
Abstract
Abstract
Background:
Initial management of urethral injury remains controversial concerning the use of suprapubic urinary diversion and delayed repair, primary open realignment, and primary endoscopic realignment. To our knowledge, we present the first reported case of a penetrating urethral injury because of an animal attack, without concomitant extragenitourinary system involvement, managed entirely endoscopically.
Case Presentation:
This is a case of an 82-year-old male who presented to the emergency department after an attack by a semidomesticated deer. He presented with a penetrating scrotal injury and gross blood at the meatus. A retrograde urethrogram was performed that revealed a urethral injury. Surgical exploration revealed an isolated 3-cm urethral defect. It was managed with primary endoscopic placement of a urethral catheter and suprapubic tube.
Conclusion:
Although initial management of urethral injuries remains controversial, an isolated urethral injury after a penetrating trauma because of an animal attack may be safely and effectively managed by primary endoscopic realignment.
Introduction and Background
Trauma is a world-wide health concern, and remains the number one cause of death in the 1 to 37-year age group. Approximately 10% of patients sustaining a traumatic injury have some form of genitourinary involvement. Most posterior urethral injuries are caused by pelvic fractures, whereas anterior urethral injuries may be caused by straddle injuries, penetrating trauma, etc. Presence of a urethral injury should be suspected based on the mechanism of injury, blood at the urethral meatus, or inability to void after the traumatic event. Diagnosis is made with retrograde urethrography. Initial emergent treatment remains controversial, but mainstays of therapy include drainage of the urinary bladder, often with placement of a suprapubic catheter (SPT) and primary endoscopic realignment of the urethra if possible. Our review of the literature reveals only one case of a penetrating urethral injury because of animal attack, and this case involved significant injuries to surrounding organ systems (bowel primarily). To our knowledge, we present the first reported case of a penetrating urethral injury because of animal attack, without concomitant extragenitourinary system involvement, managed entirely endoscopically.
Presentation of Case
We present an 82-year-old Hispanic male, who presented to our level one trauma center by ambulance after being attacked by a semidomesticated deer on his ranch property (Fig. 1). His initial evaluation by the emergency department included standard primary and secondary survey, which revealed only a 2.5 cm puncture wound to the anterior scrotal wall and blood at the urethral meatus. Testicular examination was normal grossly. Physical examination was otherwise normal without evidence of other abnormalities. His laboratory studies, which included a complete blood count, basic metabolic panel, and coagulation studies, were all within normal limits. He had no other pertinent medical history. The emergency department performed a retrograde urethrogram (Fig. 2), which revealed a significant urethral injury. Urology was notified, and we took the patient emergently to the operating room for scrotal exploration and management of his urethral injury. Scrotal exploration revealed no testicular injury, but a 3 cm laceration to the ventral urethra was noted. We were able to traverse this injury with a flexible cystoscope. No bladder abnormalities were noted. An SPT was placed under direct vision with the cystoscope in the bladder, and then a Council catheter was placed over a wire that had been deployed through the cystoscope. Given the contaminated, penetrating mechanism of his injury, we decided not to attempt primary repair of his urethral laceration, and we only loosely approximated the skin of his scrotal incision. A Penrose drain was also placed through the dependent scrotal wall to aid in drainage of the wound, and he was given empiric trimethoprim/sulfamethoxazole for further infection prophylaxis. The patient was discharged home the following day. There were no postoperative complications noted.

Patient and semidomesticated deer.

Retrograde urethrogram.
The patient subsequently returned to the clinic for drain removal on postop day 6. Voiding cystourethrogram (VCUG) on postop day 26 (Fig. 3), revealed a small bulbar urethral diverticulum filling with contrast, but no other extravasation was noted. His urethral catheter was not replaced, and SPT drainage was continued for another 8 weeks, with SPT changed at 4-week intervals. At 8 weeks, an office cystoscopy was performed with his urethra found to be completely healed and epithelialized, to include the small diverticulum previously noted on VCUG (Fig. 4). His SPT was removed and he was discharged home, voiding normally per urethra. He has continued to do well since that time.
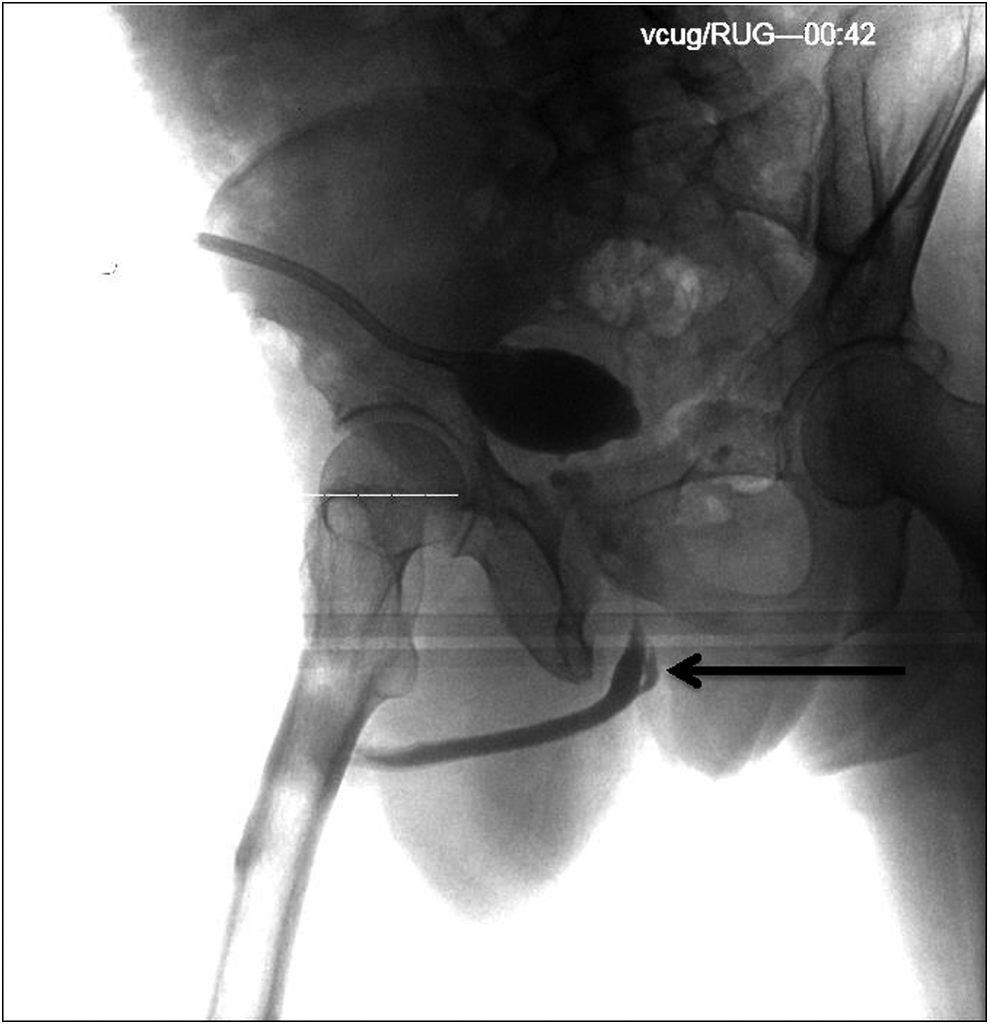
Voiding cystourethrogram, with urethral diverticulum (arrow).
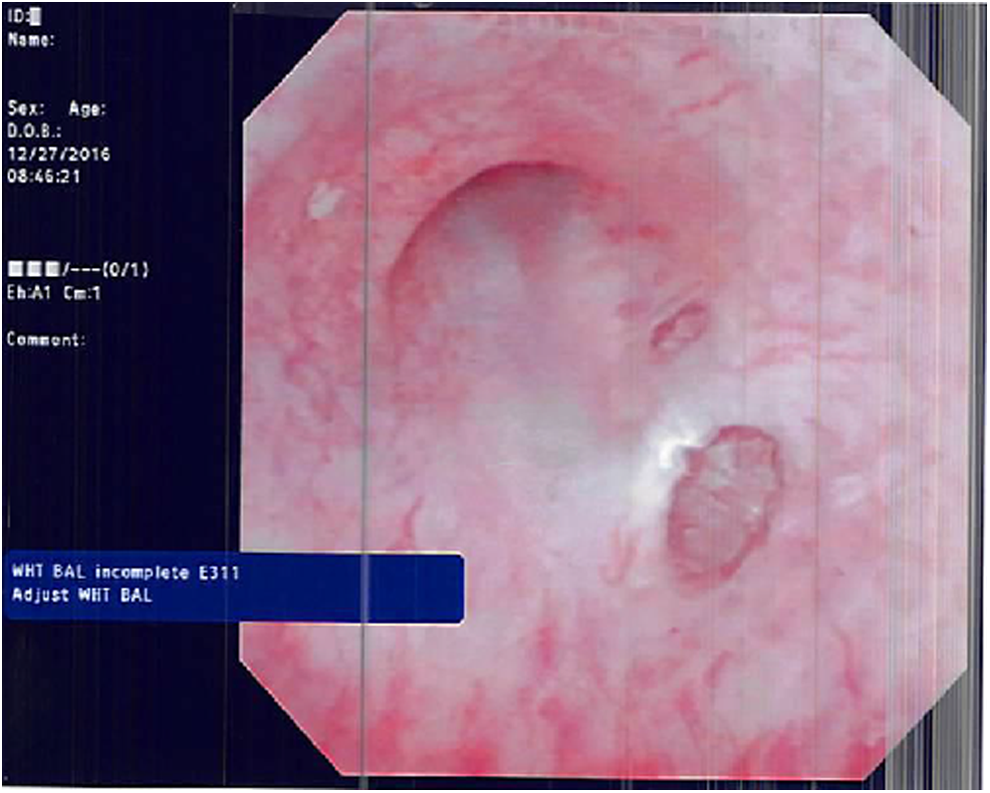
Cystoscopy findings.
Discussion and Literature Review
Urethral injuries are relatively uncommon and are often associated with significant comorbid injuries, including pelvic fractures or involvement of external genitalia. Early identification of urethral injury is essential based on the mechanism of injury and presenting symptoms, including blood at the meatus or difficulty urinating after a traumatic injury. 1 Initial management of incomplete urethral injuries remains controversial but options include suprapubic urinary diversion with delayed urethral management, primary open repair, and primary endoscopic realignment over a catheter. Long-term complications from primary endoscopic realignment include urethral strictures, incontinence, and impotence with reported rates varying from 48% to 68%, 3.7% to 5.8%, and 20% to 21%, respectively. 1 Primary endoscopic management of urethral injuries may be associated with more surgical interventions and a prolonged clinical course because of delayed presentation of urethral strictures compared with urethral injuries managed primarily with suprapubic diversion. 2 Conversely, primary realignment has a lower risk of immediate complications and may lead to more favorable surgical candidates for those who do develop urethral strictures requiring urethroplasty. 3
The majority of available data regarding initial management come from urethral injuries associated with pelvic fractures or high-velocity penetrating injuries and there are few reports of isolated urethral injuries. Long-term complications after urethral injury is likely multifactorial and are related to the mechanism of injury, comorbid traumatic injuries, and initial management. For isolated urethral injuries, endoscopic urethral realignment may have minimal effect on impotence or incontinence because of lack of manipulation of surrounding neurovascular bundles.
Our patient presented after a penetrating injury from an animal attack with an isolated partial urethral disruption. There are few reported isolated urethral traumas and only one identified as a result of an animal attack. In this case, there were several comorbid injuries, including a urethrorectal fistula after a bull horn injury in which the urethral injury was initially managed with suprapubic urinary diversion and subsequent endoscopic management. 4 Our case, to our knowledge, is the first reported case of an isolated urethral disruption after an animal attack that was managed effectively by primary endoscopic realignment. Although long-term follow-up remains to be seen, he is currently voiding at baseline and is catheter free without any further endoscopic or open surgical management. In trauma patients with low-velocity penetrating urethral injuries, and in the absence of significant concomitant extragenitourinary involvement, this may prove an effective management option that may be associated with less surgical morbidity, fewer surgical interventions, and shorter time to regained urinary function. Based on our experience with this single patient, we cannot extrapolate outcomes to higher velocity injuries, or injuries that involve other pelvic organs, such as the bowel. In that patient population, open surgical management may provide better outcomes.
Conclusion
Although initial management of urethral injuries remains controversial, many options for primary treatment are available and each has associated risks for long-term complications. Many urethral injuries are associated with comorbid traumatic injuries that may require repeat or more extensive reconstructive surgeries. In the setting of an isolated urethral injury after a low-velocity penetrating trauma, primary endoscopic realignment may prove to be a safe and effective management option.
Footnotes
Disclosure Statement
No competing financial interests exist. The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the U.S. Army Medical Department, the U.S. Army Office of the Surgeon General, The Department of the Army, the Department of the Air Force, and the Department of Defense or the U.S. Government.