
Abstract
Healing of rotator cuff (RC) injuries with current suture or augmented scaffold techniques fails to regenerate the enthesis and instead forms a weaker fibrovascular scar that is prone to subsequent failure. Regeneration of the enthesis is the key to improving clinical outcomes for RC injuries. We hypothesized that the utilization of our tissue-engineered tendon to repair either an acute or a chronic full-thickness supraspinatus tear would regenerate a functional enthesis and return the biomechanics of the tendon back to that found in native tissue. Engineered tendons were fabricated from bone marrow-derived mesenchymal stem cells utilizing our well-described fabrication technology. Forty-three rats underwent unilateral detachment of the supraspinatus tendon followed by acute (immediate) or chronic (4 weeks retracted) repair by using either our engineered tendon or a trans-osseous suture technique. Animals were sacrificed at 8 weeks. Biomechanical and histological analyses of the regenerated enthesis and tendon were performed. Statistical analysis was performed by using a one-way analysis of variance with significance set at
Introduction
Rotator cuff (RC) tears are one of the most common orthopedic disorders in the United States, with more than 200,000 repair procedures performed annually. 1 Tears of the RC tendons often fail to heal without intervention and are frequently the cause of significant shoulder pain and impaired shoulder function. 2 Current repair techniques utilize an open or arthroscopic suture technique to reattach the tendon to bone. Failure rates, however, especially in full-thickness large (3–5 cm) or massive tears (>5 cm, 2 tendons), are unacceptably high (20–94%).2,3 Factors including tendon retraction, muscle atrophy, and fatty infiltration have been known to limit the successfulness of the repair.4–7 In addition, healing of the enthesis with current techniques often results in a notably weaker fibrovascular scar rather than a normal enthesis architecture and may explain the high prevalence of repair failures. 8
The native enthesis consists of a compositionally and mechanically graded fibrocartilage transition zone that is designed to minimize stress concentrations at the tendon-bone interface. Using a rat supraspinatus RC model, Thomopoulos et al. demonstrated that the biology and zonal arrangement of the enthesis is not regenerated after RC repair. 9 Rather, a sharp boundary was observed, with disorganized collagen fibers and a fibrocartilaginous region, representing a significant deviation from the native enthesis anatomy. The regeneration of a structurally sound enthesis with normal biomechanics is paramount for improving functional outcomes and reducing the risk of recurrent structural failure after the repair of RC injuries. As such, several tissue-engineering approaches are being developed to improve the regeneration of the enthesis after the repair of RC tears.
To date, there are several commercially available extracellular matrix (ECM) scaffolds being tested clinically to improve enthesis repair after RC repair. 10 Although the biochemical properties of these scaffold materials have the potential to modulate host response and influence enthesis repair, the structural properties degrade over time and often do not match the rate of new ECM regeneration. In addition, these ECM scaffolds often fail to regenerate the fibrocartilage gradient at the enthesis, leading to stress points and weaker connections to the bone. Thus, alternative strategies are needed to improve enthesis regeneration after RC injuries.
Recently, stratified and functionally graded scaffold-based approaches have been developed to engineer the native tendon-to-bone interface
To address the concerns of scaffold-based approaches, our lab has developed a scaffold-less tissue-engineered tendon construct that relies on
Although the results of these studies are encouraging, it is unclear as to whether we can extrapolate these findings to an RC injury model. Thus, the objective of this study was to evaluate the efficacy of our scaffold-less tendon constructs to regenerate the native-like structure of tendon and the mechanical strength of the enthesis in both acute (immediate repair) and chronic (repair 4 weeks post-injury) supraspinatus tears in a rat model. We hypothesized that utilization of the tissue-engineered tendon construct would better regenerate the fibrocartilage transition zone, collagen organization, and tendon attachment strength of the native enthesis in both acute and chronic tear repairs compared with suture repair alone.
Materials and Methods
Animal model and design
Female Fisher 344 rats, approximately 150–200 g in mass, were obtained from Charles River Laboratories, Inc. All animals were acclimated to colony conditions for 1 week before any procedure. Animals were fed Purina Rodent Chow 5001 and water
For recreating an acute supraspinatus tendon tear, the supraspinatus tendons of the right shoulders underwent a full-thickness tenectomy from the humerus by using a transacromial approach
16
and were then immediately repaired with either a Mason-Allen suture technique (suture repair group) or a modified trans-osseous technique utilizing a tissue-engineered tendon construct (construct repair group). Chronic tears of the supraspinatus tendon were created by severing the supraspinatus tendon from the humerus and then encasing the detached end of the tendon in silicone tubing. The animals were then allowed to recover for 4 weeks with the detached tendon. The encasement with the silicone tubing prevented attachment to the surrounding connective tissue so that the cut end of the tendon could easily be identified and repaired at a later date. The contralateral shoulders were used as non-surgical controls for each treatment group. Next, the chronic tendon tears were repaired with either a Mason-Allen suture technique (suture repair group) or a modified trans-osseous technique utilizing a tissue-engineered tendon construct (construct repair group). At 8 weeks after repair of the tendon, animals were euthanized (
Preparation of solutions and media
Media were prepared, as previously described, with slight modifications.15,17 Growth medium (GM) consisted of Dulbecco's modified Eagle's medium (DMEM; Gibco, Cat# 10565-042) supplemented with 20% Fetal Bovine Serum (FBS; Gibco, Cat# 10437-028), 2% antibiotic-antimycotic (Sigma; Cat# A9909), 600 ng/mL bFGF, and 40 ng/mL dexamethasone. Differentiation medium (DM) consisted of DMEM supplemented with 7% Horse Serum Albumin (HS; Gibco, Cat# 16050-122) and 2% antibiotic-antimycotic, plus the addition of 0.13 mg/mL ascorbic acid-2 phosphate, 0.05 mg/mL L-proline, 400 ng/mL dexamethasone, and 2 ng/mL transforming growth factor-beta (TGF-β; Peprotech, Cat# 100-21).
Bone marrow isolation and cell expansion
Bone marrow stromal cells were isolated and expanded according to a previously described protocol.15,17 Briefly, rat femora were removed from the animal and cut at the proximal and distal metaphysis. The marrow contents were extracted through centrifugation (900
Preparation of self-organized tendon constructs
Methods for creating scaffold-less three-dimensional tendon/ligament tissues have been previously described.14,15,17 Briefly, mesenchymal stem cells (MSCs) were plated onto 100 mm cell culture dishes at 21 × 103 cells/cm2 and suspended in 8 mL of GM supplemented with 0.13 mg/mL ascorbic acid-2 phosphate and 0.05 mg/mL L-proline. The dishes were placed in a 37°C, 5% CO2 incubator and medium was changed every 2–3 days. After approximately 5 days, the cells became confluent and DM was substituted for GM to induce monolayer delamination. As the monolayer delaminated, it was transferred to a Sylgard coated dish and constrained between two minutien pins that were placed approximately 60 mm apart. The monolayer was fully self-assembled into a 60 mm-long cylindrical construct within 1–2 days. One week after delamination, constructs that were approximately 0.9 mm in diameter were cut into 6 mm-long segments for use in RC repairs. The medium was again changed every 2–3 days until the construct was used for implantation.
Surgical technique
Rats were anesthetized by using 2% isoflurane, and the right shoulder was shaved and scrubbed with povidone iodine. An incision was made from a point 2–3 mm distal to the head on the humerus to approximately 5 mm proximal along the deltoid muscle. The deltoid muscle was cut longitudinally to expose the supraspinatus muscle. The acromion was cut and moved to expose the enthesis of the supraspinatus on the humeral head. The supraspinatus was isolated, and the tendon was sharply released from the bone at the enthesis. For acute suture repairs, two 0.6 mm crossing tunnels were drilled into the greater tuberosity footprint. A 4–0 Vicryl suture (Ethilon) was used to suture the detached supraspinatus tendon back onto its original insertion point. For the acute construct repairs, a 0.9 mm bone tunnel was drilled directly through the middle of supraspinatus insertion footprint and guided out to the lateral aspect of the humeral head. A tissue-engineered graft (∼6 mm in length) was pulled into the bone tunnel and anchored to the periosteum on the lateral aspect of the humerus with 9–0 silk sutures (Ethilon) (Fig. 1).

Tissue-engineered construct inserted into humeral bone tunnel during repair of acute rotator cuff tear. Scale bar represents 5 mm.
A small hole was made in the remaining supraspinatus tendon with #5 forceps and the construct was pulled into the hole, such that the graft lay on the posterior aspect of the tendon. The end of the construct was sutured to the supraspinatus tendon with 9–0 silk sutures. The deltoid and biceps muscle were closed by using 7–0 sutures, and the skin was closed with staples. Animals were fed
Biomechanical testing
Biomechanical testing was performed on freshly dissected supraspinatus tendons while they were still attached to the humerus. Before testing, the supraspinatus muscle belly was carefully removed from the supraspinatus tendon and the cross-sectional area of the tendon was measured by using a digital micrometer. To prevent the fracture of the humeral physis during mechanical testing, the humerus was potted with polymer into a custom-designed grip. The specimen was then placed into a Dynamic Mechanical Analyzer (RSA-III; TA Instruments) and aligned in the native joint flexion angle for uniaxial tensile testing. The end of the tendon was secured to a screw grip by using sandpaper and cyanoacrylate. The specimen was attached to a 35 N load cell and aligned uniaxially. The specimen was loaded to failure at a rate of 0.3 mm/sec or approximately 0.10/sec. Samples were tested at room temperature and were continuously moistened via a PBS drip throughout testing. The ultimate load to failure and location of failure (enthesis or tendon mid-substance) were recorded. The stiffness for each specimen was calculated from the linear region of the load-deformation curve. Statistical analysis was performed by two-way analysis of variance (ANOVA), with significance as
Histomorphometric analysis
After recovery, the supraspinatus tendon with the humerus still attached was carefully dissected from the surrounding tissue under a microscope, leaving the supraspinatus muscle intact. After dissection, samples were fixed in 10% neutral buffered formalin for 48 h, decalcified in EDTA for 48 h, and, subsequently, washed in phosphate-buffered saline solution. The samples were dehydrated and embedded in paraffin for sectioning. To facilitate comparisons between groups, an orientation of 90° between the humerus and supraspinatus muscle was maintained for each sample during embedding. Serial sections that were 12-μm thick, containing the repaired tendon and greater tuberosity of the humerus, were cut in the coronal plane and stained with picosirius red, safranin-O, and hematoxylin and eosin (H&E). Using an Olympus B light microscope, digital images of the stained slides were taken by using a SPOT RT camera (Diagnostic Instruments). Five representative slides for each stain and specimen were prepared. Each slide was evaluated by using polarized and non-polarized light and analyzed by three different people.
To evaluate collagen organization in the repaired tendon enthesis, sections stained with picrosirius red were imaged under monochromatic polarized light. The birefringence of collagen fibers was semi-quantitatively analyzed, based on brightness, to determine differences in collagen deposition and maturation at the site of repair.18,19 Five representative tissue sections across the full width of the tendon-bone interface were analyzed for each shoulder. The polarization plane was rotated until maximum brightness was obtained to account for variations in specimen orientation on the slide. Digital images were taken of each tissue section at ×10 magnification during a single imaging session under identical imaging parameters. The images were imported into Image J software and underwent 8-bit digitalization. Non-collagenous material was shown as black (zero), and collagenous material was assigned a gray-scale value from 1 to 255. Higher gray-scale values signify more organized and mature collagen. Using the Image J software, ten rectangular areas (50 × 50 μm) were randomly selected in the tendon directly adjacent to the tendon-bone interface. Mean gray-scale values for each region were averaged for each specimen to obtain a brightness value. Statistical analysis of specimen brightness was performed by two-way ANOVA, with
The area of fibrocartilaginous material at the tendon-bone interface was assessed by use of safranin O-stained sections. Safranin O stains sulfated proteoglycans reddish-purple, a property referred to as metachromasia. Digital images of the stained sections were imported into Image J, and areas of metachromasia were meticulously outlined and measured by using the Image J software at a ×4 magnification (National Institutes of Health). Measured areas were averaged for suture- and construct-repaired shoulders and contralateral controls. Statistical analysis of the total area of fibrocartilage was performed by two-way ANOVA, with
Results
Gross morphology
At the time of necropsy, there was continuity between the tendon and bone in all of the acute and chronic repairs, with no detectable differences between groups. All animals appeared healthy and showed no signs of infection, or a negative immune or inflammatory response to the implanted graft. The cross-sectional area of the enthesis was measured and was not significantly different between the acute and chronic injury repairs (3.4 ± 0.8 mm2).
Biomechanical testing
A minimum of five samples for each treatment group was tested uniaxially until failure. In the acute injury repair groups, four of the suture-repaired specimens (
After 8 weeks of recovery, acute and chronic injuries repaired with either suture or construct techniques displayed no differences in stiffness between groups. All repair groups were significantly less stiff than their respective contralateral shoulders and not significantly different from each other (Fig. 2A). The mean stiffness of the tendon-bone interface in the acute injury repair groups was as follows: contra-lateral (23.2 ± 1.5 N/mm,
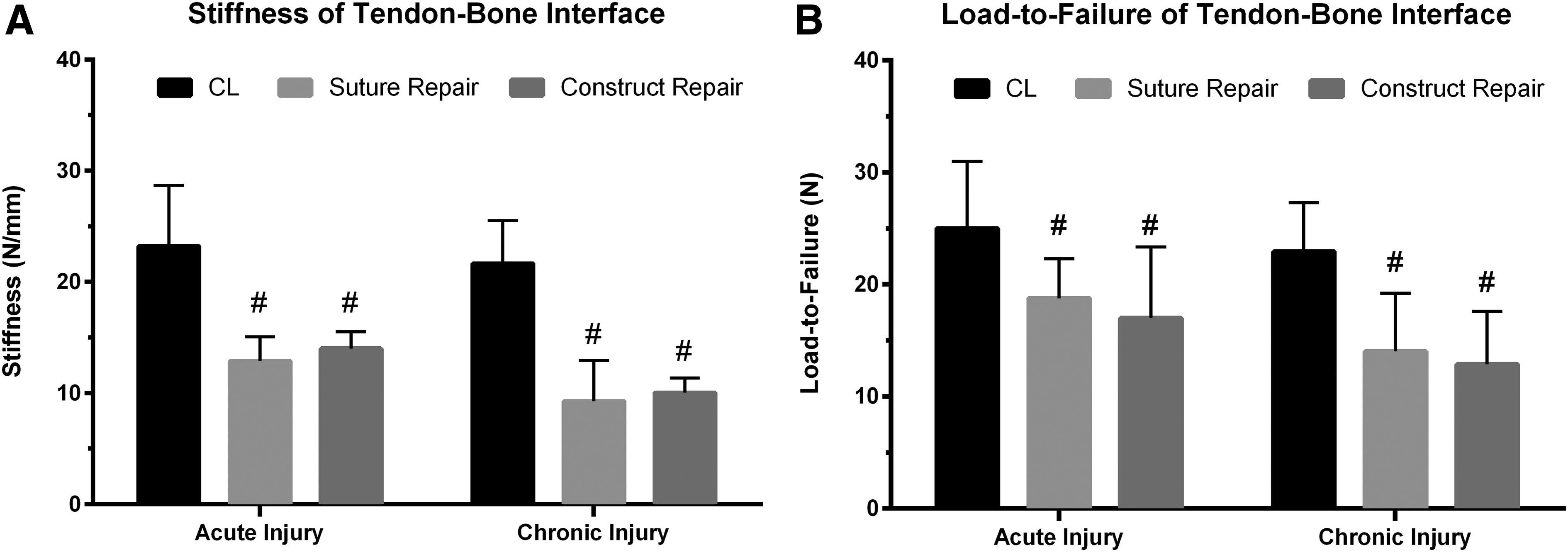
Mechanics of tendon-bone interface after acute and chronic injury repair.
The maximum load to failure was not significantly different between the acute and chronic repair groups with either suture or engineered tendon constructs. Each group was significantly less than its respective non-operative contralateral shoulder and not significantly different from the other repair groups (Fig. 2B). The maximum load to failure for acute injury repair was as follows: contra-lateral (25.0 ± 1.7 N,
Histomorphometric analysis
Collagen birefringence was semi-quantitatively analyzed, based on brightness, to evaluate collagen organization at the tendon-bone interface. Five specimens were analyzed for each treatment group. Contralateral shoulders of acute and chronic injured shoulders were not significantly different and were combined for analysis. Suture- and construct-repaired shoulders, although significantly more disorganized (shown in picrosirius red staining) than contralateral shoulders, were not significantly different from each other in either acute or chronic injury groups (Fig. 3). In addition, although repaired chronic injuries trended toward lower gray-scale values, no significant difference in collagen organization was observed between acutely and chronically injured shoulders. Suture repairs of acute injuries had a mean brightness gray-scale value of 70 ± 1 gray-scale units, whereas construct repairs had a gray-scale value of 70 ± 4 gray-scale units. Chronic injuries repaired with suture and construct techniques had gray-scale values of 58 ± 5 and 65 ± 4 gray-scale units, respectively. Non-operative contralateral shoulders had an average brightness value of 95 ± 6 gray-scale units. Representative images from each treatment and control group can be seen in Figure 4.

Collagen organization at enthesis after acute and chronic injury repair. No significant differences were observed between acute and chronic injury groups. (#) Denotes statistical significance compared with CL shoulder (

Representative collagen organization of enthesis.
The area of new fibrocartilage formation was evaluated at the enthesis by determining the area of metachromasia of safranin O-stained sections. Five specimens were analyzed for each treatment group. Contralateral shoulders of the acutely and chronically injured animals were not significantly different and were combined for analysis. The enthesis, after suture and construct repair of acute and chronic injuries, had significantly less fibrocartilage area than the native contralateral enthesis (Fig. 5). No significant difference in area of fibrocartilage formation was observed in acute injury suture or construct repairs. The area of fibrocartilage formation in the chronic injury group was significantly less in suture-repaired specimens compared with both construct-repaired specimens and unrepaired, contra-lateral shoulders. The total area of metachromasia, or area of fibrocartilage, for each treatment group was as follows: contralateral shoulders (109,905 ± 5095 μm2), acute suture repairs (52,571 ± 10,451 μm2), acute construct repairs (67,063 ± 11,455 μm2), chronic suture repairs (11,272 ± 6707 μm2), and chronic construct repairs (40,432 ± 7600 μm2) (Fig. 5). Representative images from each treatment and control group can be seen in Figure 6.

Fibrocartilage formation at the enthesis after acute and chronic injury repair. Suture repair of chronically injured shoulders had significantly less fibrocartilage formation compared with both contralateral shoulder and construct repaired specimens. No significant differences were observed between acute and chronic injury groups. (#) Denotes statistical significance compared with CL shoulder (

Representative fibrocartilage formation at enthesis. Representative images of safranin O stained
H&E staining of the tendon-bone interface allowed for qualitative evaluation of the entheses repair. Acute and chronic tendon injuries repaired with suture had less area of fibrocartilage formation and fewer organized collagen fibers than both construct-repaired and contralateral shoulders. The attachment of tendon to bone utilizing our tissue constructs resembled a more organized, native appearance. Suture-repaired shoulders in both acute and chronic injury models had a more abrupt, fibrous interface at the tendon-bone transition site, especially in suture-repaired specimens of chronic injuries. Representative images from each treatment and control group can be seen in Figure 7. There was no significant difference in the regeneration of the bone in the bone tunnel after repair with a construct or suture.

Representative structure at enthesis. Representative images of H&E stained
Discussion
Tissue engineering to improve the architecture and structural integrity of the regenerated enthesis after RC repair offers future promise to improve outcomes in patients. Engineered tendon constructs were used in this study based on their ability to specifically regenerate the enthesis in an ACL repair model. 14 The objectives of this current study were to evaluate the efficacy of our scaffold-less tissue-engineered tendon construct to regenerate the enthesis of the supraspinatus tendon after full-thickness tears in an acute and chronic RC injury model in a rat. Furthermore, we tested the hypothesis that RC repair utilizing our scaffold-less tendon construct will improve the regeneration of the enthesis, improve collagen organization and fibrocartilage formation compared with suture fixation alone.
In the acute injury repair model, our results demonstrate that there were positive effects with the utilization of our scaffold-less tendon construct. Although no significant differences in biomechanical integrity were observed, tissue failure occurred more frequently at the enthesis in suture-repaired, acutely injured shoulders. Histologically, qualitative differences in enthesis morphology revealed more native histological architecture by 8 weeks post-operatively. However, no quantitative differences were observed in enthesis structure. Although no overall difference in the total proteoglycan content was observed between the groups (Fig. 6), there were areas of differing densities of proteoglycans. Han et. al have shown that micro-domains of proteoglycan density can have significant effects on micromechanics and, in turn, effects on the native tissue biomechanics. 20 It could be that this variation in the density observed in the enthesis region of the different repair modalities explains the overall variation in tissue mechanics.
In tendons with chronic injury, repairs utilizing our tissue-engineered tendon construct resulted in a more native-like enthesis. Despite similar biomechanical properties with load-to-failure testing, suture-repaired specimens of chronic injuries failed more frequently at enthesis. However, the structure enthesis repaired with a tendon construct appeared qualitatively more native like in appearance and quantitatively more fibrocartilage was observed at the enthesis compared with suture repairs.
The formation of fibrocartilage at enthesis has an important role in the force transmission and energy dissipation between two tissues with vastly different properties. This complex tendon-bone interface is seldom recreated with current suture fixation techniques and often results in repair failure. The healing of the enthesis after repair is influenced by mechanical cues. In separate studies performed by Galatz et al., and Hettrich et al., complete removal of load after repair via immobilization and botulinum toxin application to supraspinatus muscles resulted in decreased structural properties and decreased ECM production at the tendon-bone interface.21,22 As such, suture techniques that rely on rigid mechanical fixation of tendon to bone may impede signals that may be necessary for proper enthesis regeneration, resulting in a more fibrous tissue interface. The unique ability of our initially compliant tendon construct to sense and respond to local mechanical cues and biological factors has led to improved structure and fibrocartilage formation at the enthesis.
The biological composition of our graft may also contribute to repair of enthesis. Recent research has shown that application of MSCs, with or without the addition of tendon growth factors, can enhance tendon to bone healing.
23
Our constructs are fabricated from MSCs and driven toward tendon lineage, via the addition of previously described growth factors. As such, enthesis regeneration at a repair site may be due to the unique cellular and molecular signals provided by the cells of our construct that are necessary for facilitating the proper host-mediated response. Alternately, cells within the implanted construct may be actively forming the newly regenerated enthesis
Although our tendon construct is more successful at regenerating the enthesis than current suture techniques, the excessively high strains at the site of repair may limit repair outcomes. High tensile loads, especially in chronically retracted tendons, can lead to elongation of the tendon, reducing overall muscle length and compromising shoulder function. Though the length of tendon after repair was not evaluated in this study, gross morphological changes of the supraspinatus tendon and muscle were not observed. Nonetheless, the primary benefit of our construct may be its initial compliance and the ability to remodel its structural properties over time to match the mechanical properties that are necessary to stabilize and functionalize the shoulder. In addition, initial load sharing at the repair site utilizing our construct as a biological in-lay in conjunction with suture repair may enhance repair outcomes.
There were several limitations to this study. Mechanical testing evaluated stiffness and load to failure of a single test. Cyclic loading, a more biologically representative measure, was not performed. Furthermore, material properties utilizing tissue-level strains of the repaired tissue were not evaluated due to technical difficulties and may explain the lack of significant differences in mechanics, despite histological differences in tissue composition and location of failure. Assessment of the material properties of the regenerated tissue (i.e., moduli) utilizing tissue-level strains, rather than only geometric properties (stiffness and load at failure) of the tissue, may better evaluate the quality of the regenerated tissue independent of size. Thus, the creation of a chronic supraspinatus injury in the rat may not fully represent the human condition. Healing in the rodent model is relatively robust and may not simulate the difficulties in healing and the structural failure after the repair of full-thickness tears observed in human patients. In addition, as this study focused specifically on enthesis regeneration, important components of RC injury specific to the tendon mid-substance and muscle such as muscle atrophy, fatty infiltration, quality of tendon, etc. were not evaluated.
In conclusion, the repair of acute full-thickness supraspinatus injuries in a rat model with engineered tendon constructs resulted in the regeneration of a more native-like enthesis but was not significantly different biomechanically compared with suture techniques. The utilization of our scaffold-less tendon construct for repair of chronic RC injuries was found to reduce scar formation and increase the area of fibrocartilage formation at the enthesis compared with suture repairs. Further investigation is needed to optimize the ideal tissue properties and surgical techniques for encouraging maximum enthesis regeneration
Footnotes
Acknowledgments
The authors would like to acknowledge the U of M Department of Orthopedic Surgery for funding this project as well as NIH/NIDCR Tissue Engineering and Regeneration Training Grant (DE007057).
Author Contributions
Smietana—fabrication of engineered ligament, biomechanics data collection and analysis, and article preparation; Moncada-Larrotiz—histology data collection and analysis and article editing; Arruda—biomechanics data analysis and article editing; Bedi—experimental design, data analysis, and article editing; Larkin—experimental design, data analysis, and article preparation and editing. All authors have read and approved the final submitted article.
Author Disclosure Statement
No competing financial interests exist.