
Abstract
Abstract
Background:
Schistosomiasis is rare in western countries, but remains a potentially serious disease. It is known to result in severe urogenital complications; prompt diagnosis can therefore significantly affect outcomes.
Case Presentation:
We report the case of a 41-year-old male with pleuritic chest pain and visible hematuria who had emigrated from Zimbabwe to the United Kingdom 20 years previously. CT imaging revealed a hydronephrotic right pelvicaliceal system, with a dilated ureter to its distal portion. Preliminary tests for schistosomiasis, including terminal urine microscopy and serology, were negative. An initial ureteroscopy was challenging owing to a tight ureteral stricture such that a retrograde stent insertion and not ureteroscopic visualization or biopsy was carried out. A relook ureteroscopy after 6 weeks revealed a dense distal ureteral stricture, biopsies were taken, the stricture was ablated with LASER, and a retrograde stent was placed. Microscopic examination of the biopsies confirmed Schistosomiasis haematobium. Treatment consisted of a divided dose of praziquantel and a reducing dose of steroids. At a third look ureteroscopy the stricture was ablated with LASER again, and the stent was removed. Subsequent renograms indicated recurrent obstruction despite LASER treatment and a retrograde ureteral stent was replaced. The patient ultimately had a Boari flap ureteral reimplant with good results.
Conclusion:
This case illustrates the clinical challenges of diagnosing and treating ureteral schistosomiasis. It shows that all the initial tests can be negative, but where the clinical picture points toward schistosomiasis it is worth persevering and a good tissue biopsy may be the only way to verify an otherwise elusive diagnosis.
Introduction and Background
Schistosomiasis is a common and potentially serious parasitic disease. With over 230 million people infected with schistosomiasis in 78 countries, it is a global health problem. 1 Schistosoma haematobium is the most common of the schistosoma parasites to affect the urogenital tract and the only one to affect the ureter and bladder.
Over 90% of individuals infected with S. haematobium live in Africa. 1 In Europe the disease can be seen in travelers and migrants from endemic regions. Exposure to fresh water where the snails (the intermediate host) are found is necessary for the small cercariae to penetrate the skin.
The symptoms of acute schistosomiasis, as the cercariae migrate around the body, are generalized, including fever, rash, and usually an accompanying blood eosinophilia. As the worms reach full sexual maturity they come to reside in a venous plexus which, in the case of S. haematobium, is the vesical plexus adjacent to the bladder. The characteristic clinical features associated with chronic infection arise as a result of the production and excretion of the eggs (ova) from these mature adult worms. In order for the schistosomal life cycle to be completed the ova need to be excreted to infect their intermediate host (the snail). In many cases the ova will become embedded in the bladder wall or other parts of the urinary or genital tract. It is the consequence of these eggs with subsequent granulomatous inflammation that causes the pathology associated with chronic infection. The granulomas can result in ureteral obstruction, genital lesions, loss of bladder capacity, bladder neck stenosis, and ultimately bladder cancer. The adult worms can survive for several decades; however, even after the worms have died and the ova have disappeared chronic inflammation often persists. 2
This article reports a case of ureteral obstruction from schistosomiasis and highlights the challenges of diagnosing and treating schistosomiasis in these patients.
Presentation of Case
A 41-year-old male presented to the emergency department with pleuritic chest pain and painless visible hematuria. He was originally from Zimbabwe and had emigrated to the United Kingdom at the age of 20 years.
He had tested positive for HIV 13 years ago, with a nadir CD4 count at that time of 200 × 109/L. Since then he had been taking highly active antiretroviral therapy (HAART) which at presentation composed of abacavir, lamivudine, and dolutegravir.
Urinalysis showed blood 4+ and protein 2+. Blood tests revealed an elevated creatinine of 186 μmol/mL with an eGFR of 36 mL/minute/1.73 m2. Eosinophil count was normal at 0.31 × 109/L.
A CT pulmonary angiogram was carried out which excluded a pulmonary embolus, but it demonstrated the right kidney to be hydronephrotic. A subsequent noncontrast CT of the kidneys, ureter, and bladder revealed a dilated and hydronephrotic right pelvicaliceal system with a dilated right ureter traceable to the distal ureter. Contrast administered at the time of the prior CTPA could still be seen in the dilated right ureter (Fig. 1).
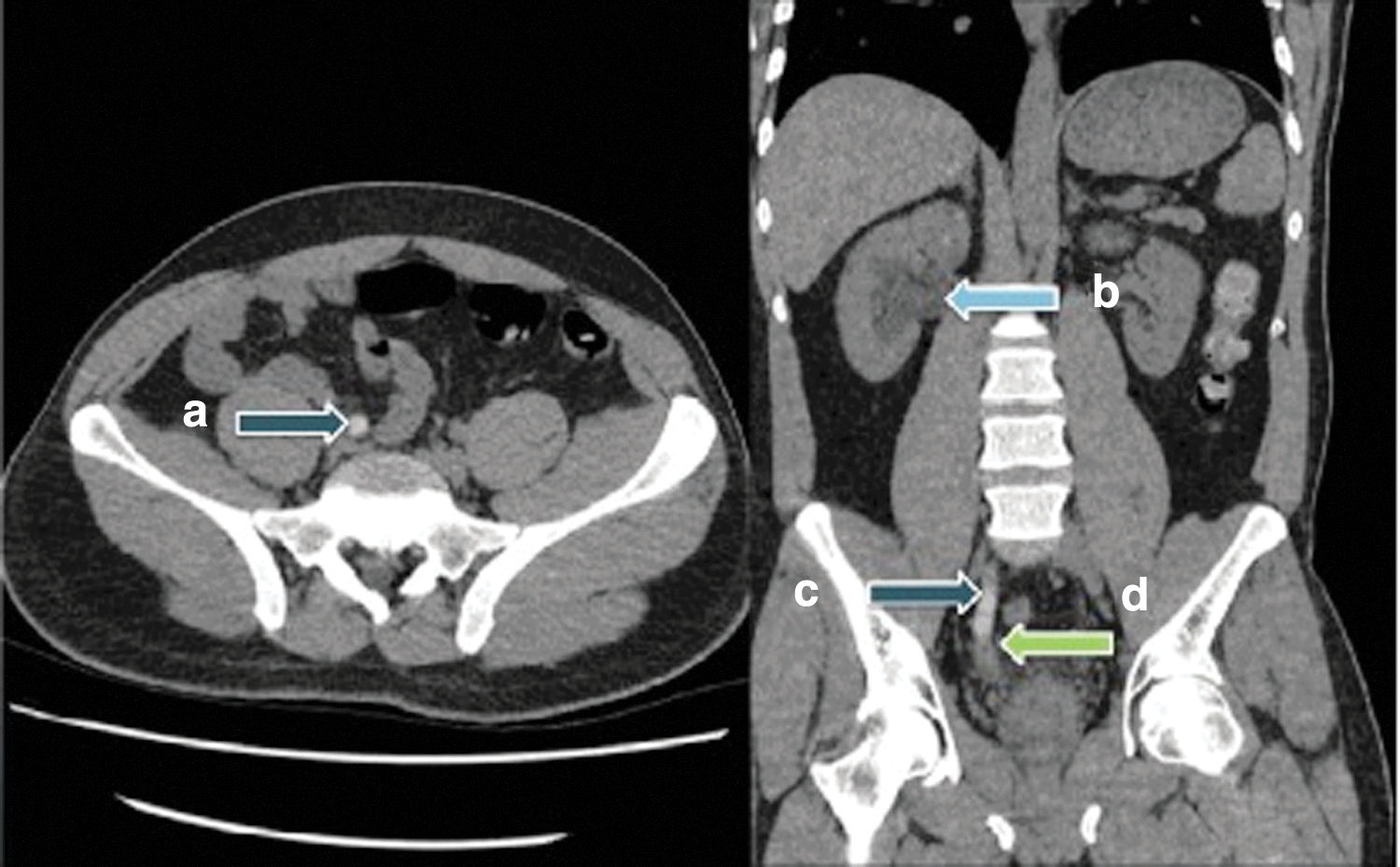
Images from noncontrast CT kidney, ureter, and bladder. Arrow points to
The differential diagnosis was consistent with delayed excretion in the context of obstruction secondary to a radiolucent distal ureteral drug stone (it was not known if there had been a history of protease inhibitor use as part of his HAART which is associated with these stones) or a distal ureteral stricture. Given his previous residential history, the possibility of schistosomiasis was raised; however, microscopy of an “end terminal urine” did not demonstrate ova, and serology for schistosomiasis was negative.
Cystoscopy revealed a tight bladder neck and red patches throughout the bladder. Retrograde pyelogram revealed a dilated right pelvicaliceal system and ureter to the distal ureter, consistent with the CT images. Ureteroscopy was challenging. The initial hydrophilic tipped (Sensor™) guidewire was positioned well in the kidney; the distal ureter was extremely tight and inserting the ureteroscope was difficult. Insertion of a second Sensor guidewire to help facilitate ureteroscopy, as is standard practice, also proved to be challenging. Retrograde studies at this point showed extravasation indicating ureteral perforation (Fig. 2). A Double-J ureteral stent was placed in the appropriate position, and a biopsy of the bladder was taken which showed an accumulation of inflammatory cells, but no diagnostic pathology.
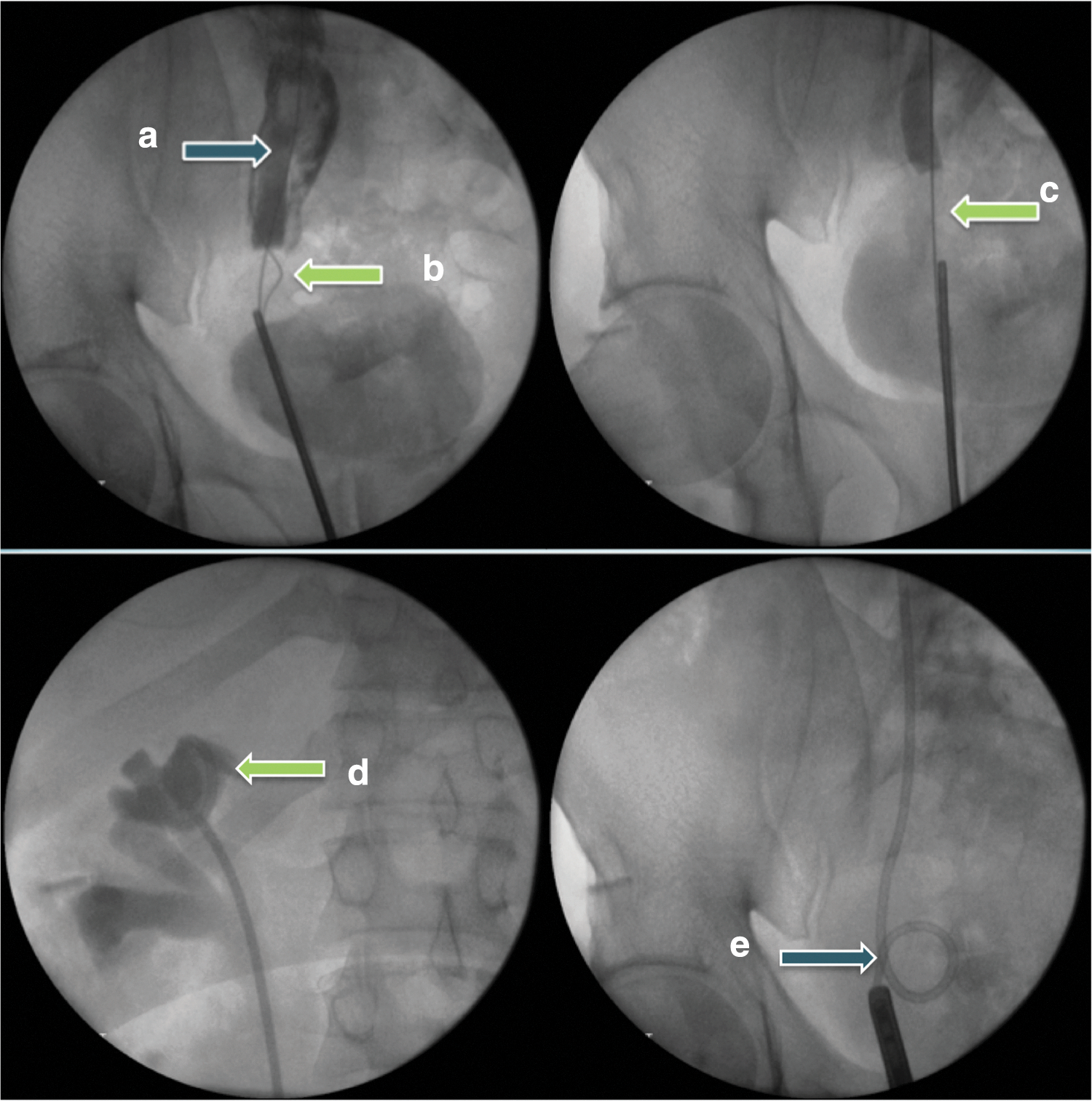
Fluoroscopy images from initial attempt at ureteroscopy and retrograde Double-J stent insertion. Arrows point to
Six weeks after the original procedure the patient underwent repeat ureteroscopy; this showed a dense right distal ureteral stricture. This was biopsied and ablated with LASER. A further Double-J ureteral stent was placed.
Histologic analysis of the ureteral tissue showed both calcified and noncalcified eggs, multinucleated giant cells, and eosinophils (Fig. 3) pathognomonic of S. haematobium infection.
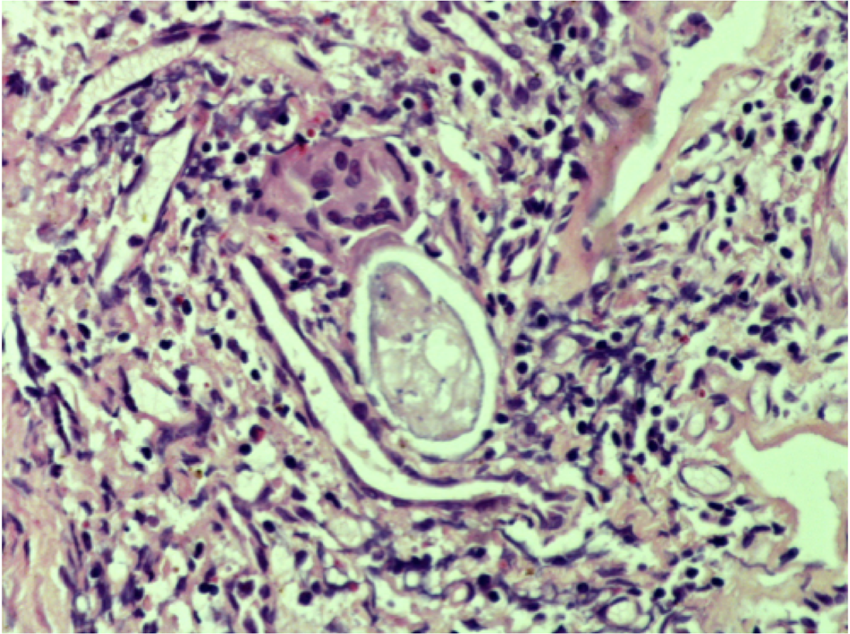
Ureteral biopsy. Arrows point to
The patient was then treated with a 40 mg/kg dose of praziquantel in a divided dose and given a reducing course of steroids in an attempt to reduce the inflammation seen at biopsy; at a third ureteroscopy 2 months later the ureter visually appeared to be open and urine could be seen draining through its lumen. The stent was removed at this stage. A further biopsy at this procedure demonstrated ongoing chronic inflammation with some calcified ova. In view of this he was given a further split dose of 40 mg/kg of praziquantel without steroids as the inflammation was not felt to be steroid responsive.
MAG-3 renogram carried out 4 weeks after stent removal showed a curve with equivocal drainage; repeat MAG-3 renogram a further 3 weeks later showed an obstructed curve with deteriorating renal function. This indicated that the stricture was recurring and that the kidney was not draining adequately. The ureteral stent was replaced and the patient underwent reconstructive surgery with Boari flap ureteral reimplant. Due to local surgical expertise this was done open. Follow-up MAG-3 showed normal unobstructed drainage (Fig. 4). He will continue to have routine annual cystoscopies for surveillance of his bladder mucosa given the increased risk of bladder squamous cell carcinoma in these patients.
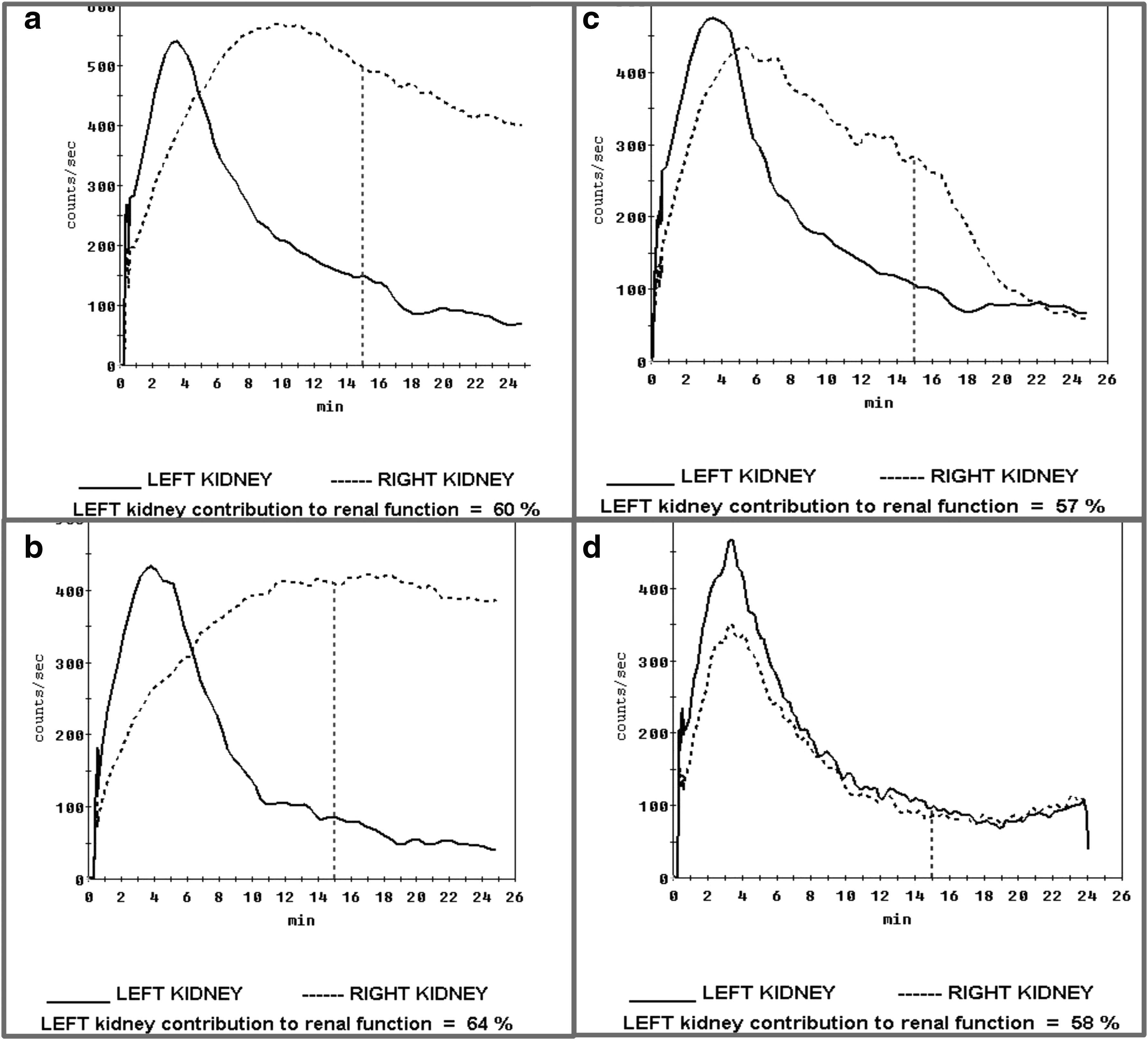
Sequential MAG-3 renograms.
Discussion and Literature Review
This case illustrates the clinical challenges of diagnosing schistosomiasis. In Europe it is a rare disease and early diagnosis can prevent serious complications. In this instance the clinical history and intraoperative findings were key “red flags” indicating a possible diagnosis of schistosomiasis. Despite the initial urine microscopy and serum serology both being negative, the diagnosis was only finally confirmed on tissue biopsy; this may have been due to his concomitant HIV infection which could have attenuated his serologic response to his schistosomiasis infection. It may also have been that his worm burden and subsequent ova excretion levels were low (he had been exposed to fresh water as a child in Zimbabwe but not since). This would fit with the absence of ova in his urine. The pathology was hence a reflection of a few ova that had become embedded in the ureteral mucosa at a site where obstruction occurred easily.
Factors in the history that raised a suspicion of schistosomiasis included the patient's exposure history and the presenting complaint of hematuria, which on further questioning he reported occurring periodically since childhood. Zimbabwe has the second highest rates globally of S. haematobium infection, after Malawi. 1
In a recently published large case series looking at over 1020 cases of diagnosed schistosomiasis in a tertiary referral hospital in London, 57% of patients with ova positive S. haematobium included hematuria as one of their presenting symptoms. 3
Our patient had a normal eosinophil count and negative urine microscopy and serology. In the large case series described previously 3 58% of patients did not have eosinophilia. The yield for ova in urine samples was 20%, with no significant difference in yield for travelers or patients born in endemic regions. Results from this study estimate the sensitivity of schistosomal serology testing to be 91.1% for travelers and 78.9% for patients born in an endemic region. This reflects the time from exposure to presentation in a nonendemic country, usually longer in those born in an endemic region presenting with the chronic consequences of ova deposition in tissues rather than the symptoms of acute schistosomiasis in travelers.
Conclusion
Treatment of schistosomal ureteral strictures remains challenging. Treatment with praziquantel kills the adult worms but the chronic inflammatory changes surrounding the ova persist. Since endourologic treatments such as dilatations tend to fail except in the simplest of strictures, the literature generally advocates reconstructive surgery for the best results. 2 In this case endourologic treatment was initially attempted with LASER ablation of the stricture. Despite intraoperative visual appearances of a wide-open ureter, consecutive MAG-3 renograms indicated the kidney re-obstructed, presumably secondary to fibrosis and therefore recurrence of the stricture in the distal ureter.
This case demonstrates the difficulties involved in diagnosing and treating schistosomiasis and its urologic complications. It illustrates that initial tests can often be negative but if the clinical history and operative findings raise a suspicion of schistosomiasis it is worth persevering as a tissue biopsy can often confirm the diagnosis.
Footnotes
Disclosure Statement
No competing financial interests exist.