
Abstract
Background:
While studies have identified the negative cardiovascular effects of obesity, the effects of obesity on youth athletes are less studied. This study investigates the associations between obesity in youth athletes and exercise activity and exertional cardiac symptoms.
Methods:
The HeartBytes National Youth Database produced by Simon's Heart, a nonprofit that organizes adolescents' sports pre-participation examinations (PPEs), was used. This database contains demographic data, exercise-related symptoms, and electrocardiogram data obtained during PPEs. BMI was converted to percentiles, with obesity defined as BMI ≥95th percentile. Outcomes were evaluated using a chi-squared test with odds ratios (ORs) and 95% confidence intervals (CIs).
Results:
Of 7363 patients, there were 634 individuals with obesity. Youth athletes within normal weight ranges (5th–85th percentile) had higher exercise rates than those with underweight, overweight, or obesity (p < 0.001 for each). Athletes with obesity had higher odds of exertional symptoms overall (OR: 1.63 [CI: 1.36–1.96]; p < 0.001). However, for athletes who exercised >10 hours a week, there was no association between obesity and exertional symptoms. Athletes with obesity had higher odds of elevated blood pressure (OR: 5.35 [CI: 2.00–14.30]; p < 0.001) and hypercholesterolemia (OR: 3.84 [CI: 2.51–5.86]; p < 0.001).
Conclusions:
In this dataset, obesity in youth athletes is associated with decreased physical activity and increased exertional symptoms in general. Obesity is not associated with exertional symptoms in athletes who participated in higher weekly physical activity. Further studies are needed to elucidate the cause-effect relationship of these findings.
Introduction
Childhood obesity has become a large public health problem with increasing prevalence and significant impacts on the development of cardiometabolic, pulmonary, orthopedic, and psychiatric comorbidities into adulthood.1–8 Obesity refers to the presence of excess body fat and is frequently measured by BMI with the ratio of an individual's weight to height squared (kg/m2). 9 BMI percentiles for children and adolescents 2–19 years of age are determined by the CDC growth chart, which uses age- and sex-adjusted z-scores.9–11 Pediatric obesity is defined as having a BMI greater than or equal to the 95th percentile or having a BMI >30 kg/m2.12,13 While BMI absolute values are widely used as an estimate of body fat, age- and sex-adjusted BMI percentiles are more accurate at predicting total fat mass in youth 9 to 18 years of age.9,14–16
Within the youth athletes population, obesity remains widely prevalent.17,18 The association between body weight and sport participation varies by study depending on how sport participation is defined.19,20 It has been identified that pediatric populations with obesity may experience dyspnea due to having decreased cardiovascular fitness. 21 In addition, studies have found that adults with obesity may experience dyspnea and chest discomfort, possibly from an increased sensation of respiratory effort during exercise.21–23 However, few studies have looked into the associations between obesity, exercise intensity, and exertional cardiac symptoms. This study explores the association between BMI and exercise intensity, and exercise-induced cardiac symptoms in youth athletes. We hypothesized that among youth athletes, increased BMI percentiles beyond the normal weight range are associated with decreased activity levels, and obesity is associated with increased exercise-induced cardiac symptoms.
Methods
Data Source
This is an Institutional Review Board-approved, retrospective study of the HeartBytes National Youth Cardiac Registry database produced by Simon's Heart, a nonprofit with a mission of sudden cardiac death prevention in children and young adults by organizing pre-participation physicals and examinations. The HeartBytes database includes data on children (youth athletes) 12–20 years of age, who were self-referred and screened at a Simon's Heart pre-participation cardiac examination event between August 2014 and July 2021. During these events, self-reported information was collected on the patient's demographics, past medical history, medication use, family history, participation in sport, and physical activity level. The examination includes obtaining height, weight, and blood pressure measurement, in addition to an electrocardiogram interpreted by a cardiologist at the event. 24
Statistical Analysis
In this study, the age- and gender-adjusted CDC-LMS model was used to assess BMI z-scores and their corresponding percentiles.15,25–30 LMS stands for model variables L, M, and S, which are functions of a youth athlete's age and gender and are used to convert the athlete's BMI to z-score and then BMI percentile. The CDC's BMI classification identified underweight as 0 to less than the 5th percentile, normal weight as 5th to less than the 85th percentile, and overweight as 85th to less than the 95th percentile. Obesity was defined as BMI greater than or equal to the 95th percentile. 31
Continuous variables are reported with mean and standard deviation for normally distributed variables or median and interquartile range for variables not normally distributed. Categorical variables are reported as counts and proportions. Physical activity levels were compared using a t-test, and other categorical variables were compared using Pearson's chi-squared test. Obesity-related outcomes were reported with odds ratios (ORs) and 95% confidence intervals (CIs).
The primary outcomes of the study were self-reported physical activity level per week, comorbidities, and exercise-induced symptoms (easily fatigued, chest pain, dyspnea, syncope, and palpitations). To analyze the association between obesity and exercise-induced dyspnea, individuals with asthma were removed to eliminate its confounding effects. Physical activity level was divided into four levels of increasing activity: <2, 2–5, 5–10, and >10 hours of exercise each week. The comorbidities of interest include elevated blood pressure, diabetes, asthma, hypercholesterolemia, anxiety, depression, and attention-deficit/hypersensitivity disorder (ADHD). Athletes who exercised >10 hours a week were selected as a subgroup for additional analysis.
Results
Demographics
Of the 7425 youth athletes in the HeartBytes database, 7363 had reliable BMI information documented. Of the 7363 individuals, 39.3% were female. The athletes ranged from 12 to 20 years of age. The median age was 15.1 years (interquartile range: 13.5–16.5 years). The patients screened were predominantly White (83.3%) with other represented races, including Black (7.1%), Asian/Pacific Islander (3.9%), and Latino/Hispanic (3.1%) (Table 1). The majority of patients screened came from Pennsylvania, New Jersey, and Georgia.
Demographics of Youth Athletes
There were 634 youth athletes with obesity identified, of which 212 individuals exercised >10 hours per week. Youth athletes with obesity exercising >10 hours a week mainly participated in football (62%) and basketball (16%). The majority of individuals had BMI percentiles in the normal weight range, followed by overweight, with obesity, and underweight. The mean BMI of all youth athletes before percentile conversion was 21.6 kg/m2, with standard deviation of 4.19 kg/m2 (Table 2).
BMI Percentiles of Screened Youth Athletes
Physical Activity Level
Athletes with different BMI percentiles had distinct distributions of physical activity per week (Fig. 1). Youth athletes classified within normal weight ranges had significantly higher mean exercise levels and the highest rate of exercising >10 hours per week compared to athletes who were with underweight, overweight, or obesity (p < 0.001 for each). Table 3 shows the comparison of weekly physical activity distribution between youth athletes with and without obesity. Compared to those without obesity, a higher percentage of youth athletes with obesity exercised <5 hours per week (p < 0.001). Furthermore, a lower percentage of youth athletes with obesity exercised >10 hours per week compared to those without obesity (p < 0.001).
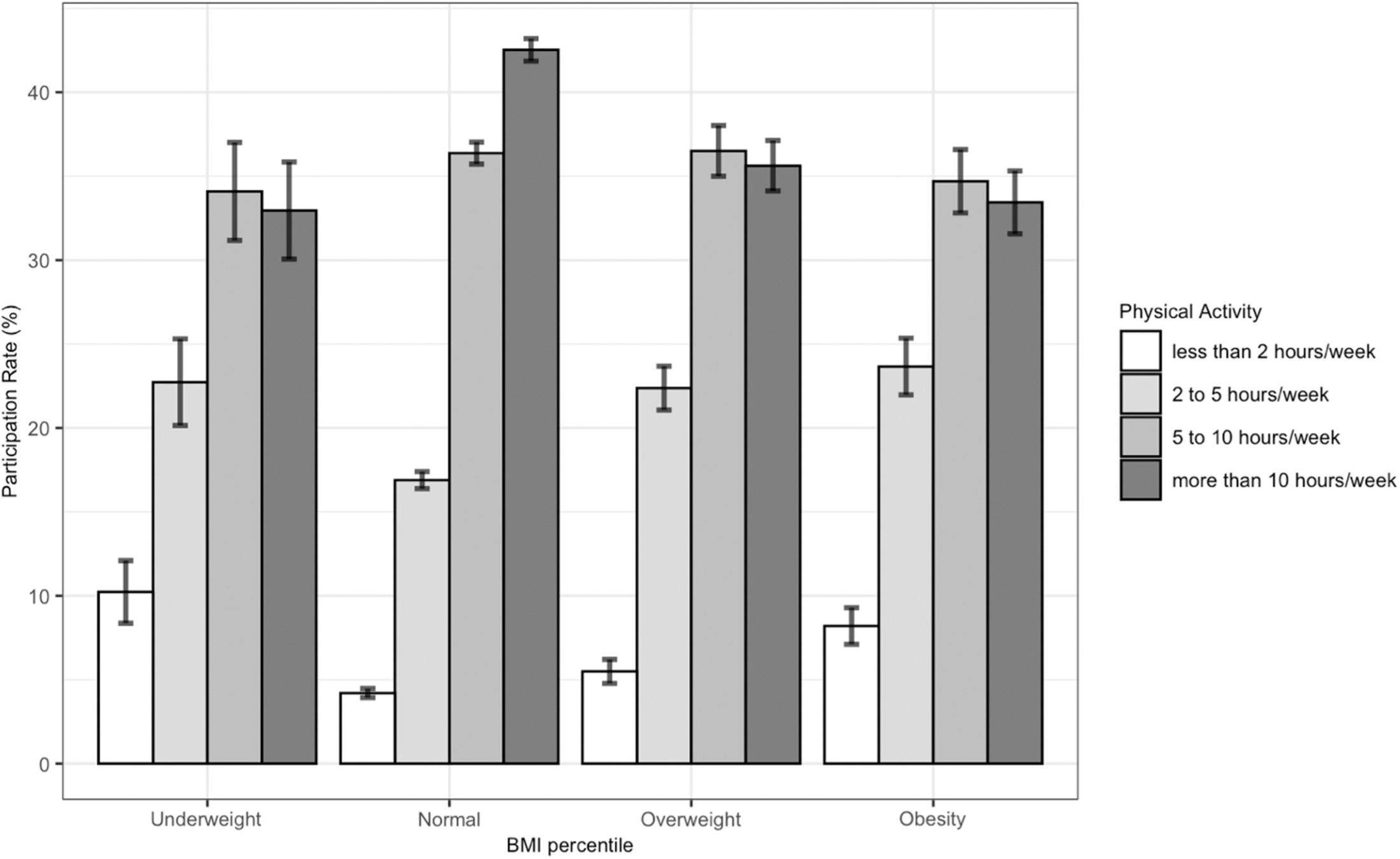
Physical activity of youth athletes based on their weight classification. Error bars represent standard deviation.
Comparison of Physical Activity Distribution between Athletes With and Without Obesity
Comorbidities
Obesity in youth athletes was associated with various comorbidities (Table 4). In general, the odds of asthma were significantly higher in individuals with obesity than in individuals without obesity (OR: 1.27; 95% CI: 1.04–1.56, p = 0.017). However, for youth athletes exercising >10 hours per week, there was no significant association between obesity and asthma.
Association of Obesity and Comorbidities
ADHD, attention-deficit/hypersensitivity disorder; CI, confidence interval; OR, odds ratio.
Youth athletes with obesity were significantly more likely to have elevated blood pressure and high cholesterol when compared to those without obesity (OR: 5.35; 95% CI: 2.00–14.30, p < 0.001 and OR: 3.84; 95% CI: 2.51–5.86, p < 0.001, respectively). In athletes who exercised >10 hours per week, obesity was also associated with elevated blood pressure and high cholesterol (OR: 13.16; 95% CI: 1.84–93.9, p < 0.001 and OR: 7.62; 95% CI: 3.33–17.5, p < 0.001), respectively.
Exertional Symptoms
In general, obesity in youth athletes was also associated with various exercise-induced cardiac symptoms (Table 5). In terms of predominant exercise-induced symptoms, youth athletes with obesity were more likely to feel easily fatigued (OR: 3.00; 95% CI: 2.38–3.79, p < 0.001) and dyspnea (OR: 1.92; 95% CI: 1.42–2.60, p < 0.001) than individuals without obesity. However, for youth athletes exercising >10 hours per week, there was no significant association between obesity and exertional cardiac symptoms.
Associations of Obesity With Exercise Symptoms
n = 6050 after adjusting for asthma.
Discussion
In this cross-sectional study of 7363 youth athletes, findings suggest that youth athletes classified within normal weight ranges had significantly higher mean exercise levels compared to athletes who were not classified within normal weight ranges. Youth athletes with obesity had significantly lower exercise levels compared to those without obesity. In addition, obesity in youth athletes is associated with various comorbidities and exercise-induced symptoms. However, for athletes who participated in higher weekly physical activity, obesity is not associated with asthma and exertional symptoms.
Youth athletes with normal weight BMI percentiles were significantly more active than athletes with BMI percentiles outside this range. Specifically, athletes with overweight or obesity had lower participation rates of exercising >10 hours a week than athletes with BMI percentiles within normal weight limits. This is consistent with the findings of previous studies that exercise activity levels in children and adolescents with obesity are significantly lower than exercise activity levels in children and adolescents who are not with overweight or obesity.32–34 Since higher fat mass percentages are associated with decreased relative muscle mass, individuals with obesity tend to have lower physical fitness and decreased physical activity in comparison to individuals with normal fat mass percentages. 35 This suggests that these exercise activity trends among children and adolescents may also apply to youth athletes.
Exercise continues to be a hallmark therapy for improving cardiometabolic health in children. Participating in frequent exercise is particularly important for children with obesity, who are inherently at higher risk for cardiovascular comorbidities such as high blood pressure and high cholesterol. Unfortunately, our study highlighted a stark contrast in activity levels between youth athletes with and without obesity. A large proportion of youth athletes with obesity in our study exercised for <10 hours per week. On the other hand, athletes with obesity who exercised for >10 hours a week had fewer symptoms and comorbidities. This suggests the need for programs to promote physical activity in youth athletes with obesity. Further research is needed to fully understand the limitations to exercise in youth athletes with obesity.
This study found that obesity is associated with other comorbidities, including asthma, elevated blood pressure, and hyperlipidemia in general. Obesity is a risk factor for asthma in youth and is also associated with more severe symptoms and exacerbations and reduced response to treatments. 36 Asthma may be a contributing factor to symptoms of difficulty breathing on exertion in youth athletes with obesity. The presence of elevated blood pressure and hypercholesterolemia in childhood is associated with adverse cardiovascular outcomes in earlier adulthood, 37 and this trend may be relevant among youth athletes.
The associations between obesity and diabetes, and obesity and psychiatric comorbidities were not statistically significant. With diabetes, studies have found that obesity and hypertension are important components of metabolic syndrome, which increase the future risk of developing diabetes.38,39 Youth athletes with obesity may not be affected by diabetes immediately, given the long-term development of diabetes. With psychiatric comorbidities, mental health diagnoses are often underreported, especially in males. 40 Since the majority of youth athletes in the Heartbytes database were male, it is likely that diagnoses of depression, anxiety, and ADHD could be underreported and hence underrepresented.
Multiple studies have previously identified dyspnea on exertion as a common finding in individuals with obesity, which is attributed to increased work of breathing and impaired respiratory muscle function.41,42 However, few studies have explored dyspnea on exertion in the pediatric athlete population with obesity. In this analysis, findings suggest that at BMI levels greater than the 95th percentile, athletes were more likely to have exercise-induced cardiac symptoms of difficulty breathing and feeling easily fatigued compared to athletes without obesity. This suggests that the physiologic mechanisms of dyspnea on exertion may also apply to youth athletes.
This study found that obesity was not associated with asthma and exertional symptoms in the subgroup of athletes who engaged in higher weekly physical activity. Since the majority of athletes with obesity exercising at higher physical activity participated in football and basketball, these athletes may engage in more anaerobic exercise and strength training rather than sustained aerobic exercise. Furthermore, BMI does not take into account the mass ratio of muscle to fat, so these athletes may have elevated BMI without elevated amounts of adipose tissue. This may explain why these individuals had fewer symptoms than other youth athletes with obesity. Further investigation is needed to address why this group of athletes had higher odds of elevated blood pressure and hypercholesterolemia.
Limitations
The HeartBytes dataset is unique in its patient population and data collection process as it is set up as a database of screened youth. This population is predominantly White (83.3%) and male (60.7%), therefore limiting the generalizability of results. The questionnaire completed at screenings is self-administered, and the collected data are therefore self-reported. This process makes these data subject to response bias.
A response bias may exist as respondents had to self-report whether they felt certain cardiac symptoms when exercising. However, no option was available for respondents to specify how frequently they experienced cardiac symptoms or the severity of these symptoms. Athletes who do not exercise frequently may be less likely to experience and report exercise-induced symptoms. Moreover, the types of cardiac symptoms were predetermined, so any additional symptom that was not previously outlined by the questionnaire would not have been recorded. In addition, BMI is an imperfect measure of obesity, as children with high amounts of muscle mass may have an elevated BMI, despite having normal or low levels of adipose tissue.
Conclusions
In this dataset from a large national pre-participation examination registry, obesity in youth athletes was associated with decreased physical activity, elevated blood pressure, hypercholesterolemia, and an increased rate of exertional symptoms in general. Obesity is not associated with exertional symptoms in athletes who participated in higher weekly physical activity. Youth athletes within normal weight ranges were found to have significantly higher levels of physical activity compared to those with BMI percentiles outside the normal weight range. Further studies are needed to elucidate the cause-effect relationship of these findings.
Impact Statement
This study identifies associations between obesity and increased exertional cardiac symptoms in youth athletes, a population that is not as well studied. Obesity in youth athletes is associated with elevated blood pressure, hypercholesterolemia, and decreased physical activity compared to youth athletes within normal weight ranges.
Footnotes
Acknowledgments
Authors' Contributions
G.Q.: Conceptualization (lead), methodology (lead), data curation, formal analysis (lead), writing—original draft (lead), and writing—review and editing (equal). J.M.R.: Formal analysis (supporting) and writing—review and editing (equal). S.D.: Conceptualization (supporting), methodology (supporting), and writing—review and editing (equal). D.J., I.M., A.G.H., and D.S.: Writing—review and editing (equal).
Funding Information
No funding was secured for this study.
Author Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.