
Abstract
Abstract
Background:
Fistulae between the prostatic urethra and the rectum are rare. They may result from prostatic or rectal surgery. Predisposing factors are previous radiation or immunosuppression. The repair of such fistulae usually involves major surgery. Recently, clips that can be deployed over an endoscope have been developed to close gastrointestinal fistulae or access points for natural orifice surgery. We report the first case of effective treatment of a prostatorectal fistula with a rectal “over-the-scope” clip.
Case Presentation:
A 64-year-old man under chronic immunosuppression presented with an iatrogenic fistula between the prostatic urethra and the rectum after transurethral resection of the prostate. A transverse colostomy was placed but the fistula failed to heal conservatively. The fistula was effectively closed with an endorectal clip. Six weeks after the procedure, spontaneous micturition was started. Two weeks further, the colostomy was reversed. At 32 months of follow-up, the remains closed, micturition is unimpaired.
Conclusion:
In select cases of prostatorectal fistula, an endorectal clip may be effectively used for closure.
Introduction and Background
Fistulae between the prostatic urethra and the rectum are rare. Known causes of a prostatorectal fistula are external beam radiation and/or brachytherapy, cryotherapy, high-intensity focused ultrasound for the treatment of carcinoma of the prostate. 1 It has also been described as a complication of local trauma and of surgery of the prostate, namely radical prostatectomy or transurethral resection of the prostate. Predisposing conditions may be immunosuppression, diabetes, and previous radiation. Surgical repair of a prostatorectal fistula is a major operation and requires considerable surgical expertise.2,3 There is considerable risk of failure and fecal or urinary incontinence. Therefore, some patients may seek for a simpler and less invasive treatment. We report the first effective use of a new minimally invasive technique using an endorectal clip.
Presentation of Case
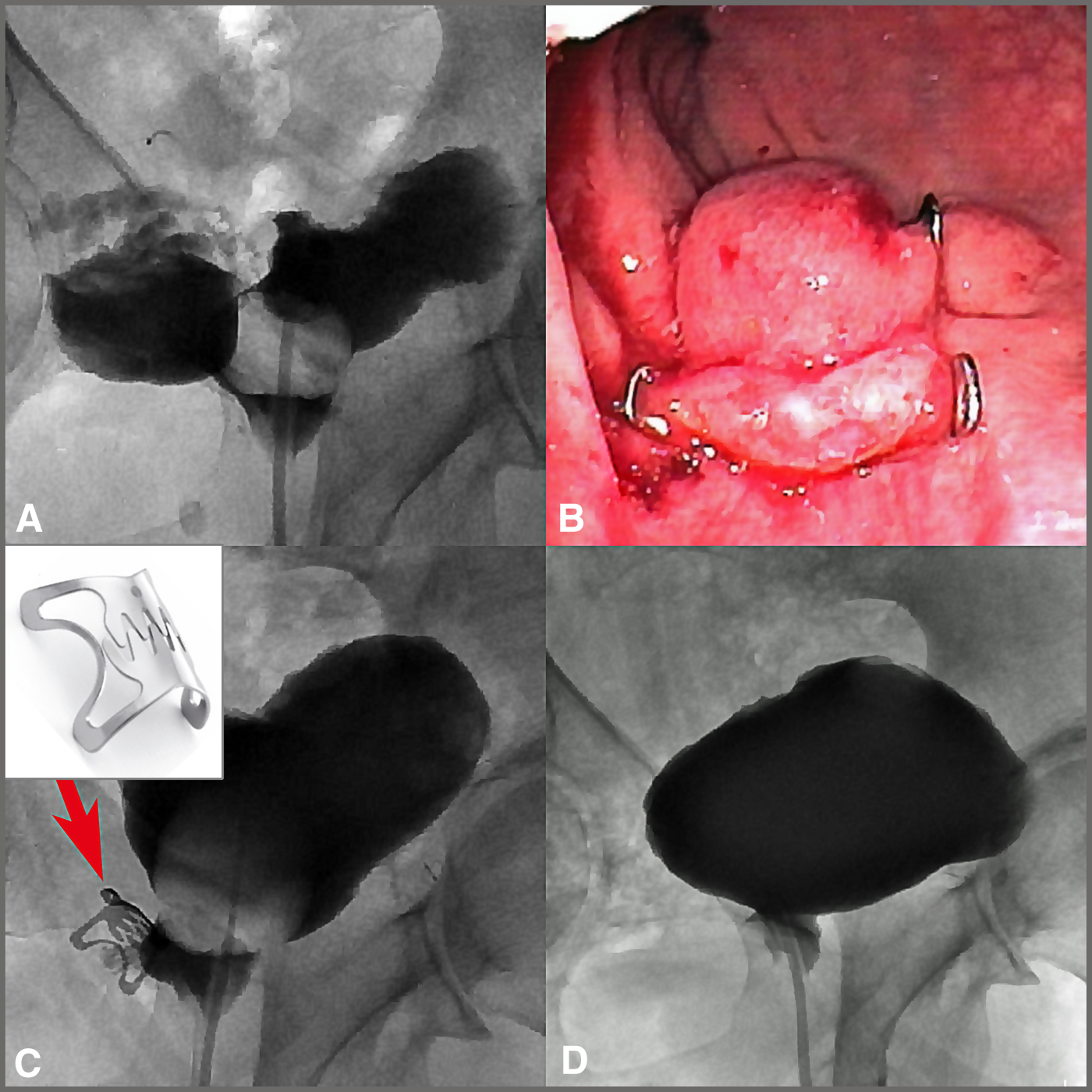
A 64-year-old man presented with chronic obstructive bladder outlet symptoms. Urinary maximum flow was 8 mL/s, residual urine measured 150 cc, International Prostate Symptom Score was 18, and serum prostate specific antigen was 1.4 ng/mL. The patient had been under chronic immunosuppression for Crohn's disease with oral steroids for ∼20 years. Transurethral resection of the prostate was carried out in August 2013. Histopathologic evaluation of the resection chips confirmed benign prostatic hyperplasia. After removal of the transurethral catheter, micturition started spontaneously on day 2, but transanal loss of urine was noted. Flexible urethrocystoscopy and cystography demonstrated a fistula originating from the prostatic resection cavity to the rectum with a diameter of ∼4 mm, taking a slant caudo-cranial course. A transverse colostomy was placed and a transurethral catheter was left indwelling. Subsequently, the patient was treated conservatively and was monitored with regular cystoscopies and cystographies. After 4 months, the fistula had still failed to heal. At this point, surgical reconstruction was suggested to the patient: fistula closure via a transperineal approach and use of a musculus gracilis flap as a buttress. The patient refused any form of surgical reconstruction. Subsequently, in collaboration with our department of gastroenterology, we applied an endorectal clip via a sigmoidoscope to close the fistula from the rectal side under sedation (OTSC® = over-the-scope-clip; Ovesco Endoscopy GmbH, Tuebingen, Germany). Six weeks after the procedure, the transurethral catheter was taken out, no fistula was demonstrable in cystoscopy or cystography (Fig. 1). Spontaneous micturition was started. The fistula remained closed and no complications occurred. Two weeks further, the colostomy was reversed. The further course was uneventful. At 7 and 32 months of follow-up, the patient's micturition is uneventful, no signs of fistula recurrence or urinary tract infection. The clip had been lost spontaneously. Immunosuppressive therapy had been continued during the whole course of the disease.
Discussion and Literature Review
To our knowledge, this is the first report of the repair of a prostatorectal fistula with an endorectally applied clip. The clip that we used is made from nitinol. It is introduced via a transanally introduced colonoscope or sigmoidoscope and is deployed as an OTSC. Its effective use in different clinical situations such as bleeding, management of complications subsequent to endoscopic or surgical intervention, and closure of gastric, colonic, or rectoanal fistulae has recently been reported by others. 4 The clip may be removed after several months using a specially devised clip cutter, which we did not. In our patient, it was probably egested spontaneously.
The body of literature on the repair of prostatorectal fistula is limited. Occasionally, a prostatorectal fistula may heal spontaneously with or without transient placement of a colostomy. However, in nearly every case of prostatorectal fistula, surgical interventions will be necessary to close it.2,3 Conservative therapy failed in our patient despite colostomy and indwelling catheter for 4 months.
The local use of fibrin glue or dextranomer to close the fistula has been described, but satisfactory results are improbable. Established methods for surgical repair of prostatorectal fistulae will comprise the excision or freshening of the fistula wall and closure of the defect in the rectum. It should also be attempted to close the defect in the prostatic capsule, which may be more difficult or even impossible because of insufficient mobility of the residual prostate surgical capsule or poor tissue quality. Surgical access is via abdominal (open or laparoscopic), perineal, or posterior transsphincteric route. A case of fistula repair via transanal endoscopic microsurgery has recently been described. 4 Especially if a fistula is large in size or if it is postradiation, a pedicled buttress, such as omentum, dartos island flaps, rectus muscle or favorably gracilis muscle, will be strongly advisable. In desperate cases, radical prostatectomy or bladder neck closure with mitrofanoff stoma or even cystectomy with urinary diversion will have to be carried out.
The technique described herein is a novelty and its long-term results and limitations (fistula size, location, postirradiation) are yet to be defined.
We feel that in the case that clip closure had failed in our patient, open surgical reconstruction would still have been possible without having been impaired by the previous endoscopic clip placement.
Conclusion
In select cases of prostatorectal fistula, an endorectal clip may be effectively used for closure. Because of the elegant and minimally invasive nature of the procedure, further studies on the treatment of urorectal fistula with these clips are justified.
Footnotes
Disclosure Statement
No competing financial interests exist. The views expressed herein are those of the authors and do not reflect the official policy or position of Augusta Urology or Witten/Herdecke University.