
Abstract
Abstract
Background:
Living near community recreation centers (CRC) is associated with increases in adolescent and adult physical activity, but the efficacy of efforts to increase use among Latino parents and young children is unknown. We hypothesized that Latino parent–child dyads with exposure to a CRC through culturally tailored programming would be more likely to use the facility for physical activity a year after programming ended than dyads living in the same geographic area who were not exposed to the programming.
Methods:
Self-identified Latino parent–child dyads who had participated in a randomized controlled trial (RCT) of a culturally tailored healthy lifestyle program and completed a 12-month follow-up assessment constituted the “exposed” group (n=66). The “unexposed” group included 62 parent–child dyads living in the same zip codes as the exposed group, all within a 5-mile radius of the CRC. Participants completed in-person structured interviews.
Results:
Approximately two-thirds of exposed parents reported more than monthly use of the CRC for themselves a year after programming ended, compared to one-third of unexposed Latino families with the same geographic access (χ2=11.26, p<0.01). Parents in the exposed group were four times more likely than the unexposed group to use the CRC with their children on a monthly basis (odds ratio=4.18, p<0.01).
Conclusions:
CRCs that develop culturally tailored programs that invite Latino families inside can increase sustained CRC use for physical activity in this population at heightened risk for childhood obesity.
Introduction
Physical activity rates decline dramatically as children grow from childhood to adolescence, a decline that continues with age and that holds true not just for Latinos but for the entire U.S. population.10–13 Because most Americans do not meet daily activity recommendations, policymakers have established goals to increase the number of people who lead active, healthy lives.14,15 However, there are barriers to physical activity, such as unsafe neighborhoods and limited access to built environments.16,17 In one report, obesity rates were 20%–60% higher among children living in neighborhoods perceived as unsafe, or those with poor housing and no sidewalks. 18
Built environments—man-made surroundings such as sidewalks, community recreation centers (CRCs), schools, grocery stores, and parks—may be either barriers to or facilitators of healthy lifestyles. For example, children tend to have higher BMI values if they live closer to fast-food restaurants. 19 Conversely, adolescents and adults who live near a CRC tend to engage in more moderate levels of physical activity.11,20–22 Currently, there is no definitive research showing how Latino families with young children, a population at disproportionately high risk for developing obesity, use their built environment.
The purpose of this study was to assess how exposure to a CRC affects its use for physical activity by Latino families with young children 1 year after initial exposure. We focused on CRCs because they are publicly accessible, at low cost to users, and provide built environmental resources for physical activity (e.g., walking tracks, swimming pools, basketball courts, exercise equipment). We hypothesized that Latino parents with systematic exposure to a CRC through culturally tailored programming would be more likely to use the facility for physical activity by themselves and with their preschool children 1 year after programming ended relative to Latino families who had similar geographic access but were not exposed to a CRC through programming.
Methods
These analyses are based on a supplemental cross-sectional study carried out with equal-sized groups of Latino parent–preschool child dyads who were exposed versus unexposed to culturally tailored programming at a public CRC.
Participants
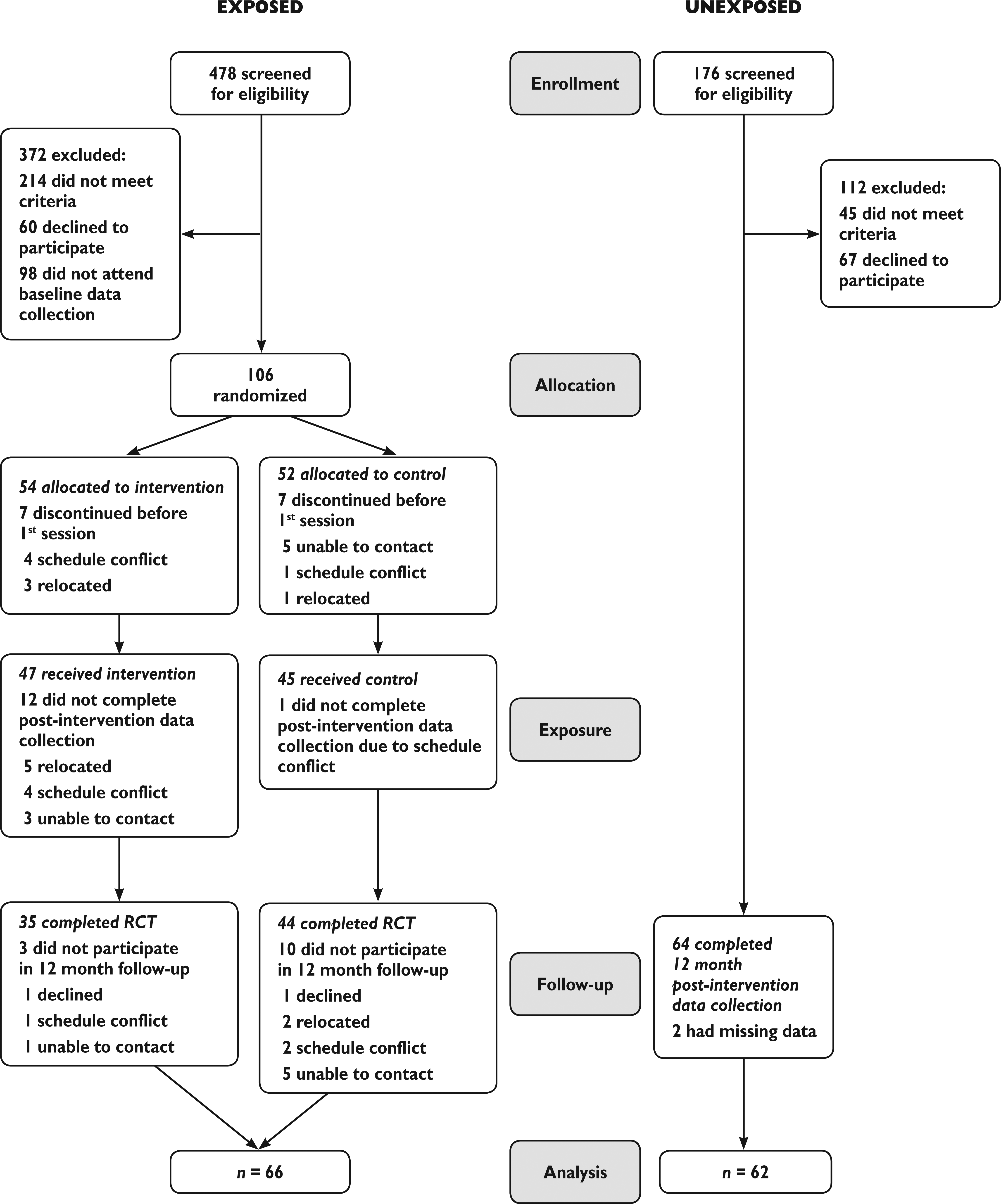
The full sample consisted of 130 self-identified Latino parent–child dyads (66 exposed and 64 unexposed). Prior to the enrollment into this study, half of the sample (n=66) had participated in a randomized controlled trial (RCT) of a culturally tailored, family-centered behavioral intervention, Salud con la familia (Health with the Family). For the RCT, parents older than 18 years were eligible if they: (1) Self-identified as Hispanic/Latino/a, (2) had a child aged 3–5 years not currently enrolled in another healthy lifestyle program, (3) had a valid phone number, and (4) planned on remaining in the city for the next 6 months. Families were recruited from two general pediatric clinics that serve Spanish-speaking populations from zip code regions within a 5-mile radius of the CRC. Out of 106 eligible, 79 dyads (35 treatment, 44 control) participated in the pre- and postintervention data collection waves of the RCT (see Fig. 1). The Salud con la familia treatment condition consisted of 12 weekly sessions designed to improve nutritional family habits, increase weekly physical activity, and decrease media use (sedentary activity), and was based on a best practice program developed by the National Latino Children's Institute (NLCI). 23 The control condition consisted of three monthly school readiness sessions. Both programs were culturally tailored and delivered in the same CRC. We refer to the 66 participants (32 treatment, 34 control) who completed a follow-up interview 12 months postintervention (86% retention) as the “exposed” group for the purposes of this paper because they had repeated exposure to the CRC by attending the culturally tailored programs. Both the intervention group (potentially exposed to the built environment 12 times) and the control group (potentially exposed to the built environment 3 times) were considered to be the exposed condition for our analyses.
Our comparison (“unexposed”) group consisted of 64 parent–child dyads who did not participate in the Salud Con La Familia RCT, but were recruited from the same general pediatric clinics as the exposed group. Eligibility criteria for the comparison/unexposed group included: (1) Parent older than 18 years, (2) who self-identified as Hispanic/Latino/a, (3) had a child aged 3–6 years (as of February 2009, to match ages of children enrolled in the RCT), (4) did not (nor did a family member) participate in Salud con la familia, (5) lived in one of the same zip codes in which RCT participants lived (when the RCT was conducted), and (6) could identify the CRC in their community (and thus answer questions about it). Two of the unexposed participants were missing data on CRC use, so for the reported analyses the comparison group consists of 62 participants.
Procedures
Data collection occurred during March to April, 2010, for the exposed group and July, 2010, for the unexposed group. Eligible adults underwent an oral consent process in Spanish before providing written consent. Trained, bilingual research assistants (RAs) read survey questions aloud for parents (in the language of their choosing), and parents noted their answers by completing the paper-based survey. All interviews were conducted at the CRC. Study procedures were approved by the Vanderbilt University Institutional Review Board (IRB#091131).
Measures
Use of the CRC was measured with two self-report questions. As an indicator of their use, parents were asked, “In a typical week, how often do you go to your community recreation center?”, and they were instructed to respond about their use without their children. To indicate use with their child, they were asked “In a typical week, how often do you go to your community recreation center with your children?” Parents responded using a 5-point frequency scale from “every day” (5) to “more than once a month” (2), to “never” (0). To have large enough groups for statistical comparison, scores for parent use and parent use with child were dichotomized as “0” if the frequency was once a month or less and “1” if the frequency was more than once a month. For descriptive purposes, the parents also reported how frequently they themselves and they and their preschool child had participated in specific physical activities offered at the CRC (e.g., walking track, swimming pool).
An item from the Ainsworth Environmental Supports for Physical Activity Questionnaire 24 was used to measure perceptions of safety of the CRC. Parents were asked, “How safe are the public recreation facilities in your community?”, and they responded using a 4-point scale from “not at all safe” to “very safe,” or they could choose “don't know.” Perceived safety was categorized as “2” if the participant perceived the CRC as “very safe,” “1” if the participant didn't know, or “0” for all lesser ratings of safety. Because residents from the neighborhood from which participants were recruited relied on privately owned automobiles more than public transportation, as an indicator of access to the CRC, parents were asked, “How many automobiles, vans, and trucks of one-ton capacity or less are kept at home for use by members of your household?” 25
Parents completed a demographic survey that included date of birth, gender, and country of origin of parent and child, parental education, and marital status. They also reported the number of people living in their homes. Acculturation was measured using the previously validated Brief Acculturation Scale for Hispanics (BASH). 26 The BASH asks parents what language they speak, use at home, think in, and use among friends given the following options: Spanish only, Spanish better than English, Spanish and English equally, English better than Spanish, and English only. Responses were averaged across the four items, with scores ranging from 1 to 5; <2 indicates a low level of acculturation. 26 Internal reliability of the BASH scale was α=0.81 in our sample.
Statistical Analysis
We conducted chi-squared and Student t-tests to compare the exposed and unexposed groups on demographic variables, access to the CRC, and perceived safety. Next, we conducted a chi-squared analysis to test the difference between groups in use of the community recreation center by parents alone and with their children. Logistic regression models were conducted to test the effect of exposure to the CRC on parent only and parent with child use of the CRC independent of access and perceived safety (dummy coded with “very safe” as reference group). Follow-up univariate logistic regression models were conducted to test the effect of “dosage” (i.e., number of sessions attended by the exposed group) on use of the CRC by parent only and parent with child. All the analyses were conducted with STATA/IC 11.1, and p values less than or equal to 0.05 were considered significant.
Results
Sample Description
Chi-squared and Student t-tests revealed few statistical differences in demographic characteristics between the exposed and unexposed groups for parents and children (Table 1). The majority of both groups of parents were born in Mexico with low levels of acculturation. Parents in the exposed group had completed higher levels of education than parents in the unexposed group. While the exposed group was more likely to have completed high school or a certificate of General Educational Development (GED), the majority of parents in both groups had not obtained a high school degree. Parents in the exposed group had significantly more cars available than parents in the unexposed group, but there was no significant group difference in the percentages of parents who perceived the CRC as safe. The majority of participants in both the unexposed (71%) and exposed (72%) groups lived in the same two zip codes (results not shown to protect participant confidentiality), indicating that the exposed and unexposed groups had comparable geographic access to the CRC.
Descriptive Statistics among Study Sample
Note: Student t-tests conducted for continuous variables and χ2×test conducted for categorical variables.
BASH, Brief Acculturation Scale for Hispanics; GED, General Educational Development; CRC, community recreation centers.
CRC Use by Group
There was a significant group difference in parents' use of the CRC by parents themselves (Table 2). Almost two-thirds (65%) of the exposed group reported at least monthly use of a CRC, whereas only one-third (36%) of the unexposed group did (χ2=11.26, p<0.01). There was also a significant group difference in parents' use of the CRC with their young children. The majority of the exposed parents (62%) reported more than monthly use of the CRC with their young children compared to only 26% of the unexposed group (χ2=17.07, p<0.001).
Use of Recreation Center by Group, I Year after Exposed Group Participated in Culturally Tailored Programming at Community Recreation Center
Follow-up analyses within the exposed group indicated that the number of sessions attended was not a significant predictor of monthly CRC use by parents alone [odds ratio (OR)=1.04; p=0.62] or parents with their children (OR=1.10; p=0.21), indicating that any systematic exposure through culturally tailored programming is associated with continued CRC use. The CRC activities used by parents with their preschool children, for those reporting CRC use, included the playground (74%), the walking track (36%), and the swimming pool (17%). When using the CRC by themselves, most parents reported using the walking track (41%).
Independent Predictors of CRC Use
We conducted two logistic regressions predicting monthly use of the CRC by parent only and parent with child, from group assignment, access, and perceived safety (Table 3). When controlling for access and perceived safety, which were not significant predictors, parents in the exposed group were twice as likely to use the CRC for physical activity by themselves (OR=2.28, p<0.05) and over four times more likely to use the CRC with their children (OR=4.18, p<0.01) than parents in the unexposed group.
Logistic Regressions Predicting Community Recreation Center Use by Parents Only and Parents with Their Young Child
N=128 (62 unexposed, 66 exposed).
N=114 (53 unexposed, 61 exposed, due to missing data on perceived safety).
p<0.05. **p<0.01. ***p<0.001.
OR, Odds ratio; SE, standard error.
Discussion
Systematically exposing Latino families with young children to a CRC through culturally tailored programming increased the likelihood of continued use for physical activity by parents and their preschool-age children 1 year after initial exposure. These findings are consistent with prior research that demonstrated the use of the built environment increases physical activity.4,22,27 However, these studies did not focus on parents and preschool-age children, especially at-risk, low-acculturated, Latino families who are disproportionately affected by childhood obesity. Activity habits set in early childhood can profoundly influence lifelong trajectories for health,28,29 so exposing children as young as preschool-age to the use of CRCs for physical activity can have enormous potential for preventing obesity and its major complications.
That there was no significant effect of the number of program sessions attended on CRC use suggests that even minimal exposure to a CRC through culturally tailored programming can increase the likelihood of Latino parents and children regularly (i.e., monthly) using a CRC for physical activity.
Family-centered programming can encourage use of the built environment for physical activity when it includes social and environmental behaviors that support healthy lifestyles in a culturally sensitive way. This study adds to the growing body of research supporting the efficacy of community-based programming to address childhood obesity and its feasibility with minimal funding through the use of existing community-based resources.30,31
Our study indicated that one of the most popular facilities for physical activity at the CRC was the walking track for both parents alone and with their young children. This area of the CRC is open to the public and requires no membership fees, but this accessibility (free, open during light hours) was only known to parents exposed to the CRC through programming that brought them inside the built environment. Individuals in our unexposed group knew about the walking track and ball fields; however, in key participant interviews conducted before the RCT, many Latino parents of preschoolers mentioned that they did not believe these facilities were for their use. This demonstrates the need to reach out and publicize community resources to Latino residents to encourage them to utilize their built environment for physical activity.
Prior studies indicated that access (defined by distance to a facility, number of routes available to reach a facility, and cost) is a determinant of use of CRCs and level of physical activity.22,32 We used the total number of vehicles in the home as a measure of access in our study because distance to the facility was controlled through sampling within a 5-mile radius of the CRC, and vehicles were identified as the primary “route” to the CRC, given limited public transportation options. While other studies have found access to be a predictor of physical activity,11,20–22 our study found that promoting the built environment with culturally tailored programming was a stronger predictor of CRC use than access, which was insignificant. This is consistent with recent research conducted by Cohen et al. investigating the relationship of park characteristics with park use, which concluded that programming is the strongest predictor of park use and physical activity. 33
Moreover, in our study, perceived safety was not significantly associated with CRC use. This seems to be due to a restricted range of responses, with very few participants perceiving the CRC as unsafe. Although research has documented that perceptions of low safety are a barrier to public park use, perceptions of high safety do not facilitate park use. 33
Limitations
Our study is cross-sectional, which limits our ability to examine directionality and causality, and as a supplemental follow-up, the comparison group was not randomly assigned. However, this is a first step in understanding how any systematic exposure to built environments through culturally tailored programming affects Latino parents' and their young children's physical activity. Future research is needed to determine whether CRC use helps Latino families meet recommendations for physical activity. Our operational definition of access was the number of vehicles in the home, which may not directly reflect access for all families. For example, while the sampling frame was constrained to a 5-mile radius around the CRC to control for geographical access, there remains variability in who could walk to the CRC versus those families who needed to use a car. This may explain why access was not a statistically significant predictor of CRC use. There was also a notable proportion of parents (24%–27%) who said they were not sure how safe their communities' public recreation facilities were. This sample with low acculturation (BASH<2), may not have felt they had enough of an understanding of their environment to assess its safety. Furthermore, while the exposed and unexposed groups were interviewed within 5 months of each other, the difference in seasons may have influenced use of the CRC. More qualitative research on determinants of CRC use among Latino parents may provide additional insights.
Conclusions
As the world's children continue to face obesity earlier in life, ensuring that young children engage in routine physical activity could prevent this dangerous trajectory of obesity. Latino children are the fastest growing ethnic minority in the United States that bears the largest burden of childhood obesity.34,35 Our findings suggest that by exposing Latino families to CRCs through culturally tailored programming, communities could promote Latino families' use of CRCs for physical activity. Policy makers should be aware that offering programs that encourage families to “walk through the door” could be a promising strategy for helping Latino families with young children to better utilize their recreational built environment and promote health.
Footnotes
Acknowledgments
We would like to thank the staff and leadership of Metro Parks and Recreation in Nashville, Tennessee. We would specifically like to thank Stevon Neloms and his staff at the Coleman Community Recreational Center for their dedication to this project. We also thank Stephanie Mitchell and Evan Sommer for their time and efforts in contributing to manuscript editing.
This study was funded by the Robert Wood Johnson Foundation through its national program, Salud America!, the RWJF Research Network to Prevent Obesity Among Latino Children (![]() ). Salud America!, led by the Institute for Health Promotion Research at The University of Texas Health Science Center at San Antonio, Texas, unites Latino researchers and advocates seeking environmental and policy solutions to the epidemic. The study was also supported by the Vanderbilt CDTR through P30DK092986 from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), as well as by a Project Diabetes Implementation Grant from The State of Tennessee (GR-09-25517-00) awarded to S.L. Barkin and pilot funds awarded to S.L. Barkin from the Vanderbilt Clinical and Translational Science Award [National Center for Research Resources/National Institute of Health (NCRR/NIH)] (1 UL1 RR024975). S.B. Gesell was supported by the American Heart Association Clinical Research Grant Program (09CRP2230246). None of the funders contributed to the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
). Salud America!, led by the Institute for Health Promotion Research at The University of Texas Health Science Center at San Antonio, Texas, unites Latino researchers and advocates seeking environmental and policy solutions to the epidemic. The study was also supported by the Vanderbilt CDTR through P30DK092986 from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), as well as by a Project Diabetes Implementation Grant from The State of Tennessee (GR-09-25517-00) awarded to S.L. Barkin and pilot funds awarded to S.L. Barkin from the Vanderbilt Clinical and Translational Science Award [National Center for Research Resources/National Institute of Health (NCRR/NIH)] (1 UL1 RR024975). S.B. Gesell was supported by the American Heart Association Clinical Research Grant Program (09CRP2230246). None of the funders contributed to the design and conduct of the study; collection, management, analysis, and interpretation of the data; or preparation, review, or approval of the manuscript.
Author Disclosure Statement
No competing financial interests exist.