
Abstract
Abstract
Background:
Although the breakage of a Sachse's knife blade is already a rare event while performing optical internal urethrotomy, a double failure appears to be at the same time a unique and a challenging complication to manage since no reference has emerged from literature review.
Case Presentation:
A male patient, 80 years of age, underwent retreatment of recurrent urethral stricture that occurred after transurethral resection of the prostate. The latter was complicated by severe intraoperative urethrorrhagia; this is the reason he was transferred from another institution where at first a suprapubic cystostomy was carried out, followed by urethral recanalization through internal urethrotomy and finally he underwent intracavernous Sachse's knife blade discharge. Preoperative evaluation included combined retrograde and voiding urethrography and CT to evaluate the complete resolution of the urethral stenosis and to establish the correct location of the blades inside the corpus cavernosum. A transperineal approach to the left corpus cavernosum was carried out with manageable removal of the foreign body and postoperative assessment showed no early considerable complications for the patient.
Conclusion:
To our knowledge, this is the first case of double breakage of Sachse's knife blade performing optical internal urethrotomy reported in literature. Although it may appear to be an easy procedure, close attention to its execution must always be paid to prevent major complications. A transperineal approach has proven to be effective and safe without creating any further outcomes to the patient.
Introduction and Background
Direct vision internal urethrotomy (DVIU) is well established as a minimally invasive procedure for the treatment of short segmental stricture of the urethra in patients presenting this disease for the first time. Although considered to be a versatile, safe, and efficient endoscopic procedure, it is not free from complications. We would like to report the first case of double intracavernous breakage of Sachse's knife blade that occurred during DVIU and its management.
Case Presentation
Clinical history
On April 2017, an 80-year-old male was transferred from another institution with severe urethrorrhagia and acute urinary retention after a previous unsuccessful DVIU for recurrent urethral stricture after transurethral resection of the prostate (TURP). He was promptly managed with the placement of suprapubic cystostomy enabling complete bleeding control and drainage of about 500 mL of urine. An abdomino-pelvic radiography was then carried out to confirm the presence of a foreign body inside corpus cavernosum, as referred at the time of the patient's admission to hospital, confirming the location of a “metal chip” at the level of the left ischiopubic branch. The patient was discharged after a few days without any complications. On May 2017, the patient was readmitted to the same institution to complete the urethral recanalization. He first underwent abdomino-pelvic CT to establish the exact anatomic location of Sachse's knife blades and a urethrography confirming the presence of urethral segmental stenosis of about 1 to 1.5 cm just above the navicular fossa; no further injury to the urethra was detected. Urethrotomy and urethral recanalization were effectively completed and surgery for final blade removal was planned.
His medical history included arterial hypertension and diabetes; his prior surgery included left inguinal hernioplasty, TURP, and one urethrotomy.
No other relevant pathologies emerged from his medical history.
Physical examination
He was 175 cm tall and weighed 84 kg; his body mass index was 27.4 kg/m2. The abdomen was soft, no remarkable penile abnormalities emerged. Blood pressure was normal and the other remaining vital signs.
Diagnostic studies
Preoperative noncontrast CT-scan (Fig. 1) revealed a metal density foreign body of 17 mm diameter located at the base of corpus cavernosum, close to left ischiopubic branch, and combined retrograde and voiding urethrography showed complete resolution of urethral stricture. Low-dose aspirin was replaced with low-molecular-weight heparin 6 days before surgery. Urine analysis and urine culture were positive for Escherichia coli and a prompt antibiotic therapy, based on specific antibiogram, was carried out. Other laboratory parameters did not show any pathologic findings.
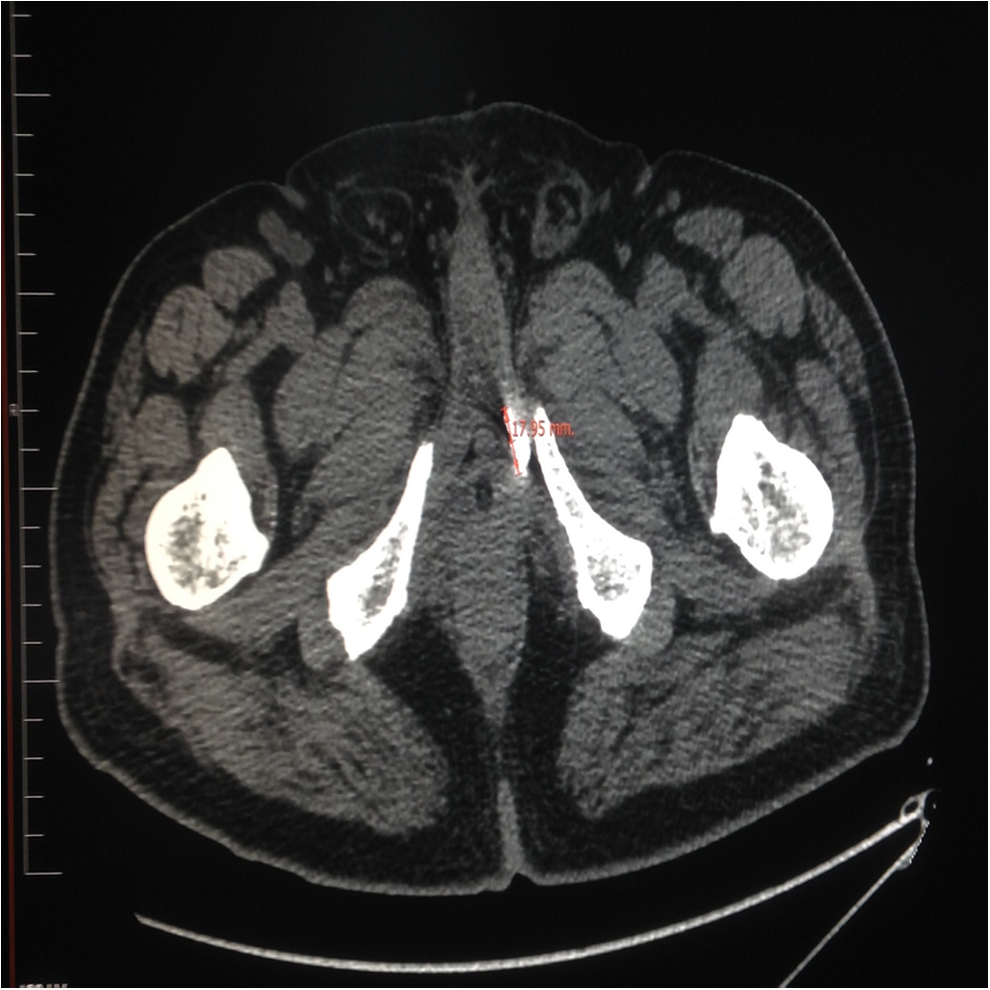
Preoperative CT-scan showing Sachse's knife blades inside left corpus cavernosum, close to homolateral ischiopubic branch.
Intervention
The patient underwent spinal anesthesia and then placed in lithotomic position with hips and knees flexed and thighs apart with the perineum positioned at the edge of the surgical table.
Perineal incision on anus-scrotal raphe was carried out with the exposure of the underlying muscular planes. Left bulbospongiosus and ischiocavernosus muscles were medially incised and lateralized to expose Buck's fascia at the level of the urethral bulbous and proximal end of left corpus cavernosum; urethra and left corpus cavernosum were subsequently isolated (Fig. 2). A landmark was placed on the surface of the corpus cavernosum, and under biplanar fluoroscopic guidance, the correct location of the blades was identified just close to the lower third of left ischiopubic branch. Two no. 0 suture stitches (coated Vicryl® polyglactin 910) were, respectively, placed at 12 and 6 o'clock position to the foreign body to either limit the incision area on the surface of the corpus cavernosum or to rotate its lateral surface for a better exposition. Incision of the tunica albuginea was performed using scalpel blade size no. 15 and tourniquet around penis for bleeding control was not required. The blade discharge was fairly easy thanks to their shallow location (Fig. 3). Corpus cavernosum was sutured using no. 3-0 sutures (coated Vicryl polyglactin 910), and muscular planes were subsequently reconstructed as well as subcutaneous and cutaneous planes. A perineal drain was finally located. Operative time was about 150 minutes.
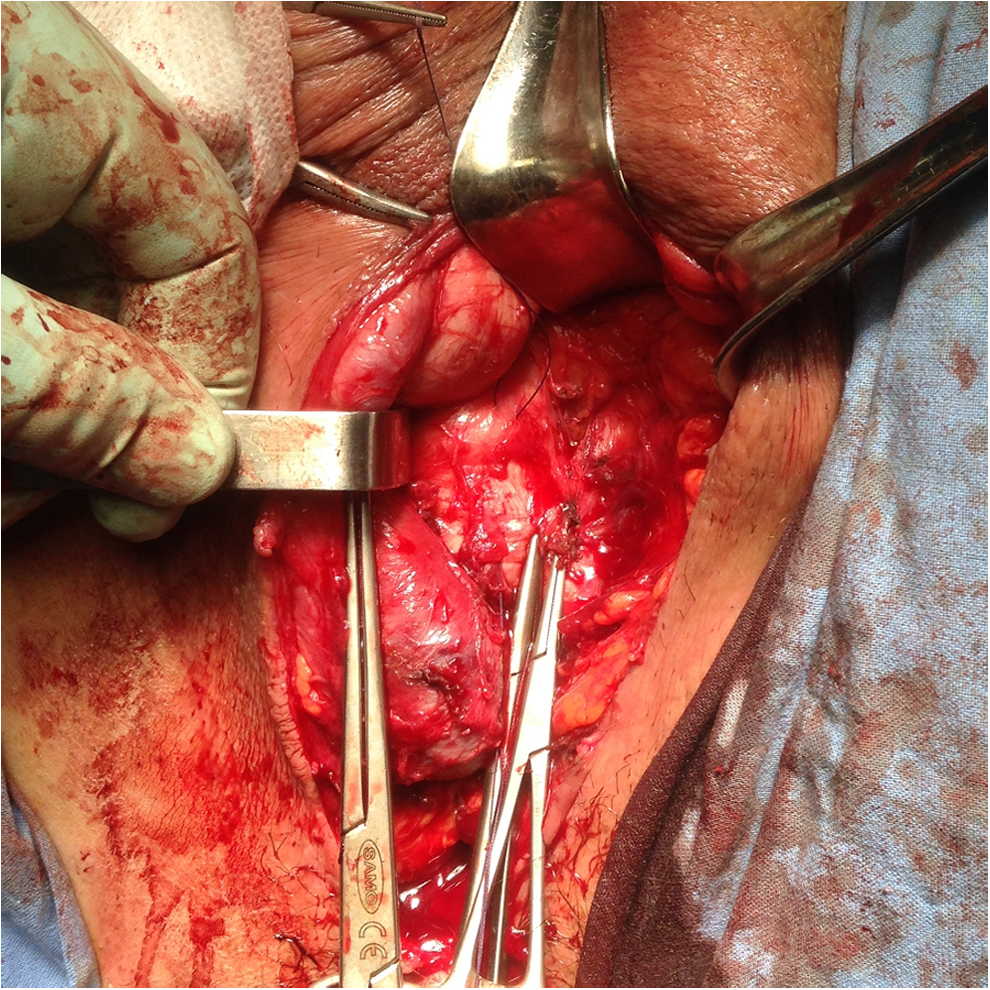
Intraoperative urethral and left corpus cavernosum isolation.
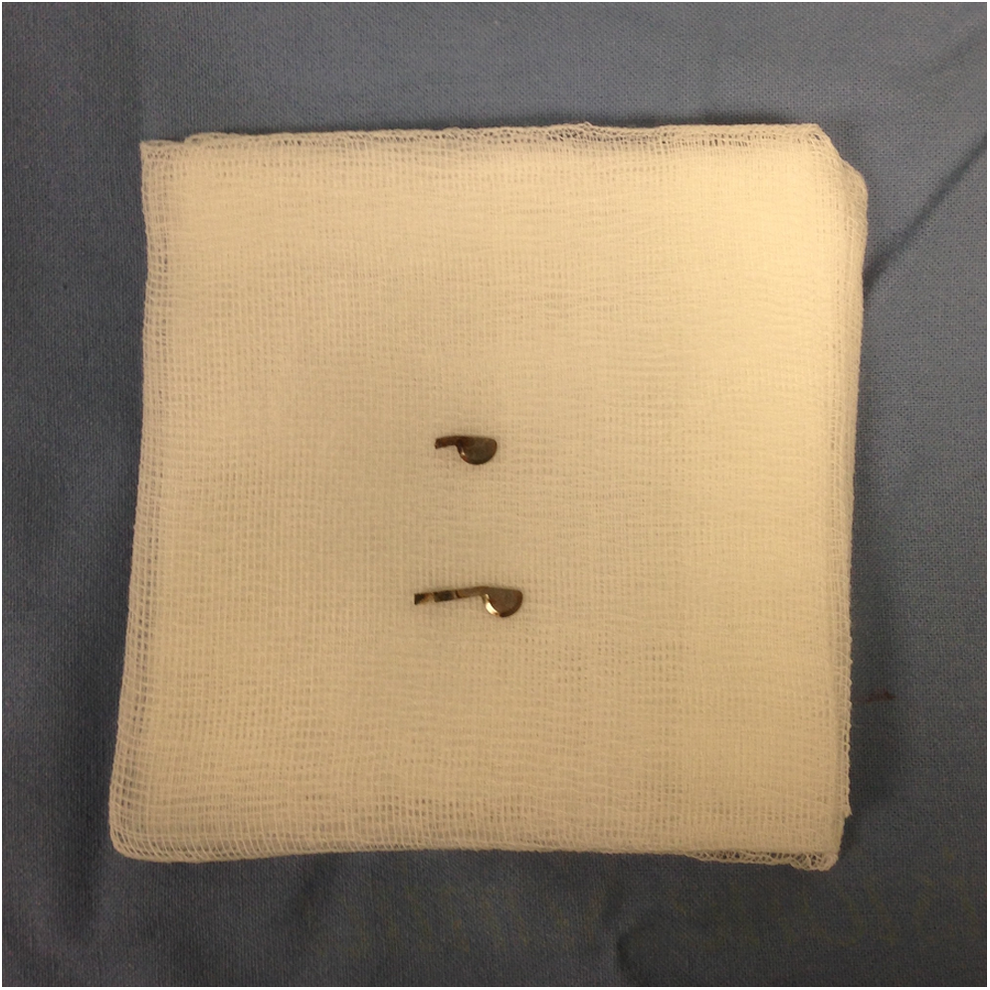
Sachse's blades removed.
Outcome
Postoperative laboratory studies showed stable levels of hemoglobin, hematocrit, platelets, and electrolytes; perineal drain was removed after 2 days. No immediate complications such as local infections, edema, or hematomas emerged. A month after surgery is still too early to evaluate late surgical complications such as erectile dysfunction or corpus cavernosum fibrosis.
Discussion and Literature Review
Urethral stricture is a common and a challenging urologic disease whose effective worldwide incidence remains unclear and seems be influenced by both ethnic and geographic risk factors. Literature evidence reports an incidence of 9.0 per 100.000 in patients aged >65 years compared with 5.8 per 100.000 in patients aged <65 years; black race recorded higher stricture rates compared with whites and bulbar strictures revealed to be more common especially among younger patients. 1
The most common reason for urethral strictures in the United States remains idiopathic (31.9%), followed by iatrogenic (31%) and infection causes (26.6%) particularly due to sexually transmitted diseases; in a high-volume Italian center on a total of 2302 patients reviewed for urethral strictures, idiopathic remains the most common reason of disease (37.8%), followed by failed hypospadias repair (17.1%), trauma (13.8%), catheterization and instrumentation (10.5% and 10.3%, respectively). 1 Concerning the management of urethral strictures, dilatation and/or internal urethrotomy, recently also performed with holmium or thulium laser, are today standard procedures that are readily available and minimally invasive.2,3 Results mainly depend on location, follow-up, stricture length, anatomy, and etiology and the success rate unavoidably varies. It approximately ranges from 20% to 90% even if other authors have reported a success rate varying from 30% to 35% reaching a peak of 70% in short strictures of bulbous urethra (<1.5 cm) without spongiofibrosis after DVIU 4 ; no evident differences were reported among the two surgical procedures in terms of success rate after a period of follow-up of 3.5 years (65% vs 68%). 5 The reported median time to recurrence is 6 months after dilatation and 12 months after urethrotomy and only one study directly compared this outcome between dilatation and DVIU reporting a stricture recurrence 10% greater in the first group, but the difference was not statistically significant. 3
Although considered a safe and minimally invasive procedure, DVIU is not free from complications, including urethral hemorrhage, false passage, perineal hematoma, infections, meatal stenosis, and rectal perforation. According to literature review, only two cases of single intraoperative breakage of Sachse's knife blade have been reported,6,7 but no previous evidence of a double intracavernous split emerged and we wanted to provide the best management of a complication that apparently may seem complex to deal with.
Transperineal approach revealed to be safe and effective to reach the blades inside the corpus cavernosum; their location was deep, just close to the ischiopubic branch and the ideal surgical access to best manage this complication was considered. Preoperative CT and intraoperative biplanar fluoroscopic guidance also gave us the exact anatomic location of the foreign body allowing its removal. It ensures no relevant complications, with hospital discharge of the patient after just few days from surgery.
Conclusion
To our knowledge, this is the first case of double intracavernous breakage of Sachse's knife blade performing DVIU reported in literature. Although it may appear to be an easy procedure, close attention to its execution must always be paid to prevent major complications. A transperineal approach has proven to be effective and safe without giving any further complications to the patient.
Footnotes
Disclosure Statement
No competing financial interests exist.