
Abstract
Abstract
Background:
Continent diversions have since been performed with increasing frequency since the 1950s, with some providers espousing the use of orthotopic diversions as being the new gold standard. However, patients must be counseled to take great care in the maintenance of their diversions because of complications such as metabolic abnormalities, pouch stones, and mucus retention.
Case Report:
A 21-year-old male with a history of posterior urethral valves underwent a continent catheterizable diversion as a child. He is undocumented and without health insurance and as a result unable to follow-up with an urologist for >10 years. He subsequently develops pyocystis with cutaneous fistulization and pouch stones necessitating percutaneous management.
Conclusion:
Patients may benefit greatly from a continent urinary diversion, however, selection must include patients who are able to maintain their pouch and follow-up with their providers to avoid major complications that may occur up to years following the procedure.
Clinical History
A 21-year-old male presented with complaints of left lower-quadrant pain and purulent drainage. He had a history of posterior urethral valves and underwent cystectomy with creation of a continent catheterizable urinary diversion at 4 to 5 years of age and was lost to urologic follow-up, but subsequently developed dialysis-dependent end-stage renal failure at age 12. He catheterizes his stoma three to four times per day with return of 100 to 200 cc of fluid but does not irrigate his diversion, and upon presentation noted increased pain and difficulty with catheterization over the past few months. He stated that during dialysis, he and his nurses noted a painful “pimple” located over his left lower quadrant. This area then progressed to express copious purulent drainage that prompted him to present to the emergency department (ED).
Physical Examination
Upon presentation to the ED, vitals were temperature 37.1°C, blood pressure 132/77, pulse 114, and respiratory rate 17 with 100% O2 saturation on room air. On examination, he was in no distress and was noted to have a catheterizable stoma over his right lower quadrant as well as an ∼1 cm wide skin defect toward the left lower quadrant (Fig. 1). There was copious malodorous, purulent material draining from the skin defect, further expressible with cutaneous pressure. The surrounding skin was erythematous, indurated, and tender to palpation without any crepitance.

Examination revealing lower abdominal skin defect with purulent drainage. Stoma is cannulated with an 8F feeding tube to bulb suction.
Diagnosis
Laboratories obtained in the ED included a comprehensive metabolic panel, which revealed hypochloremia of 90 mmol/L and an elevated creatinine of 5.1 mg/dL. Complete blood count consisted of a leukocytosis with white blood cell count 15.4 and a leftward neutrophil shift of 82% as well as anemia with hemoglobin of 11.5. Urinalysis was obtained and concerning for infection due to findings of pyuria of 154 white blood cells/high power field with many bacteria seen as well as microscopic hematuria of 159 red blood cells/high power field. Urinary pH was 6.0.
A CT scan of the abdomen and pelvis was performed with IV contrast that revealed a distended, thickened urinary diversion containing multiple calcifications consistent with stones (Fig. 2). There was severe hydroureteronephrosis with thinned renal cortices. A 3 × 1 cc fluid collection was noted in the lower anterior abdominal tissue that appeared to be in continuity with the skin and the urinary diversion (Fig. 2, right).
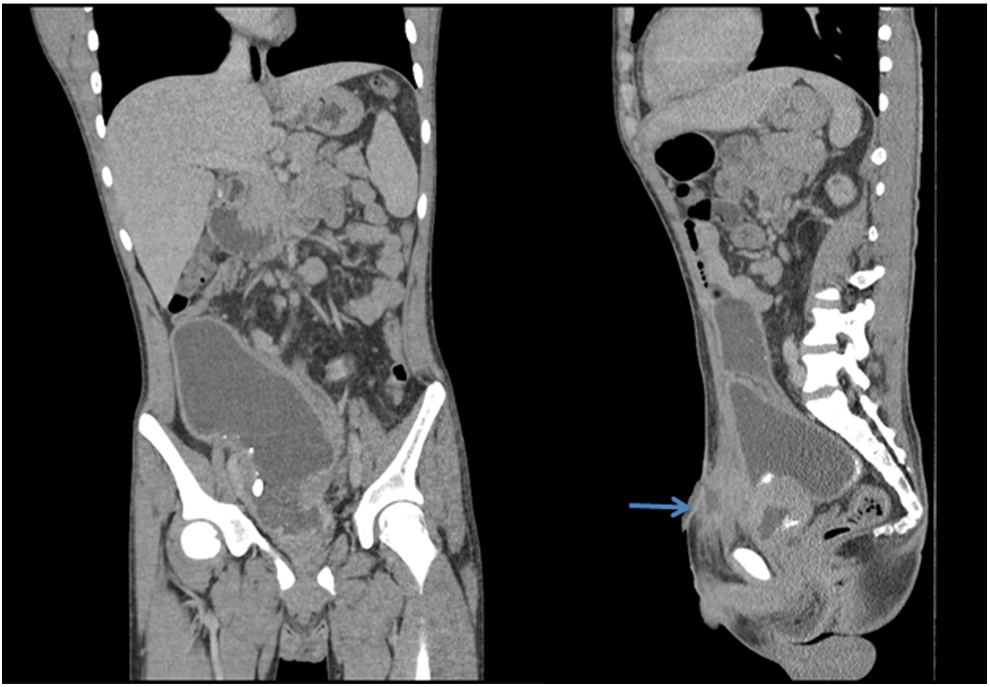
CT imaging with coronal view (left) showing a distended urinary diversion with calcifications. Sagittal view (right) with lower abdominal fluid collection (arrow) in close vicinity to the diversion.
Intervention
Given the findings of the distended diversion and likely fistulous connection, attempts were made to place a catheter into his stoma for drainage. Unfortunately, there was significant difficulty with passage of a catheter and only an 8F feeding tube was effectively passed into the diversion and subsequently placed to suction drainage. He was started on piperacillin/tazobactam and underwent bilateral nephrostomy tube placement for urinary diversion and determination of his true daily urinary output, given his end-stage renal disease status.
The patient was then taken to the operating room for irrigation of his urinary diversion. An O'Brien suprapubic access set was used to gain access into the urinary diversion and the tract was then serially dilated to 24F using the Amplatz renal dilator set. A rigid nephroscope was advanced into the tract and the pouch was thoroughly irrigated. There was drainage of irrigation fluid through the skin defect, confirming the presence of a fistula. Within the diversion, there was extensive purulent debris lining the walls as well as several stones that were removed (Fig. 3). An indwelling 22F three-way Foley catheter was placed within the access site into the pouch and the bilateral nephrostomy tubes were left to gravity drainage.
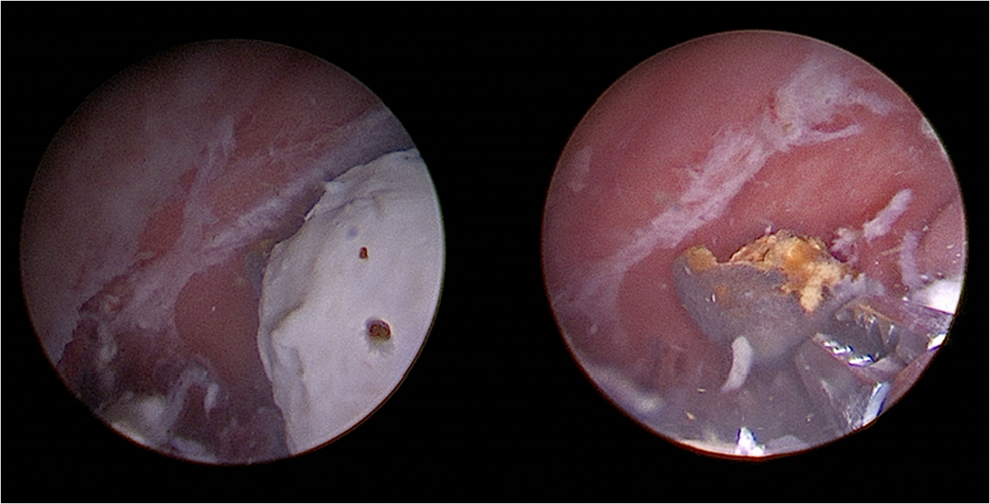
Endoscopic view of the diversion with purulent debris and pouch calculi.
Follow-Up/Outcome
The patient was admitted for postoperative care and antibiotics. Cultures resulted in two different colonies of Pseudomonas aeruginosa and two different colonies of Escherichia coli. Stone analysis revealed 100% carbonate apatite (dahllite). He was converted to oral antibiotics without issues and was discharged. At outpatient follow-up, the patient was instructed on proper care of his pouch and need for daily irrigation. Long-term options were also discussed with the patient regarding possible native nephrectomy and removal of his diversion given his dialysis dependence and undocumented, uninsured status, preventing future kidney transplant. Unfortunately, the patient became lost to follow-up shortly after his postoperative visit.
Discussion
The first continent urinary diversions were first described between 1890 and 1920, with Gilchrist being the first to describe the effective use of an ileocecal segment for urinary diversion in 1950. 1 Since then, the use of continent urinary diversions after cystectomy has increased, with some providers championing for the use of orthotopic urinary diversions as the new gold standard. 2 Advantages of continent diversions over ileal conduit have been described in the literature, primarily revolving around possibly increased quality of life 3 and continence, with continence rates ranging from 72% to 98%.1,4 However, many studies in the literature have failed to demonstrate any statistically significant difference in quality of life between incontinent urinary diversion and continent diversion, 1 with most patients stating that they would choose the same method of diversion again if given the choice. 3
Contraindications for continent diversions include compromised renal function, severe hepatic dysfunction, impaired intestinal function, urethral disease for those patients undergoing orthotopic diversions, and inability to self-catheterize or care for oneself. Complications of continent urinary diversions have been previously described in the literature as including metabolic complications dependent on the type of bowel incorporated, mucus retention possibly leading to urinary retention, and pouch calculi. 1 Difficulty catheterizing, as demonstrated in this patient, can be caused by complications such as stomal stenosis, false passage, and channel stricture at rates up to 40%, the majority of which occurring within the first 2 years of surgery.5,6 This is in addition to the not insignificant late complication rate of 11% to 37%. 7
To our knowledge, this is the first description in the literature of a fistulous tract resulting from a poorly maintained urinary diversion. Patients selected to undergo continent urinary diversions must be able and willing to perform the meticulous care needed to maintain their pouches to avoid complications, both immediate and years down the line.1,5 This patient underwent a continent urinary diversion as a child in the United States despite the obstacles to care, given his undocumented and uninsured status. Although he is willing and able to self catheterize, he is unfortunately without the necessary resources required for routine follow-up and was lost again to follow-up shortly after his first postoperative visit. Given his circumstances, a continent urinary diversion may not have been the best option for urinary management, especially given the literature suggesting similar quality of life with an incontinent urinary diversion. This case highlights the complications that can arise from a continent urinary diversion as well as the need for strict patient selection for such diversions and the importance of urologic follow-up.
Footnotes
Author Disclosure Statement
No competing financial interests exist.