
Abstract
We report a case of retained Double J ureteral stent with huge, multiple calculi at both ends in a 10-year-old female child. The renal and bladder calculi were managed by percutaneous nephrolithotomy and percutaneous cystolitholapaxy in a single sitting.
Introduction
Management of upper urinary tract calculi has evolved dramatically in children in the past few decades. This progress has been possible solely by adopting and applying adult endourologic methods in the management of pediatric stone disease. The most important catalyst in the evolution of surgical advancement has been with development of smaller and more durable endoscopic equipment. This advance has allowed easier endourologic treatment in children at an earlier age. 1
Initially, urologists were reluctant to perform percutaneous nephrolithotomy (PCNL) in children because of several concerns, which included the use of large instruments in pediatric kidneys, parenchymal damage, associated effects on renal function, radiation exposure with fluoroscopy, and risks of major complications, including sepsis and bleeding. Potential sequela of hypothermia (i.e., coagulopathy) from prolonged exposure to irrigation was also a deterrent to performing PCNL in children. Today PCNL is used either as a monotherapy or in combination with shockwave lithotripsy SWL (sandwich therapy) in children to achieve stone-free rates ranging from 68% to 100%.1,2 Although there is no current international consensus, relative indications for PCNL as a primary treatment modality in children include large upper tract stone burden (>1.5 cm), lower pole calculi larger than 1 cm, concurrent anatomic abnormality impairing urinary drainage and stone clearance, or known cystine or struvite composition. 3 We report on a child with a retained Double J (DJ) ureteral stent with both renal and bladder calculi treated with PCNL and PCCL (percutaneous cystolithotripsy) in a single sitting.
Case Report
A 10-year-old female child presented with pain in the left flank of 2 months duration. She was a known case of urolithiasis and had undergone left-sided ureteroscopy/extraction of ureteral calculi/DJ stent insertion 2 years prior. The child and her parents did not follow up with her previous urologist, despite being made aware of the DJ stent removal. Plain X-ray kidney, ureter and bladder (KUB) revealed the presence of a DJ ureteral stent on the left side with multiple calculi on both the sides, that is, bladder and kidney (Fig. 1). Serum creatinine was 0.5 mg% and hemoglobin was 10.4 g%. Plain CT revealed multiple renal calculi on the left side, the largest measuring 2.7 × 1.7 cm, with multiple bladder calculi, the largest measuring 3.8 × 1.3 cm (Fig. 2).

Plain X-ray kidney, ureter and bladder (KUB) showing retained Double J (DJ) stent on left side along with renal and vesical calculi.

Plain CT showing retained DJ with renal and vesical stone.
It was decided to tackle the stones in one sitting. Under cover of injectable antibiotics and under general anesthesia, the child was placed in supine position. PCCL was performed using a 24F nephroscope and pneumatic lithotripter. Once the bladder calculi were extracted, the child was positioned in the prone position. PCNL was performed using an 18F amplatz and 16F pediatric nephroscope. All the stones were extracted along with the retained DJ stent (Fig. 3). A new 4.5F DJ was inserted along with a 12F nephrostomy catheter. The total operating time was 240 minutes. and blood loss was <50 mL. After surgery, the child was placed in supine position and it was noticed that the child's abdomen was distended. Intraoperative ultrasonography revealed collection of fluid in the peritoneal cavity. A small intraperitoneal drain was introduced and connected to a collection device. Postoperatively the child had an uneventful recovery. The intraperitoneal drain was removed after 48 hours, nephrostomy after 24 hours, suprapubic cystostomy after 72 hours, and perurethral catheter after 5 days. The child did not require any blood transfusions. Postoperative plain KUB showed no evidence of residual calculi.
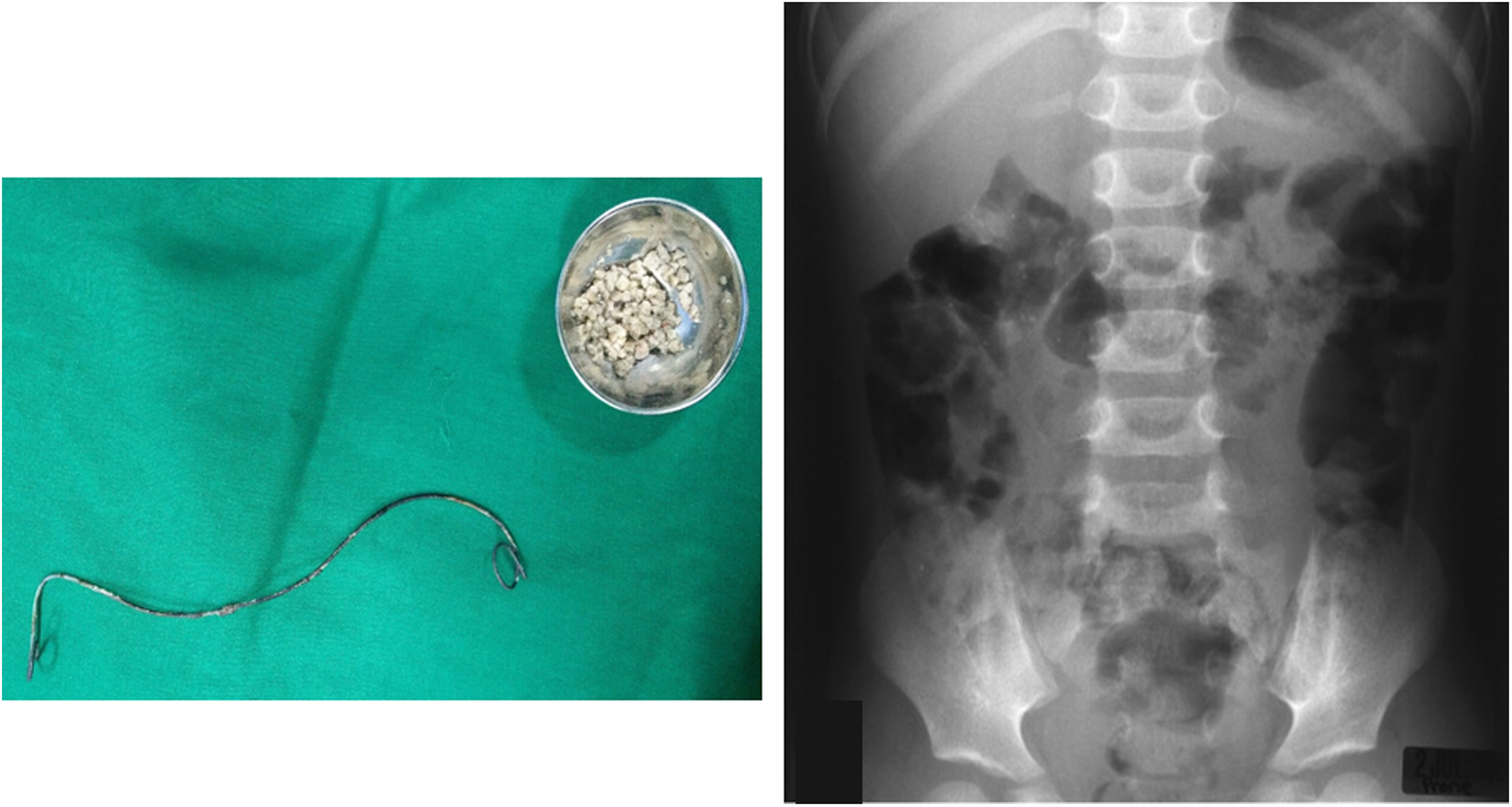
Left: extracted DJ stent and calculi. Right: postoperative KUB.
Discussion
Urinary lithiasis affects between 5% and 10% of the humans during their lifetime, 2%–3% of them being children. 2 There is a wide epidemiologic variation in relation to pediatric urolithiasis in developed and the developing nations, with a prevalence of 1%–5% to 5%–15%, respectively. 2 Management of stone disease in children necessitates complete stone clearance, eradication of urinary infection, and appropriate correction of any underlying metabolic or anatomical abnormalities. 2
Since their introduction into clinical use, DJ ureteral stents have been widely used in urologic practice. DJ ureteral stents have been used to establish or improve drainage in cases of extrinsic or intrinsic obstruction of urinary passage. They have also been placed after iatrogenic injuries to the ureter and prophylactically in complex urinary tract reconstructive surgeries. Over the decades, technological improvements in stent design and stent biomaterials have greatly minimized patient discomfort. As a result, DJ stents have been left in place for a longer duration of time, and it is possible that the patient and the treating physician may forget their presence. These forgotten or retained ureteral stents could lead to various complications such as stent migration, stent occlusion, breakage, encrustation, and stone formation. 4 Despite improved design and biomaterial used, encrustation remains one of the most important side effects. Encrustations are most frequently noted in forgotten/retained DJ stents, which remain indwelling for a long period of time. 4
Nerli et al. 4 reported on a total of 14 children who underwent removal of forgotten/retained DJ ureteral stents. A combination of SWL, cystolithotripsy, and PCNL was done to free the DJ stent and extract it. The authors felt that forgotten/retained stents in children are a source of severe morbidity, additional/unnecessary hospitalization, and definitely a financial strain. In this case, the child developed huge and multiple stones on both ends of the retained DJ stent, needing to undergo prolonged surgery. A forgotten or retained ureteral stent is a preventable event, and the literature is abundant with reports of forgotten DJ stents. The reason for ureteral stents being forgotten is because of failure on the part of the treating surgeon to counsel the patient or the parents in the case of children. To overcome the issue of forgotten stents, maintenance of stent registry has been suggested. An automated information system mounted on a mobile app would be useful to remind the patient/parent/guardian regarding stent removal.
Footnotes
Disclosure Statement
No competing financial interests exist.