
Abstract
Abstract
Background:
Nephron-sparing surgery has been shown to achieve oncological results equivalent to those of radical nephrectomy in patients with compromised renal function who have renal tumors <4 cm. However, technical difficulties and potential surgical complications remain challenges to the surgeon. Various factors, such as tumor size and location, collecting system invasion, and patient's expectations, are major concerns that may affect the feasibility of performing an effective partial nephrectomy. We report a patient with renal cell carcinoma who underwent open partial nephrectomy and suffered from complications of perirenal abscess because of stone migration, obstruction, and subsequence urine leakage.
Case Presentation:
A 63-year-old female with an incidental finding of a 4-cm renal tumor on the left kidney underwent an effective open partial nephrectomy at our institute. There were no intraoperative complications and the drainage tube was removed 3 days later. The patient visited our emergency department 1 month later with high fever. She was diagnosed with severe sepsis and perirenal abscess formation. Percutaneous nephrostomy was performed for prompt decompression. A sequential imaging study with CT and antegrade pyelography revealed one 0.5-cm stone, which migrated from the calix to proximal ureter postoperatively and subsequently caused obstruction and dramatic urine leakage. Ureteroscopic lithotripsy was performed with ureteral stenting. Postoperatively, the urinary leakage and abscess formation resolved.
Conclusion:
Nephron-sparing surgery is one of the most challenging procedures in the management of renal cancer. Urine leakage after partial nephrectomy may occur when a large tumor involves the collecting system. Postoperative ureteral obstruction is also a risk factor of urinary leakage. Watertight repair with a Double J catheter before operation may be required.
Introduction
Nephron-sparing surgery has been shown to achieve oncologic results equivalent to those of radical nephrectomy in patients with compromised renal function who have renal tumors <4 cm. 1 However, technical difficulties and potential surgical complications remain challenges to the surgeon. Various factors, such as tumor size and location, collecting system invasion, and patient's expectations, are major concerns that may affect the feasibility of performing an effective partial nephrectomy. 1
Urine leakage is a frustrating complication after partial nephrectomy, and the incident ranges from 0.5% to 21%. 2 Urine leakage may be detected as persistent drainage output after operation and may be the consequence of large tumor size or repair of the collecting system. 3 In most situations, the condition resolves spontaneously. However, when the symptoms become worse, ureteral stent or percutaneous nephrostomy may be required to relieve the leakage and possible healing of the renal pelvis. 3
We report a patient with renal cell carcinoma who underwent open partial nephrectomy and suffered from complications of perirenal abscess because of stone migration, obstruction, and subsequent urine leakage.
Case Report
A 63-year-old female with an incidental finding of a 4-cm renal tumor on the left kidney underwent an effective open partial nephrectomy at our institute. She previously had no systemic diseases, such as diabetes mellitus. There were no intraoperative complications, and the drainage tube was removed 3 days later. The patient visited our emergency department 1 month later with high fever. She was found to have severe sepsis and perirenal abscess formation. Percutaneous nephrostomy was performed for prompt decompression. A sequential imaging study with CT and antegrade pyelography revealed one 0.5-cm stone, which migrated from the calix to proximal ureter postoperatively and subsequently caused obstruction and dramatic urine leakage. Ureteroscopic lithotripsy was performed with ureteral stenting. The urinary leakage and abscess formation resolved postoperatively.
Our case report involves a previously healthy 63-year-old female patient without any systemic disease. She initially presented with right flank pain because of a ureteral stone, and an ∼4-cm renal tumor of the left kidney was incidentally observed. CT revealed a contrast-enhanced left renal tumor 4.3 cm in length, middle portion, posterior aspect, 50% endophytic, and close to the collecting system (Fig. 1). In addition, one 0.5-cm stone located at the left upper calix was also noted (Fig. 2). Conventional renal cell carcinoma of the left kidney was diagnosed, and she underwent an effective open partial nephrectomy on November 2014.
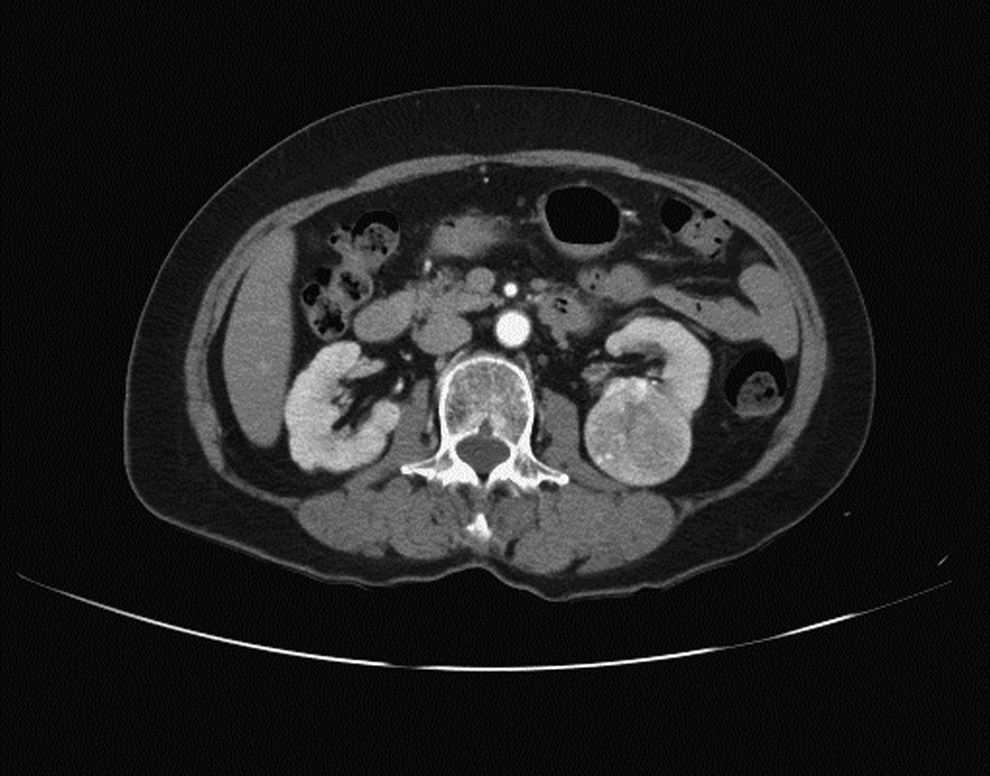
Incidentally found contrast enhancement of solid tumor or left kidney. Contrast enhancement of left renal tumor of 4.3 cm in length, middle portion, posterior aspect, 50% endophytic, and near collecting system.
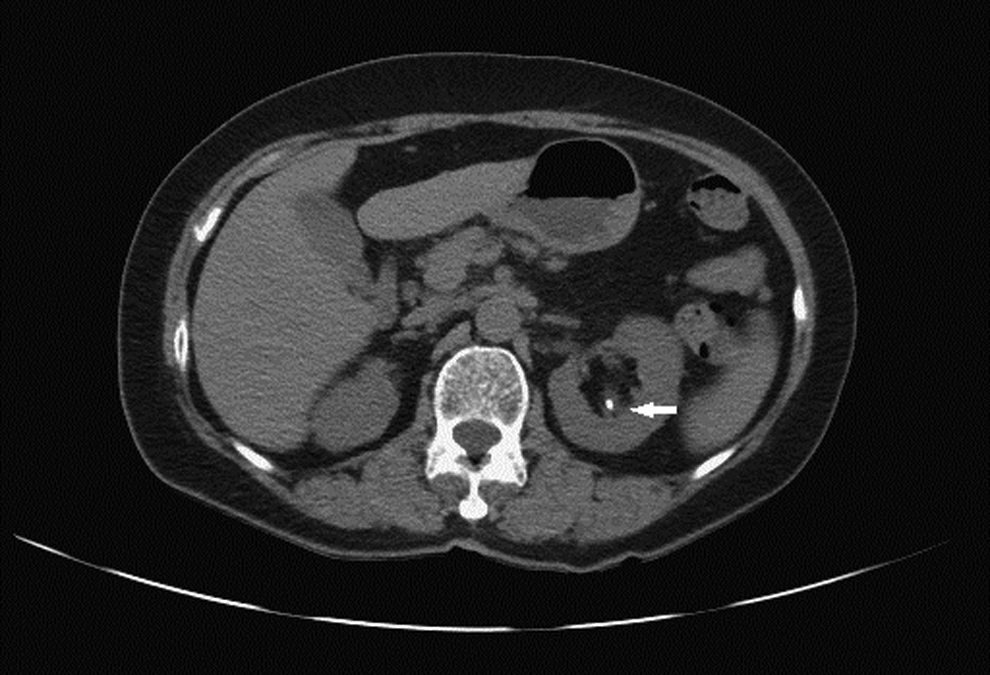
In precontrast phase, one 0.5 cm upper calix stone was found. One 0.5 cm intracollecting system stone at left upper calix (arrow).
The operation was performed through flank incision alone at the upper margin of the left 11th rib. During the operation, one well-capsulated tumor arising from the posterior lower pole of the kidney and protruding into the renal hilum was observed. After pedicle dissection and tumor location, the renal artery and vein were controlled with bulldog clamps, and the kidney was under surface cooling with ice for 10 minutes. The tumor was excised through the capsule to the sinus fat, and the defect of the central calix was repaired with absorbable suture materials. The bleeding parenchyma surface of the low pole defect was cut, sutured with continuous 3–0 V-Loc for the inner cortex and 2–0 V-Loc for the outer cortex, and packed with surgical seal and fatty tissue. The bulldog clamps were released, and the entire procedure was completed in 29 minutes. The bleeding amount was estimated to be ∼150 mL.
After the operation, the drainage amounts were 150, 55, and 32 cc at postoperative days 1, 2, and 3, respectively. The drainage tube was removed with a negligible amount, and the patient was discharged from the hospital. The stitches were removed 1 week later in the outpatient department.
The patient presented at our emergency department 3 weeks later with persistent turbid discharge from the drainage hole. Based on her description, she suffered from intermittent low-grade fever during the month with left flank soreness. Physical examination confirmed left flank tenderness and erythematous in the incision wound. Some yellowish pus-like discharge from the drainage wound suggested abscess formation. CT was immediately performed that revealed multilobular abscesses around the left kidney, mainly in posterior peri- and pararenal spaces (Fig. 3). Mild hydroureter was noted at the ureteropelvic junction, and the stone that was previously located at the upper calix had vanished. Two percutaneous drainage tubes were placed at lateral and posterior aspects of the abscess, and the patient was admitted with intravenous antibiotics for infection control. Fluid from drainage tube was examined that revealed an increase in creatinine and potassium, suggesting urine leakage.
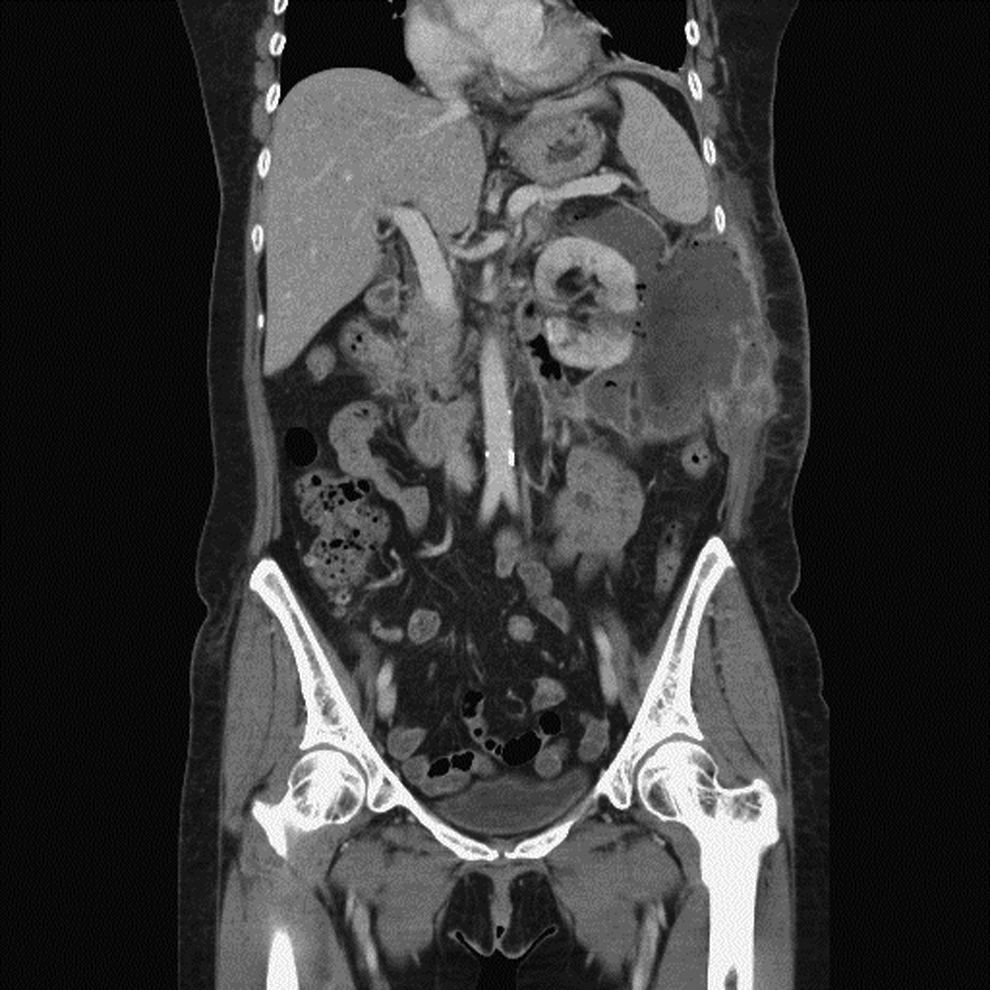
Patient went to emergency department with fever, chillness, left flank pain, and turbid discharge from previous drainage hole. CT revealed multilocular abscesses formation around left kidney, mainly in posterior peri- and pararenal spaces.
Three days later, the patient's fever subsided and discharge diminished. Ureteroscopy was performed with a Double J stent and retrograde pyelography. While under endoscopic examination, one ureteral stone that measured ∼0.5 cm was found at the middle third ureter, and lithotripsy was performed (Fig. 4A). A Double J catheter was also inserted for diversion for 1 week. Later, retrograde pyelography was repeated that showed patent collecting system without filling defect or contrast extravasation (Fig. 4B).
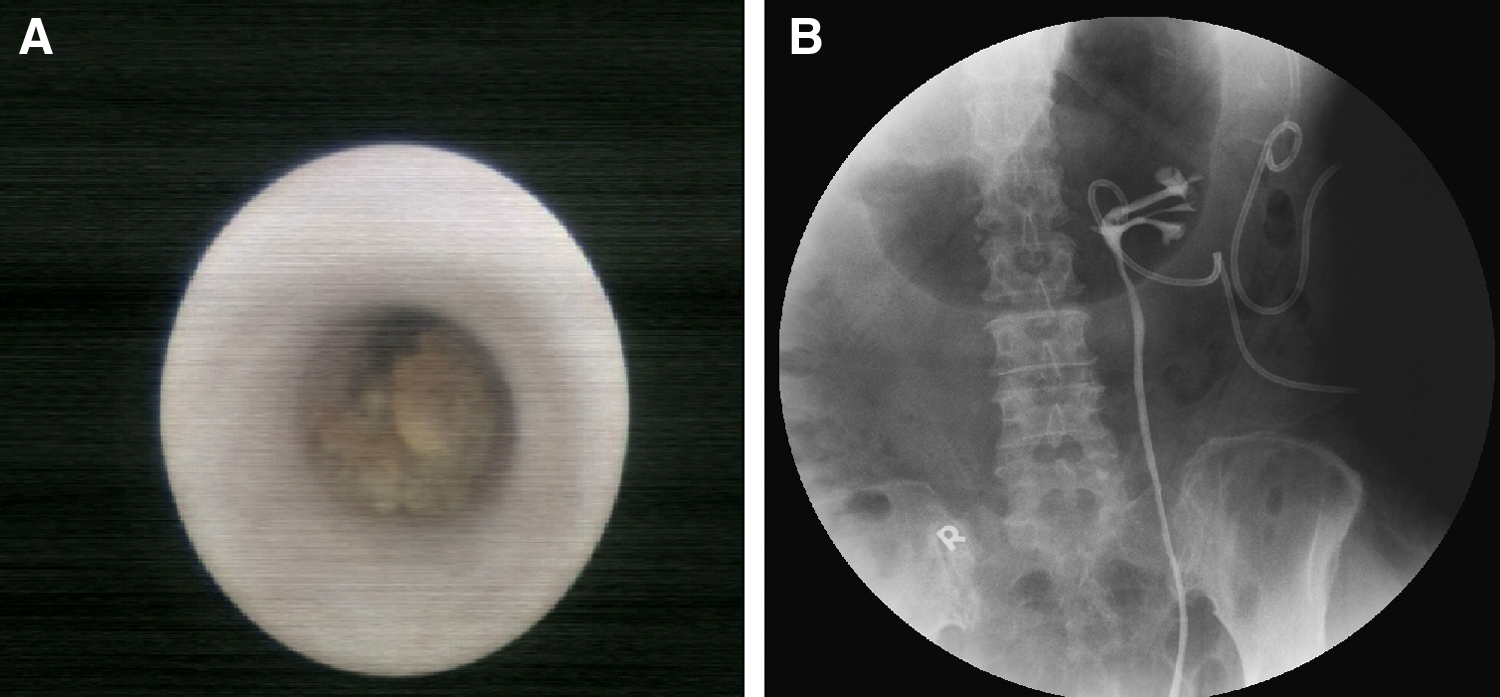
URSL and retrograde pyelography were arranged and performed 1 week later after infection control.
Full-course antibiotic treatment was completed, and the drainage tube was later removed without evidence of leakage or active infection. CT was repeated 1 month after patient discharge, and no additional lobulated abscess or urinoma was noted.
Discussion
Partial nephrectomy using an open and laparoscopic technique is increasingly used in small or select size renal tumors. The size, location, and complexity of tumors have also increased as surgical doctors' experience increases. 1 Previously, most studies about partial nephrectomy focused on oncology control, and few studies focused on complications, such as urine leakage.
Meeks et al. retrospectively reviewed 127 patients who underwent partial nephrectomy to identify risk factors associated with urine leakage and management strategies after partial nephrectomy. 3 According to their results, the major risks of urine leakage include tumor size, an endophytic mass location, and tumor resection requiring collecting system repair. Moreover, Zorn et al. reported that larger tumor size, specimen weight, and endophytic lesion correlated with increased ischemic time, perioperative bleeding, postoperative bleeding, and urine leakage rate. 4
Initial management followed by urine leakage after partial nephrectomy involves drainage manipulation, such as placement of a Foley catheter and ureteral stent. In a study by Simmons and Gill, a small series of patients received partial nephrectomy effectively managed by 30 to 45 days of ureteral stent placement. 2 The placement of a ureteral stent could provide a path with less resistance for urine to drain, thus making the collecting system an opportunity for reconstruction and healing.
In this case, the operation was performed by an experienced operator and surgical team that specialized in not only open partial nephrectomy but also laparoscope and robot-assisted partial nephrectomy. We focused on tumor size, behavior, location, and possibility of invasion of sinus fat, and the relative small size upper calix stone was not a factor. The drainage tube was removed under reasonable conditions, but the patient presented at our department with a disastrous result. Initial management with a percutaneous drainage tube for decompression and infection control is indicated. We sought to determine the cause of the disastrous result, and ureteroscopic findings provided the answer. Fortunately, after lithotripsy, retrograde pyelography revealed no sustained leakage, and the patient was discharged 1 week later.
We received considerable information from this study. First, although the stone is small, it can migrate after kidney manipulation and lead to severe obstruction. The need for a prior Double J stent may be considered. Second, stone management before operation may be controversial. For the reported renal stone, possible management may include extracorporeal shock wave lithotripsy or flexible ureteroscopic lithotripsy. This procedure may be associated with a risk of hematoma or tumor rupture, which may make the operation more difficult.
Nephron-sparing surgery is one of the most challenging procedures in the management of renal cancer. Urine leakage after partial nephrectomy may occur when a large tumor is removed that involves the collecting system. Postoperative ureteral obstruction is also a risk factor of urinary leakage. Watertight repair with a Double J catheter before operation may be required.
Footnotes
Disclosure Statement
No competing financial interests exist.