
Abstract
Disease surveillance networks in the Middle East, Southeast Asia, and Africa are models for the kind of transnational cooperation that can mount the needed flexible and coordinated response to the spread of 2009 H1N1 influenza and future pandemic threats. For example, members of the Middle East Consortium on Infectious Disease Surveillance (MECIDS), a regional disease surveillance network of public health experts and ministry of health officials from Israel, the Palestinian Authority, and Jordan, have coordinated the screening, laboratory testing, and risk communication strategies to detect and control 2009 H1N1 influenza. This coordination is made possible by trust and by well-exercised national and regional pandemic preparedness policies. The consortium illustrates the value of regional disease surveillance networks in shaping and managing cohesive policies on current and future threats. The MECIDS alliance partnership also exemplifies to other parts of the world that are experiencing conflict—like South Asia—that finding common ground is imperative to promoting health security and cooperation where it is most lacking and needed and that developing cohesive infectious disease control policies can build trust across the most difficult boundaries in the world. This article provides an overview of the history of MECIDS and similar networks and of the MECIDS response to 2009 H1N1 influenza.
Effective regional disease surveillance networks have the potential to support long-term health, stability, and security in a region and can be valuable mechanisms for under-resourced countries to collaborate on and coordinate capacity building. The Middle East Consortium on Infectious Disease Surveillance (MECIDS) has brought together public health experts and ministry of health officials from Israel, the Palestinian Authority, and Jordan to improve the region's ability to detect and respond to infectious disease threats. Regional partnerships in the form of disease surveillance networks also provide opportunities for countries to unify and coordinate to meet the core competencies and capacities required by the revised International Health Regulations (IHR) (2005). 2 *
With 2009 H1N1 influenza, neighboring states face new urgency and pressure to manage their responses within and across borders. As evidenced by the MECIDS response to the current pandemic, regional collaboration has been especially valuable for facilitating collaborative action—even in a region experiencing political conflict and with a challenged history of collaborative efforts on health issues—against a specific health threat. This article describes the history and current structure of MECIDS and provides examples of the network's collaboration; it discusses accomplishments, including the Bellagio Call for Action and Connecting Health Organizations for Regional Disease Surveillance (CHORDS), in developing regional disease surveillance networks in other regions, and it provides an overview of how the Middle East partnership has responded to 2009 H1N1 influenza.
Background of MECIDS
History and Structure
Drawing on an idea born at the height of the Second Intifada in 2002, the Nuclear Threat Initiative's (NTI) Global Health and Security Initiative (GHSI) collaborated with another international nongovernmental organization, Search for Common Ground, to facilitate the establishment of a regional disease surveillance network amid the historically divided governments of Israel, the Palestinian Authority, and Jordan. The network that developed from this initiative was MECIDS, which brought together public health experts and ministry of health officials in the region to improve the region's ability to detect and respond to infectious disease threats through coordinated surveillance and joint epidemiologic and laboratory training (Figure 1). Before the development of MECIDS in 2003, cooperative efforts on health matters in the region were scarce. By January 2007, MECIDS had formed its own executive board and secretariat, and it is now a self-governing body; the year-long rotating chair position is held by 1 of the 3 delegation heads to MECIDS (Figure 2). The members meet several times a year to discuss policies, such as regional avian influenza preparedness and national laboratory-based foodborne disease surveillance.

MECIDS Region. Color images available online at www.liebertonline.com/bsp.
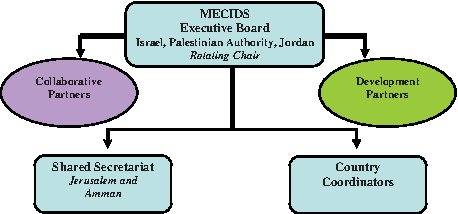
MECIDS Governance Structure. Color images available online at www.liebertonline.com/bsp.
MECIDS unites public health officials of differing Middle Eastern nationalities and contributes to regional health and stability by engaging in regular cross-border information exchange, conducting regular executive board meetings, performing laboratory and risk communication training, and implementing innovative communication technology. Initially focused on food- and waterborne diseases, the partnership developed a network of laboratories, protocols for specimen collection and diagnosis of diarrheal diseases, and data sharing and notification capabilities to analyze and share information on disease threats. Through these efforts, MECIDS has played an instrumental role in detecting significant outbreaks of mumps and salmonella. Priority diseases in the region now include influenza, leishmaniasis, mumps, salmonella, and shigella.
Examples of Collaborative Efforts
Leventhal et al. describe a successful case study highlighting that building relationships through joint efforts creates an infrastructure for cross-border collaboration during emergencies. 4 In response to an outbreak of avian influenza (H5N1) in 2006, the ministries of health of Israel, the Palestinian Authority, and Jordan coordinated preparedness plans and outbreak responses to mitigate the potential public health crisis. The H5N1 outbreaks in poultry crossed the borders of all 3 MECIDS member countries in under 10 days. However, the surveillance network's strategic planning and uniform response prevented human infection and created public confidence. Prompt reporting and sharing of information between Israeli and Palestinian contacts in the ministries of health and agriculture allowed Jordanian authorities to swiftly cull 20,000 birds in a 3-km protective zone and fully contain the avian flu outbreak. 4 After-action feedback from the MECIDS partners made clear that successful personal and working relationships fostered over years of cooperation had allowed transparent reporting and coordinated response and control measures to mitigate the impact of an outbreak of influenza.
The MECIDS partners invited representatives from the World Health Organization (WHO) to conduct a workshop on IHR (2005) implementation in November 2007. As a result of this workshop and supplementary joint meetings, the 3 partner countries developed a statement of understanding regarding the IHR procedures, which they are implementing as part of their national avian influenza preparedness plans.
In 2007 and 2008, MECIDS conducted a series of national pandemic influenza tabletop exercises to identify current gaps in preparedness and cross-sectoral cooperation and to develop a plan of priority actions to improve preparedness and response. In August 2008, the partners conducted a regional exercise to test, in particular, cross-border cooperation and procedures during the response to a pandemic. The regional exercise not only brought together the public health experts and ministry of health officials from the MECIDS countries, but the exercise also engaged representatives from multiple sectors in the 3 countries, including transportation, education, interior, laboratory, and media. These exercises were conducted with cooperation and observers from WHO Geneva and WHO's Eastern Mediterranean and European Regional Offices and the Turkish Ministry of Health.
MECIDS's Response to 2009 H1N1 Influenza
On April 29, 2009, in response to H1N1 influenza outbreaks throughout the world, WHO Director-General Dr. Margaret Chan raised the influenza pandemic alert from Phase 4 to Phase 5 and spoke of the opportunity for global solidarity to address the pandemic. Surprising to some, 2 days earlier, a group of Israeli, Palestinian, and Jordanian health officials had already held an emergency teleconference to discuss a joint plan of action to mitigate the spread of the disease.
Since mid-April 2009, WHO and the U.S. Centers for Disease Control and Prevention (CDC), along with national and local health officials, have been responding to the emergence of the novel influenza virus, 2009 H1N1. In a July 6 situation update, the United States reported 33,902 laboratory-confirmed cases and 170 deaths, while the MECIDS region reported 704 cases (Israel 681, Jordan 23) and no deaths. By September 2009 the number of laboratory-confirmed cases in the MECIDS region swelled to more than 4,000 with 32 deaths. Notably, H1N1 cases occurred at the same time as the diagnosis of new cases of avian influenza H5N1 in Egypt. The concern that H1N1 and H5N1 could combine into a new virus with potential spread around the world was reflected by Dr. Chan: “We have no idea how H5N1 will behave under the pressure of a pandemic.” 5 For this reason, effective and coordinated regional surveillance to monitor and mitigate the spread of infectious disease in the Middle East region was critical.
On July 16, 2009, WHO acknowledged that further spread of the pandemic was inevitable within affected and new countries and referenced the July 6 report showing a case count of 94,512 laboratory-confirmed cases of 2009 H1N1 influenza and 4,591 deaths. 6 WHO now acknowledges that individual case counting is no longer essential to characterization of the spread or nature of the risk. 7
MECIDS had been preparing for an event like this for some time. In response to H1N1 cases in Israel, the partners held emergency meetings and agreed to prompt and coordinated border and airport screening, laboratory testing, information exchange, and common communication strategies. This coordination was in large part due to the existence of trust and to well-exercised national and regional pandemic preparedness plans. Representatives from Egypt, which is not formally a member of MECIDS, also participated in these discussions.
On April 29, 2009, 2 days after WHO raised the pandemic threat level to Phase 4, the 3 principals of the MECIDS Executive Board initiated a teleconference to discuss suspected H1N1 cases in Israel and the cooperative measures that needed to be taken for MECIDS countries to prepare for a serious outbreak in the region. The partners discussed availability of antivirals and border issues and convened an in-person emergency meeting to discuss these and other issues in more detail. According to Dr. Alex Leventhal of Israel, a MECIDS Executive Board member, there is a common interest among members of this group: “For instance we have decided we have to upgrade the lab capabilities of the three countries. The organization has bought diagnostic equipment for the Palestinian Authority and Jordan and we've studied together. Now the same type of machine [for testing H1N1] will be used in all three countries.” 4 About the partnership, Leventhal said: “If one country is stronger, the others will get more in order to harmonize.” 8
Table 1 outlines specific MECIDS activities categorized by the early WHO H1N1 pandemic phases. Since the shift to Phase 6 on June 11, 2009, the MECIDS principals have discussed H1N1 measures ahead of the annual Hajj pilgrimage in November 2009, in anticipation of the threat that the event will facilitate the spread of 2009 H1N1 influenza among the several million Muslim pilgrims en route to Mecca, Saudi Arabia.
Networks in Other Regions and the Bellagio Call for Action
The value of regional infectious disease surveillance networks has also been demonstrated in other regions of the world. For example, in 1999, with support from the Rockefeller Foundation, delegates from ministries of health in 6 Mekong Basin countries agreed to collaborate on disease surveillance and outbreak management through the Mekong Basin Disease Surveillance (MBDS) network. The 6 countries were Cambodia, Yunnan and Guanxi Provinces of China, Laos, Myanmar, Thailand, and Vietnam. MBDS, like MECIDS, conducted national and regional pandemic influenza tabletop exercises that were designed to foster cooperation among MBDS countries and to identify gaps and weaknesses in systems for detecting, monitoring, tracking, and containing disease. As a result of these exercises, MBDS developed a 6-year action plan to strengthen weaknesses and fill gaps. Together, these countries are working to build capacities to fulfill their obligations under the IHR (2005).
In addition, within 6 months of the IHR (2005) becoming legally binding in June 2007, GHSI, also with funding support from the Rockefeller Foundation, explored an innovative approach to building and sustaining an effective international public health capacity. Public health leaders from Africa, the Americas, Asia, Europe, and the Middle East gathered in Bellagio, Italy, in December 2007 to share best practices and lessons learned and to recommend action to advance the global capacity for public health surveillance. Representatives from MECIDS, MBDS, the Pan American Health Organization (PAHO), and the East African Community (EAC) shared their experiences of working in regional disease surveillance networks.
Because an advantageous approach to including health as an integral part of foreign policy may be through NGO collaboration via public-private partnerships,9-11 the conference yielded a Call for Action to governments, international government organizations, and private foundations that emphasized innovative ideas, committed partnerships, and sustained engagement to bolster infectious disease surveillance in developing countries. 12 The Bellagio Call for Action spurred the development of a southern African network, the Southern African Centre for Infectious Disease Surveillance (SACIDS). GHSI helped to establish SACIDS, which is a multidisciplinary, multisectoral (one health) network comprised of members from the Democratic Republic of Congo, Mozambique, South Africa, Tanzania, and Zambia. GHSI facilitated communication between SACIDS principals and key MECIDS and MBDS network representatives to help develop an appropriate governance framework for SACIDS.
The sensitive nature of local political, economic, and social conditions existing within regions reinforces the notion that successful partnerships focus on mutual interests that will produce net benefits to all partners. Governance arrangements for disease surveillance networks do not have a “one size fits all” model; flexibility is paramount in creating these public-private partnerships. The arrangement could range from an informal memorandum of understanding to a more formal legal architecture outlining codes of conduct and formal partnerships. Experiences shared at the Bellagio conference showed that the investment in building trust between collaborating partners is an essential ingredient for success. To help implement the Call for Action, GHSI has launched a process called CHORDS: Connecting Health Organizations for Regional Disease Surveillance. Through CHORDS, which has a particular emphasis on developing countries, GHSI is creating a mechanism to connect the capacities of regional networks and strengthen partnerships between existing and nascent networks for early detection and response.
Conclusion
Emerging and reemerging diseases have increased the need for novel surveillance capabilities to promote collaboration across sectors and country borders to ensure early identification and rapid response to disease outbreaks, which are crucial to the prevention of pandemics. Through a regional approach, under-resourced countries are able to work with their partners to collaborate on and coordinate capacity building to fulfill obligations under the IHR (2005). Joint preparedness plans and regular communication between partners enhances each country's capacity for infectious disease surveillance.
MECIDS, which serves as an example of cross-border collaboration against shared vulnerabilities to infectious disease threats in regions of conflict, has inspired the development of surveillance networks in other regions of the world. A remarkable level of trust has been built between senior officials and ministers through the cross-border collaborations that cut across the security, defense, foreign affairs, health, agricultural, and environmental sectors, reinforcing the notion that intersections among foreign policy, health security, and the need for mutual action create a powerful synergy.9-11 A shared threat, such as 2009 H1N1 influenza, provides countries with a unique opportunity to extend the proverbial olive branch and focus on humanitarian matters for the common good of all bordering countries. 4
Important lessons from the Middle East partnership that can be readily translated to the global community include the following:
The trust built through developing collaborative action plans has proven its worth across one of the most difficult boundaries in the world. Neighboring countries facing common infectious disease threats can successfully build operational collaborative surveillance networks to strengthen public health capacity and to help meet their international legal obligations. A regional or subregional network with a common plan to improve its capacities can collectively generate funding and expert support that responds directly to the most urgent needs. Sharing experience, innovative approaches, and best practices associated with regional networks can contribute to enhancing the overall global capacity for infectious disease surveillance.
The MECIDS alliance is a model for other parts of the world experiencing conflict to find common ground and promote health security and cooperation where it is most lacking and needed. It demonstrates that even in the most politically challenged regions, effective regional disease surveillance networks can support long-term health, stability, and security in a region and can serve as vehicles for under-resourced countries to collaborate and coordinate policies on early detection and response to outbreaks. MECIDS has shown that, even in difficult political contexts, the pursuit of effective disease surveillance and response must be realized to protect public health security.13,14 Clearly, a connected framework of regional disease surveillance networks is influential in the evolution of global health policy. 15 This may be tested soon as countries face further limited resources in combating 2009 H1N1 influenza.
Footnotes
Acknowledgment
Data in this manuscript were collected by the Middle East Consortium on Infectious Disease Surveillance (MECIDS). MECIDS is funded by the Nuclear Threat Initiative, with additional supplemental funding from the World Bank.
*
The IHR (2005), which entered into force on June 15, 2007, is an international legal instrument that is binding on 194 countries across the globe, including all WHO Member States. The IHR (2005) apply to new and ever-changing public health risks and have long-lasting relevance in the international response to the emergence and spread of disease, offering legal interpretations relevant to international airports, ports, and ground crossings. The most important norm in the IHR is the strengthening of national capacities for surveillance, control, and response. 3 These capacities for achieving international health security are being tested as the spread of 2009 H1N1 influenza has reached pandemic proportions, with WHO raising the worldwide pandemic alert level to Phase 6 in response to its global spread. While not party to the IHR (2005), the Palestinian Authority works with MECIDS partners to meet requirements under IHR (2005).