
Abstract
The possibility of bilateral adrenal gland metastasis from renal cell carcinoma (RCC) has been extremely rarely reported. Surgery may be the preferred treatment strategy for adrenal metastasis from RCC. In this article, we present a patient with bilateral large adrenal metastases from the left RCC, which was managed with simultaneous bilateral laparoscopic excision. A 64-year-old woman had undergone left adrenal sparing radical nephrectomy for a left RCC 7 years ago. Her abdominal CT scan revealed bilateral large adrenal metastasis. She underwent bilateral laparoscopic adrenalectomy. The operation was uneventful and the patient was discharged after 4 days with no complications. Bilateral laparoscopic adrenalectomy for adrenal metastasis seems to be a feasible and safe procedure in such cases, but this needs to be confirmed by further studies with a larger sample size.
Introduction
Renal cell carcinoma (RCC) represents ∼3% of all types of cancer worldwide, and accounts for 90% to 95% of malignancies involving the kidneys. 1 Although, RCC metastasis can develop in every organ, the most common sites for distant metastasis are the lungs, liver, bones, and brain. 2 The risk of adrenal metastasis is low; consequently, most patients undergo adrenal sparing radical nephrectomy. The incidence of ipsilateral metastasis in the adrenal gland has been reported to be 3%–5%, whereas the rate of contralateral metastasis is 0.7%. The possibility of synchronous bilateral adrenal gland metastasis has been recorded as extremely rare (<0.5%).3–5 Nevertheless, surgical resection of metastases from RCC remains the only therapeutic option in patients with a solitary site or low-volume metastasis. Therefore, surgery may be the preferred treatment strategy for adrenal metastasis from RCC. 6 In this article, we present a patient with bilateral large adrenal metastases from the left RCC, which was managed with simultaneous bilateral laparoscopic excision.
Case Report
A 64-year-old Iranian woman was referred to our clinic; she had undergone left adrenal sparing radical nephrectomy for a left RCC, 7 years before. Microscopic histopathologic study showed a clear cell type of RCC. Abdominal CT scan revealed a right adrenal mass measuring 41 × 33 mm. In addition, two other masses measuring 40 × 33 and 30 × 24 mm were detected in the left adrenal (Fig. 1). No calcification and contrast enhancement were observed in these masses.
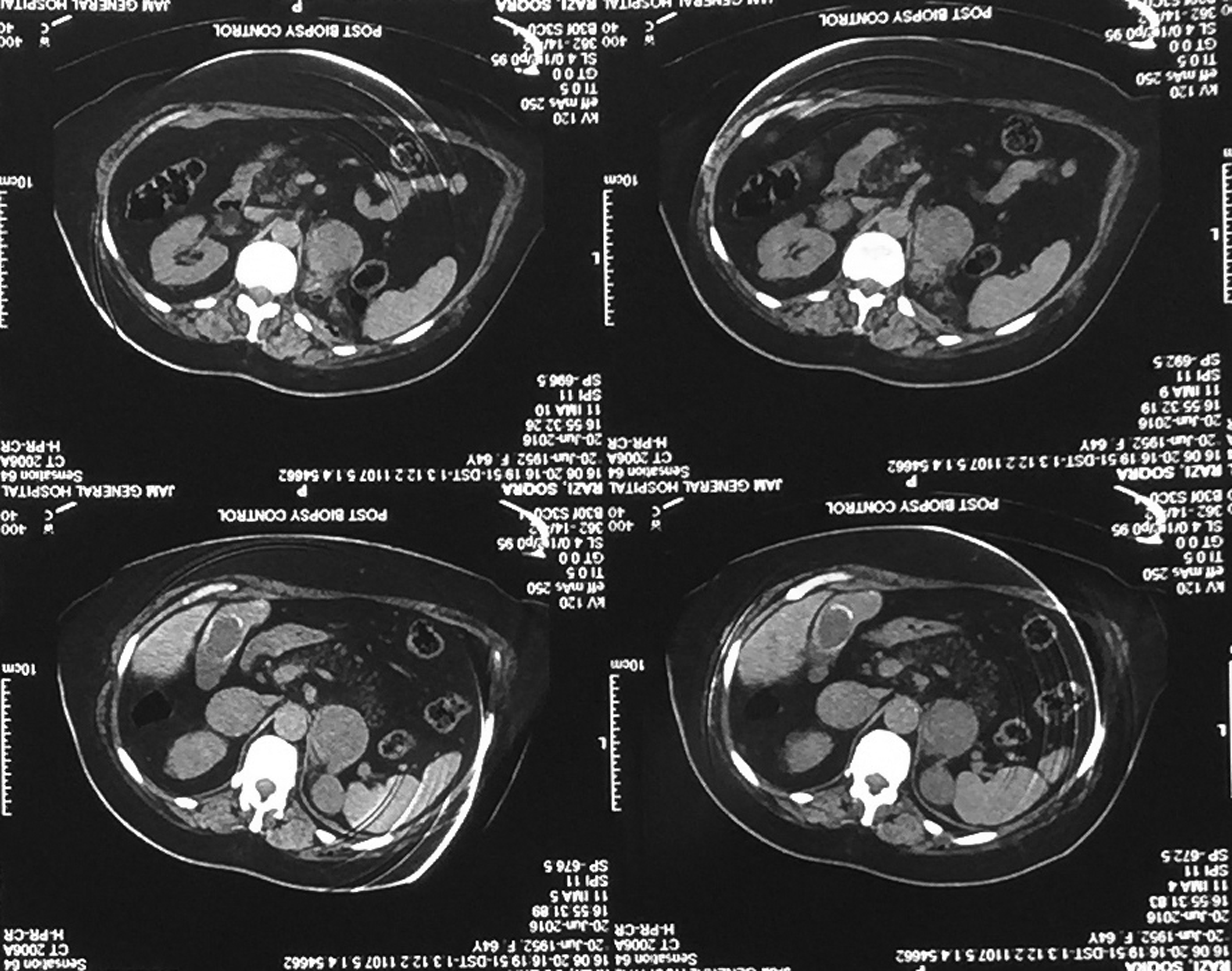
Abdominal CT-identified bilateral adrenal masses.
The patient was admitted for further investigation. On physical examination, the patient had normal blood pressure and no other abnormalities were noted. The results of laboratory studies, including blood cells count, blood chemistry, and electrolytes, were within normal limits. Hormonal examination, including adrenocorticotropic hormone, serum catecholamines, cortisol, aldosterone, 24-hour urinary excretion of metanephrines and vanillylmandelic acid, and plasma renin activities were all within normal limits. Left adrenal CT-guided needle biopsy was then performed and the histopathologic assessment of the biopsy sample revealed RCC metastasis.
She underwent bilateral laparoscopic adrenalectomy. Laparoscopy was done by the transperitoneal lateral decubitus approach, as it best exposes the gland and vessels. We used the Hasson technique to create pneumoperitoneum and the operation was done by four working trocars.
For the left side, it was necessary to mobilize the colon and tail of the pancreas. After dividing the splenocolic ligament and opening the Gerota fascia, the adrenal tumor was adequately exposed. The adrenal mass was reflected medially and the adrenal vein was clipped and divided. After extraction of the left adrenal gland, the right adrenal gland was excised effectively with the same approach (Fig. 2). The operation was uneventful and the patient was discharged after 4 days with no complications. Microscopic histopathology showed bilateral adrenal metastases of RCC.

Bilateral adrenal glands were extracted.
Discussion
Synchronous ipsilateral adrenalectomy is not routinely recommended in radical nephrectomy as the risk of ipsilateral adrenal gland involvement is around 2%. 4 Furthermore, adrenal gland metastasis may be discovered many years after radical nephrectomy. 2 The mean time required to develop a metastasis from a RCC to the contralateral adrenal gland has been identified as 52.3 months after radical nephrectomy. 4 The incidence of ipsilateral, contralateral, and bilateral adrenal metastasis from RCC are 1.9%, 1.5%, and 0.3%, respectively. 7
Given all that, certain problems have to be overcome in the diagnosis of adrenal metastasis. First, the clinical signs and symptoms of adrenal metastasis are rare. Nowadays, patients' follow-up with routine noninvasive radiologic techniques, such as CT, have improved the detection of adrenal metastatic lesions. In some patients, failure to use routine imaging studies in the follow-up period might result in delayed diagnosis. Second, the distinction between metastatic lesions, primary adrenal malignancy, and adrenal adenoma may be problematic. The history of RCC, radiologic findings and normal hormonal assessment could be suggestive of a metastatic lesion involving the adrenal. In doubtful cases, needle biopsy may be helpful in the diagnosis, but the definite diagnosis is often made only by the histopathologic study following adrenalectomy. 8
To date, various therapeutic modalities, including chemotherapy, hormonal therapy, and radiotherapy have failed to markedly improve survival in metastatic cases. Previous studies have shown that adrenalectomy with the aim of removing metastatic lesions may prolong survival in patients with adrenal metastasis. 8 After adrenalectomy, the 3-year survival rate increases from 35% to 60%, while the 5-year survival increases from 14% to 38%. 2
Reoperation for open adrenalectomy after ipsilateral nephrectomy has been associated with some difficulties and a high rate of surgical complications. Abel et al. reported minimal morbidity and complications in eight patients having undergone laparoscopic adrenalectomy. 6 In addition, laparoscopic adrenalectomy has some advantages such as rapid recovery time, less pain, better cosmetic results, lower percentage of incisional hernia, and rapid return to possible systemic therapy for metastatic diseases. 2
Therefore, laparoscopic adrenalectomy is the preferred treatment for adrenal gland metastasis in RCC patients; however, experience with simultaneous laparoscopic bilateral adrenalectomy is limited. Some articles have reported simultaneous laparoscopic bilateral adrenalectomy for patients with bilateral adrenal disease. Takata et al. 9 reported their results on simultaneous laparoscopic bilateral adrenalectomy in 30 patients with Cushing's disease and bilateral pheochromocytoma. They concluded that this procedure is safe and feasible. Kawasaki et al. 10 also published their findings on 21 patients who underwent bilateral laparoscopic adrenalectomy for Cushing's disease, bilateral pheochromocytoma, aldosterone-producing adenoma, and bilateral metastasis of RCC. They reported a small number of minor perioperative complications, which proved the safety and efficacy of this procedure. In another report, Castillo et al. 11 performed simultaneous laparoscopic bilateral adrenalectomy in 20 patients with bilateral pheochromocytoma, Cushing's disease, metastasis, congenital adrenal hyperplasia, hyperaldosteronism, adrenal adenoma, and myelolipoma. In their report, the sources of metastasis were lung cancer, melanoma, and lymphoma. Hasan et al. 12 also reported the outcome of simultaneous laparoscopic bilateral adrenalectomy in seven patients with bilateral pheochromocytoma, Cushing's disease, and metastasis from lung cancer.
To the authors' knowledge, Kawasaki reported the first case of laparoscopic bilateral adrenalectomy for RCC metastasis, and therefore, the available literature on this procedure in RCC metastasis is limited.
Although the present study is a case report which is normally classified as low level evidence, yet, it shows that bilateral laparoscopic adrenalectomy for adrenal metastasis is a feasible approach. Some reports have stated that the laparoscopic approach is associated with a low rate of intra- and postoperative complications, while preserving the principles of oncologic outcomes.10,11 Other studies have reported a higher complication rate in bilateral laparoscopic adrenalectomy compared with unilateral laparoscopic adrenalectomy; however, in the laparoscopic approach compared with the open one, there are less surgical complications and intraoperative risks. 13 Moreover, extensive experience is required in advanced laparoscopic surgeries to perform a laparoscopic excision on malignant adrenal tumors and metastasis.
In conclusion, we presented a case of bilateral adrenal metastasis from left RCC, occurring 7 years after radical adrenal sparing nephrectomy. Laparoscopic bilateral adrenalectomy was effectively performed with no complications; yet, this approach needs to be confirmed by future studies and more cases.
Footnotes
Disclosure Statement
No competing financial interests exist.