
Abstract
Abstract
Introduction:
The endocannabinoid system (ECS) regulates functions throughout human physiology, including neuropsychiatric, cardiovascular, autonomic, metabolic, and inflammatory states. The complex cellular interactions regulated by the ECS suggest a potential for vascular disease and stroke prevention by augmenting central nervous and immune cell endocannabinoid signaling.
Discussion:
The endocannabinoid N-arachidonoylethanolamine (anandamide) plays a central role in augmenting these processes in cerebrovascular and neurometabolic disease. Furthermore, cannabidiol (CBD), a nonpsychoactive constituent of Cannabis, is an immediate therapeutic candidate both for potentiating endocannabinoid signaling and for acting at multiple pharmacological targets.
Conclusion:
This speculative synthesis explores the current state of knowledge of the ECS and suggests CBD as a therapeutic candidate for stroke prevention by exerting favorable augmentation of the homeostatic effects of the ECS and, in turn, improving the metabolic syndrome, while simultaneously stalling the development of atherosclerosis.
Introduction
The study of cannabis and endocannabinoid biology has recently been identified as a priority by the National Academy of Medicine. 1 The extensive history of this medicinal plant has propelled the discovery of the human endocannabinoid system (ECS) and has opened a new therapeutic path for a multitude of disease states. Preclinical and human research has revealed the ECS to be pleiotropic and context-dependent regulator of stressed physiological states. Relevant to cerebrovascular neurology, the ECS has been shown to drive food intake and inhibit vascular inflammatory processes. This medical hypothesis suggests cannabidiol (CBD) as a therapeutic candidate for stroke prevention through its capacity to selectively augment and inhibit separate aspects of endocannabinoid biology simultaneously.
Endocannabinoid Physiological Effects
Endocannabinoids are arachidonic acid derivatives with widespread functions throughout physiology present in the central nervous system and circulation. The relevance of endocannabinoid function for stroke prevention will focus on two aspects known to be regulated by endocannabinoid function, neurometabolic balance, and vascular inflammation.
Neurometabolic balance
Observational evidence of the appetite-stimulating effects of herbal cannabis combined with knowledge of the pharmacological mechanisms of THC eventually identified dorsomedial, ventromedial, and lateral hypothalamic type 1 cannabinoid (CB1) receptors as a driver of reward-seeking behaviors, particularly food intake, reviewed by Cota et al. 2 CB1 receptors are described in the hypothalamus 3 and endocannabinoids have high affinity for CB1 receptors. 4 Administration of anandamide has been shown to stimulate appetite in mice. 5 Finally, CB1 inverse agonist has been shown to be a potent appetite suppressant in clinical trials and improve several cardiometabolic health measures.
Peripheral immune cell regulation
Two of the well-known endocannabinoids, anandamide and 2-arahidonoyl glycerol (2-AG), have different cellular responses at type 2 cannabinoid receptors. 2-AG increases migration in macrophage differentiated HL-60 cells, 6 human natural killer cells, 7 human B cells, 8 and human eosinophilic leukemic cells but not neutrophils. 9 Furthermore, 2-AG activates human umbilical vein endothelial cells promoting leukocyte migration by both CB1 and CB2 mechanisms. 10 Mutations in ABHD12, a gene that synthesizes the 2-AG degrading enzyme, have been linked to polyneuropathy, hearing loss, ataxia, retinitis pigmentosa, and cataract. 11
In contrast, anandamide exerts anti-inflammatory effects by decreasing tumor necrosis factor-alpha (TNF-α) and interferon-γ expression in human T cell cultures 12 and decreasing expression of interleukin (IL)-6, IL-12, and interferon-γ in prestimulated human dendritic cell cultures. 13 CB2 receptor agonists have also shown anti-inflammatory effects in cell culture models involving human astrocytes prestimulated with IL-1β, 14 human endothelium prestimulated with TNF-α, 15 and human T-lymphocytes 16 and neutrophils.
Endocannabinoid Response to Disease
Endocannabinoid receptors and their endogenous ligands are found to be altered in cardiovascular disease, hypertension, obesity, and diabetes. In congestive heart failure, human myocardial CB2 receptors are upregulated and CB1 receptors are downregulated, 17 which has been attributed to inverse expression of the suppressive miRNA regulation of CB1 and CB2 receptor transcription. 18 Elevated circulating levels of anandamide and cardiomyocyte CB2 receptor upregulation were present in both patients with aortic valve stenosis 19 and congestive heart failure. 17 Circulating levels of anandamide were significantly more elevated in humans with obstructive sleep apnea and diabetes when compared with controls and anandamide was also positively associated with increase in blood pressure. 20
Plasma endocannabinoid levels were positively correlated with elevations in blood pressure when depressed women were compared with nondepressed controls 21 and elevated in diabetic men 19 and obese postmenopausal women 22 and obese adults. 23 Circulating 2-AG but not anandamide was significantly increased in visceral obese humans and positively correlated with visceral fat area, and circulating 2-AG was inversely associated with insulin sensitivity, even when controlling for body fat percentage. Abdominal fat mass was associated with alterations in circulating endocannabinoids. 24 It is more likely that elevations in circulating endocannabinoids and altered CB1 and CB2 receptor expression are homeostatic reactions to the stresses of cardiac and metabolic syndrome disease states than primary causes of these disorders.
Both CB2 receptor agonists and antagonists have been reported to induce anti-inflammatory immune cell responses, the majority view is that peripheral immune CB2 receptor activation is anti-inflammatory. Furthermore, despite CBD having no pharmacological activity at the CB2 receptor, low doses of CBD appear similar to what is described with CB2 receptor activation in vitro and in vivo murine models of inflammation and atherosclerosis. Low dose THC arrests the development of a murine model of atherosclerosis through a CB2 receptor action. 25 Intraperitoneal coadministration of both proinflammatory lipopolysaccharide (LPS) and 2-AG nullified the TNF-α serum response normally provoked by LPS alone in a murine model of inflammation. 26
However, in murine experimental models of inflammatory pain, oral CBD doses as high as 20 mg/kg were not found to independently alter levels of TNF-α when compared with control. 27 Anandamide and 2-AG inhibit the CD14 and TLR4 proinflammatory pathway, and synthetic CB2 agonists also show this effect as well. 28 In vitro TNF-α stimulated human coronary arterial endothelial cell activation and monocyte adhesion was blocked by a CB2 receptor agonist. 15 Human macrophages laden with oxidized low-density lipoprotein (oxLDL or “foam cells”) are believed to promote the development of atherogenesis through a subendothelial proinflammatory process.
In vitro data obtained with human cell lines support a role for peripheral circulating macrophage CB2 receptor activation as an anti-inflammatory and antiantherogenic mechanism. 29 Human macrophages treated with a synthetic CB2 receptor agonist (JWH-015) were exposed to oxLDL in culture and were compared with controls. The central finding among the CB2-activated cell group was reduced levels of intracellular oxLDL, proinflammatory cytokine TNF-α, and IL-12. Interestingly, levels of 2-AG and anandamide were elevated in “foam cells” compared with controls. Is anandamide driving the formation of foam cells or responding to it? CB2 receptor agonist JWH-133 was shown to arrest TNF-α activation of human neutrophils in vitro by inhibiting phosphorylation of ERK1/2. The level of neutrophil collagen degrading enzyme matrix metalloproteinase-9 (MMP-9) is increased in areas of low CB2 receptor expression, marker of plaque instability.
In humans, CB2 receptor expression is decreased in symptomatic carotid plaques as compared with asymptomatic plaques. 30 Interestingly, it was later shown that CB1 receptor expression was undetected in human carotid plaque samples. 30 Thus, preclinical models of atherosclerosis offer a possible role for endocannabinoid signal modulation as a method for stalling the development of atherosclerosis through reduction of the inflammatory drivers of this process. To the authors' knowledge, the effects of ischemic and hemorrhagic stroke on circulating endocannabinoid levels have not been investigated to date.
Rationale for CBD in Cerebrovascular Disease Prevention
Cannabidiol
The scientific literature has described >65 molecular targets for the nonpsychoactive phytocannabinoid CBD, including receptors, ion channels, and enyzmes, and transporters. These molecular targets make CBD relevant for a host of neurological diseases; for a review on the molecular targets of CBD, see Bih et al. 31 Despite being named a cannabinoid, CBD has very low affinity for both CB1 (Ki: 1510 nM) and CB2 (CB2 Ki: 3612 nM) receptors and probably exerts no direct effect at CB2. Furthermore, CBD does not appear to exert a direct antagonist effect on CB1 receptors in pharmacological assays, yet CBD clearly shows “functional” antagonism of CB1 agonists, possibly through negative allosteric modulation.32,33 CBD increases circulating endocannabinoids through inhibition of fatty acid amide hydrolase (FAAH) 34 and competition for intracellular lipid catabolism.35,36 CBD potentiates anandamide by reuptake inhibition of the anandamide membrane transporter (AMT) in vitro although this finding is controversial and needs to be replicated in vivo. 37 CBD has demonstrated activation of peroxisome proliferator-activated receptor gamma (PPARγ), 38 adenosine A2A, 39 and 5-HT1a serotonin receptors. 40 CBD is subject to first pass hepatic metabolism and is a potent CYP inhibitor, including clopidogrel prodrug metabolizing enzyme CYP2C19. 31
Obesity
CBD is very likely a negative allosteric modulator of activated hypothalamic CB1 receptors exerting a homeostatic effect and reducing the strong hunger drive and improving weight loss. 32 CBD has shown to attenuate CB1 receptor agonist-driven food intake in a rat model of hyperphagia, although there was no difference in food intake seen with CBD in fed or fasting state rats. 41 In a recently published clinical trial investigating CBD for epilepsy, loss of appetite was reported in 28% of the treatment arm compared with 5% of the control arm 42 and is currently being investigated in clinical trials as a treatment for hyperphagia in the Prader–Willi syndrome. CBD differs completely from rimonabant in chemical structure, pharmacological mechanism, and safety, 43 therefore, CBD would not be expected to produce the serious neuropsychiatric effects seen with the rimonabant clinical experience. CBD may have relevance for the prevention of metabolic syndrome and insulin resistance through PPARγ agonism as reviewed by Kleiner. 44 Finally, the possible 5HT1a agonist effects may provide concurrent anxiolysis. 45 A potential mechanism for the appetite suppressive effects of CBD is shown in Figure 1.
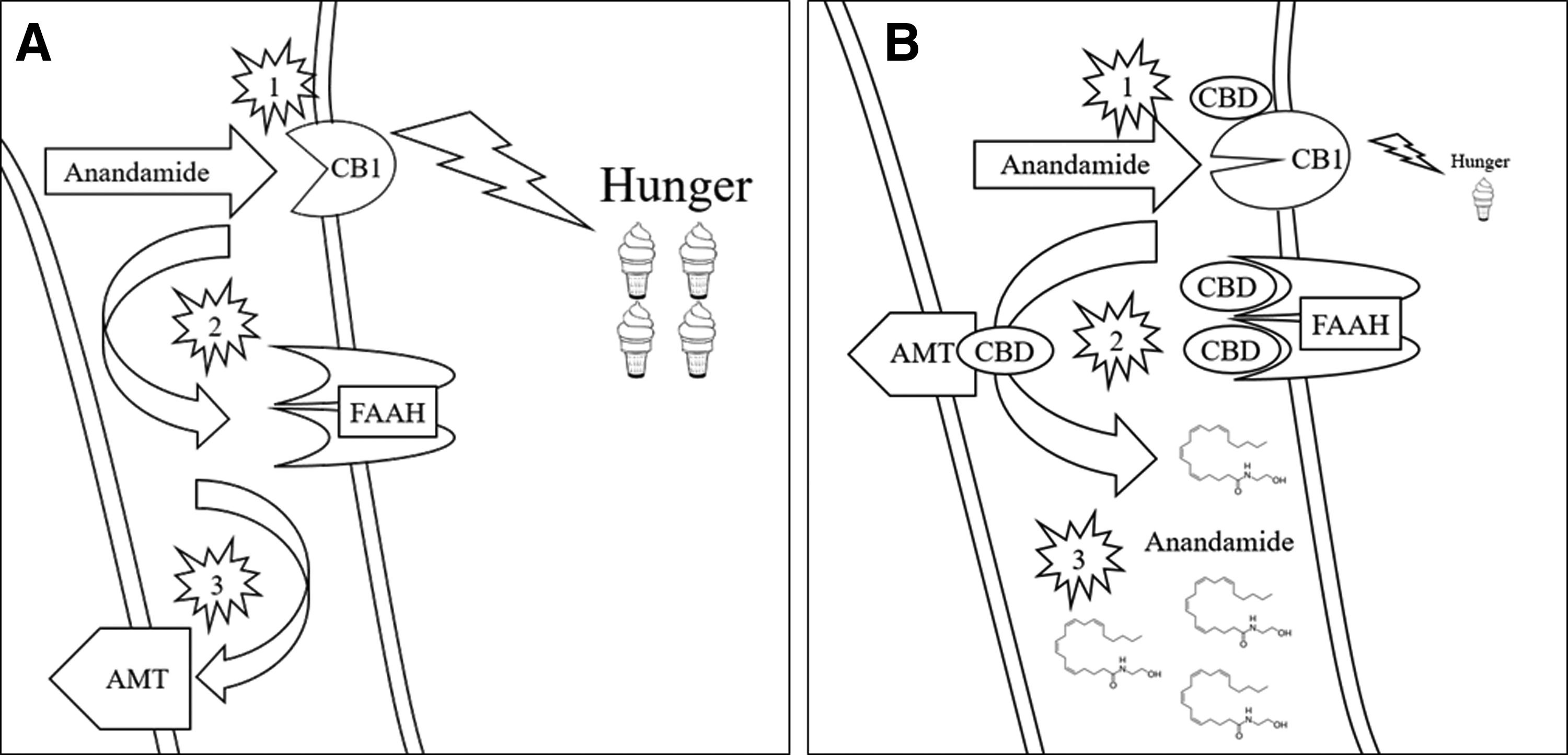
Effects of CBD on hunger signaling.
Atherosclerosis
CBD likely exerts an indirect effect on immune cell function by inhibiting the degradation of circulating endocannabinoids, thus increasing the availability to target type 2 CB receptors on neutrophils and macrophages in atherosclerotic plaques. CBD increases levels of the anti-inflammatory endocannabinoid anandamide but not proinflammatory 2-AG, 46 a finding that needs to be reproduced clinically. If present, this augmented “endocannabinoid tone” likely explains the finding of reduced IL-1β, IL-2, IL-6, and TNF-α in experimental conditions. Until synthetic CB2 receptor agonists become available for clinical trials, the established safety profile and putative mechanism support the investigation of CBD as a therapeutic for atherosclerosis.
Conclusion
The rationale for CBD as a therapy for stroke prevention is shown in Figure 2. There is now a therapeutic opportunity to examine the effects of CBD in atherosclerosis and obesity. Synthetic cannabinoid agents although possibly more potent would not necessarily have the pleiotropic effects ascribed to CBD in the scientific literature. 33 Although the role of endocannabinoids in cerebrovascular disease should be studied, a current hypothesis that must be explored clinically is whether CBD can functionally antagonize central CB1 receptors while simultaneously increasing availability of circulating endocannabinoids (particularly anandamide) to promote an antiatherogenic vascular effect. Therefore, a clinical trial investigating CBD in vascular disease and obesity would serve an immediate public health need and is a necessary next step in advancing stroke prevention.
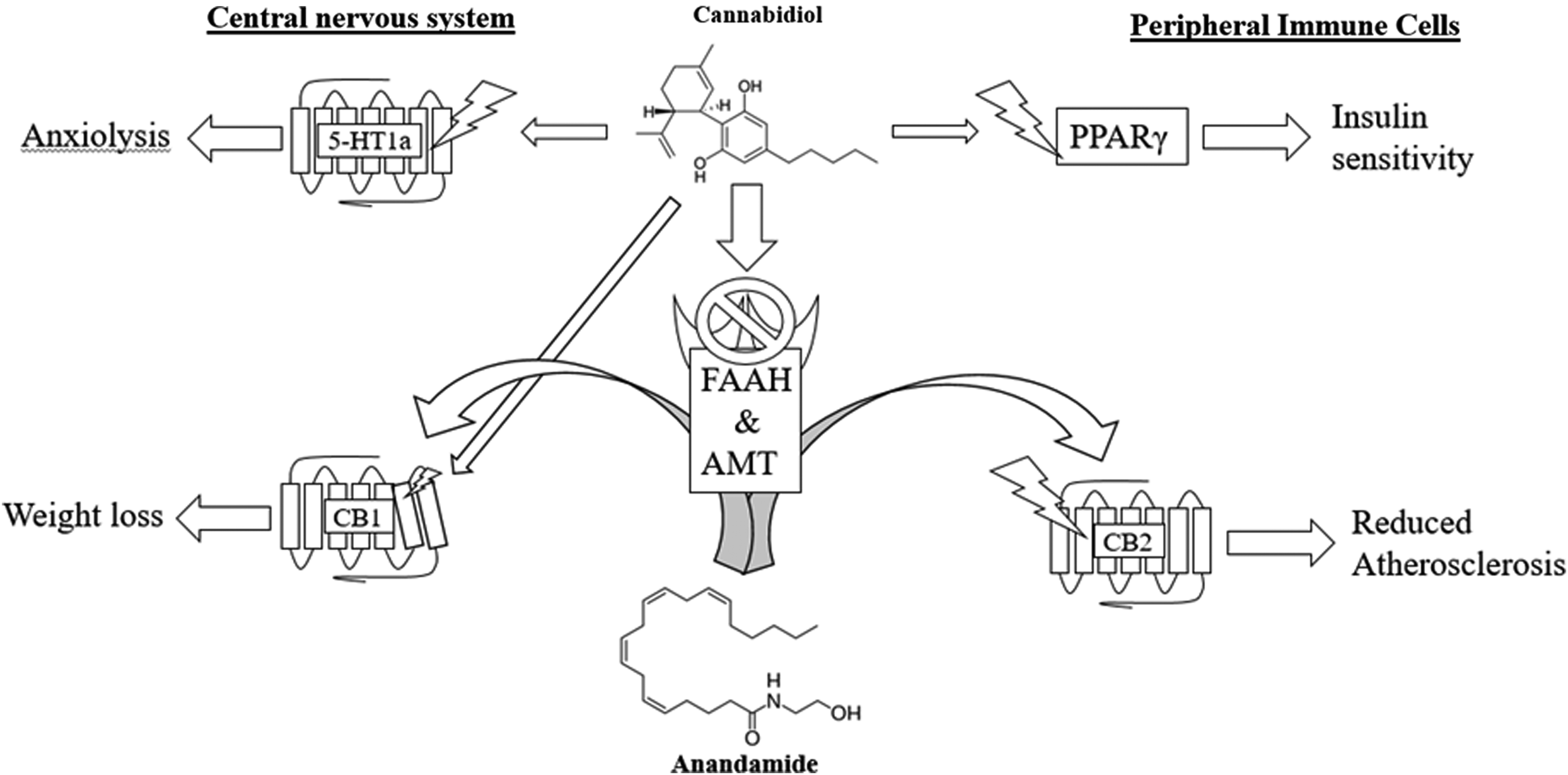
Direct and indirect effects of CBD on vascular and metabolic risk factors. CBD (center) increases circulating anandamide by inhibiting the catabolic enzyme FAAH and transporter AMT. Central nervous system (left): CBD promotes anxiolysis through 5-HT1a activation. CBD reduces hunger signaling through negative modulation of activated CB1 receptors. Peripheral immune cells (right): CBD activates PPARγ. Anandamide promotes CB2-mediated anti-inflammatory response, decreasing atherosclerosis on circulating neutrophils and lymphocytes. 5-HT1a, type 1a serotonin receptor; CB2, type 2 cannabinoid receptor; PPARγ, peroxisome proliferator-activated receptor gamma.
Footnotes
Author Disclosure Statement
No competing financial interests exist.