patient with unknown retroperitoneal fluid collection or complicated postoperative course. Identification with CT urogram and temporizing with stent or nephrostomy tube along with drainage of urinoma with percutaneous drain insertion are recommended. An attempt at stenting in a retrograde and/or antegrade manner is one of the first steps in management. Definitive management may require endoscopic or surgical techniques following the general urologic principles in management of ureteral injury depending on patient characteristics, location, and extent of the ureteral injury.
Footnotes
Disclosure Statement
No competing financial interests exist.