
Abstract
Availability of integrase strand transfer inhibitors created interest in determining whether their use would decrease persistently infected cell numbers. This study hypothesized that adding raltegravir (RAL) to standard antiretroviral therapy (ART) would decrease human immunodeficiency virus (HIV)-infected CD4+ T cells more than standard combination ART. This was a pilot, randomized study comparing open-label standard triple ART to standard triple ART plus RAL over 96 weeks in ART-naive adults with early HIV infection. The primary objective was to compare quantity and trajectory of HIV DNA. Eighty-two persons were referred. A diverse set of reasons precluded the enrollment of all but 10. Those who enrolled and completed the study had an estimated median duration of HIV infection of 74 days at ART start. The groups had similar baseline characteristics. The RAL group had more rapid first phase plasma HIV RNA decay (0.67 log10 copies/mL/day) than with combination ART (0.34 log10copies/mL/day),
Introduction
Availability of the first integrase strand transfer inhibitor created interest in determining whether its use would decrease the number of cells persistently infected with human immunodeficiency virus (HIV) type one. Raltegravir (RAL, Isentress®) added to standard combination antiretroviral therapy (ART) in persons with chronic HIV decreased latently infected, resting CD4+ T cells and had favorable effects on ileal cell-associated unspliced HIV RNA in CD4+ T cells1,2; other studies showed no virologic impact of RAL intensification.3–6 No difference in HIV RNA or DNA was seen in randomized studies of 5-drug RAL-containing ART versus three-drug ART in recent HIV infection.7,8 Persons who start ART earlier versus later have lower HIV DNA burden.9–11 We performed a pilot study to evaluate impact of RAL in addition to standard three-drug ART in persons with early HIV infection on virologic measures and describe the challenges and lessons learned.
Materials and Methods
Study participants
Participants were ≥18 years old, ART-naïve, had HIV RNA ≥500 copies/mL within 14 days before entry and had early HIV infection defined as follows: A current positive HIV EIA and western blot with either a negative HIV EIA within the past 6 months or a negative point-of-care HIV test or a nonreactive less-sensitive (LS) HIV EIA within the past month. Exclusion criteria included pregnancy, breastfeeding, and prior HIV vaccines. Complete entry criteria are listed on ClinicalTrials.gov number NCT00781287. This study was approved by University of Washington (UW)'s Human Subjects Review Committee. Participants provided written informed consent.
Study design and procedures
This was a pilot randomized study comparing open label standard triple ART to standard triple ART plus RAL (hereafter called RAL group). We hypothesized that adding RAL to standard ART would decrease HIV-infected CD4+ T cell number more than standard ART. Standard ART, prescribed by the subject's primary care provider, was two nucleoside reverse transcriptase inhibitors (NRTIs) and a non-NRTI or a protease inhibitor. The study provided RAL 400 mg twice daily for up to 96 weeks. The study statistician performed the 1:1 randomization.
Participants underwent evaluations at entry, day 3, weekly for 4 weeks, at weeks 8, 12, 16, 24, and every 12 weeks until week 96. Consenting subjects underwent leukapheresis at entry, weeks 48 and 96 for assessment of infectious HIV in resting CD4+ T cells. Assays were performed by laboratory personnel blinded to treatment. Plasma HIV RNA levels were determined in Seattle until viral suppression using the Abbott m2000sp/rt HIV-1 RealTime assay (Abbott Molecular) and subsequently, in Bethesda using the COBAS® Ampliprep/COBAS Taqman HIV-1 Test, version 2.0 (Roche Diagnostics) done in triplicate as previously described 12 with a limit of detection of 20–48 copies/mL. Residual plasma viremia (<20 HIV RNA copies/mL) (by low copy assay) was determined by averaging Ct values obtained in triplicate from plasma specimens. Frequency of CD4+ T cells carrying HIV proviral DNA was determined by real-time polymerase chain reaction (PCR). 12 For detection of cell-associated unspliced HIV-1 RNA, 500 ng of total cellular RNA was subjected to real-time PCR using TaqMan RNA-to-CT 1-Step Kit (Applied Biosystems) and HIV-specific primers and probe. 13 Frequency of CD4+ T cells producing infectious (replication competent) HIV was measured by quantitative coculture assays. 14 Extra-chromosomal 2LTR circular DNA was assessed on stored peripheral blood mononuclear cells using a modified assay procedure.4,15 The quantity of 2LTR circles was reported as log10copies/106 CD4+ T cells. CD4+ T cells and routine toxicity assessments were performed using standard methods by UW Department of Laboratory Medicine clinical laboratories. Toxicities were graded by standard tables. 16
Statistical considerations
The primary objective was to compare quantity and trajectory of HIV-infected CD4+ T cells, assessed by HIV DNA. Secondary endpoints included levels and trajectory of plasma HIV RNA, cell-associated RNA, quantity and half-lives of CD4+ T-cells with infectious virus, and clinical and laboratory toxicities. Residual plasma HIV viremia and 2LTR circles were added as secondary endpoints when these assays became available.
The study originally had a sample size of 10 per arm and 88% power to detect a 0.7 log10 difference in HIV DNA at 96 weeks, assuming a standard deviation (SD) of 0.5 log10 and using a two-sided
Results
Enrollment, participant characteristics, and follow-up
Subjects enrolled from March 2009 to 2011. Follow-up ended in February 2012. Figure 1 describes the disposition of individuals referred for participation and enrollees.

Disposition of individuals who screened for and participated in the study. ART, antiretroviral therapy; HIV, human immunodeficiency type 1; LS-EIA, low-sensitivity enzyme immunoassay.
Table 1 describes baseline characteristics of enrollees. Participants had symptoms consistent with primary HIV infection; nine sought medical attention. Each had early HIV infection with an estimated median HIV infection duration of 74 days at ART start. Each group's characteristics were similar except for a trend toward higher HIV RNA values at screening in the RAL group (
Two subjects had Fiebig I/II at diagnosis.
One subject is missing in the raltegravir-containing group.
One subject is missing data in each group.
ART, antiretroviral therapy; CCR5, C-C chemokine receptor 5; HIV, human immunodeficiency virus; LTR, long terminal repeat; mL, milliliter; mm, millimeter; NNRTI, non-nucleoside reverse transcriptase inhibitor; No., number; PBMCs, peripheral blood mononuclear cells; 1°, primary HIV; PI, protease inhibitor; RNA, ribonucleic acid.
Virologic, immunologic, and clinical outcomes
The RAL group had more rapid first phase plasma HIV RNA decay (0.67 log10copies/mL/day) than the other group (0.34 log10copies/mL/day),
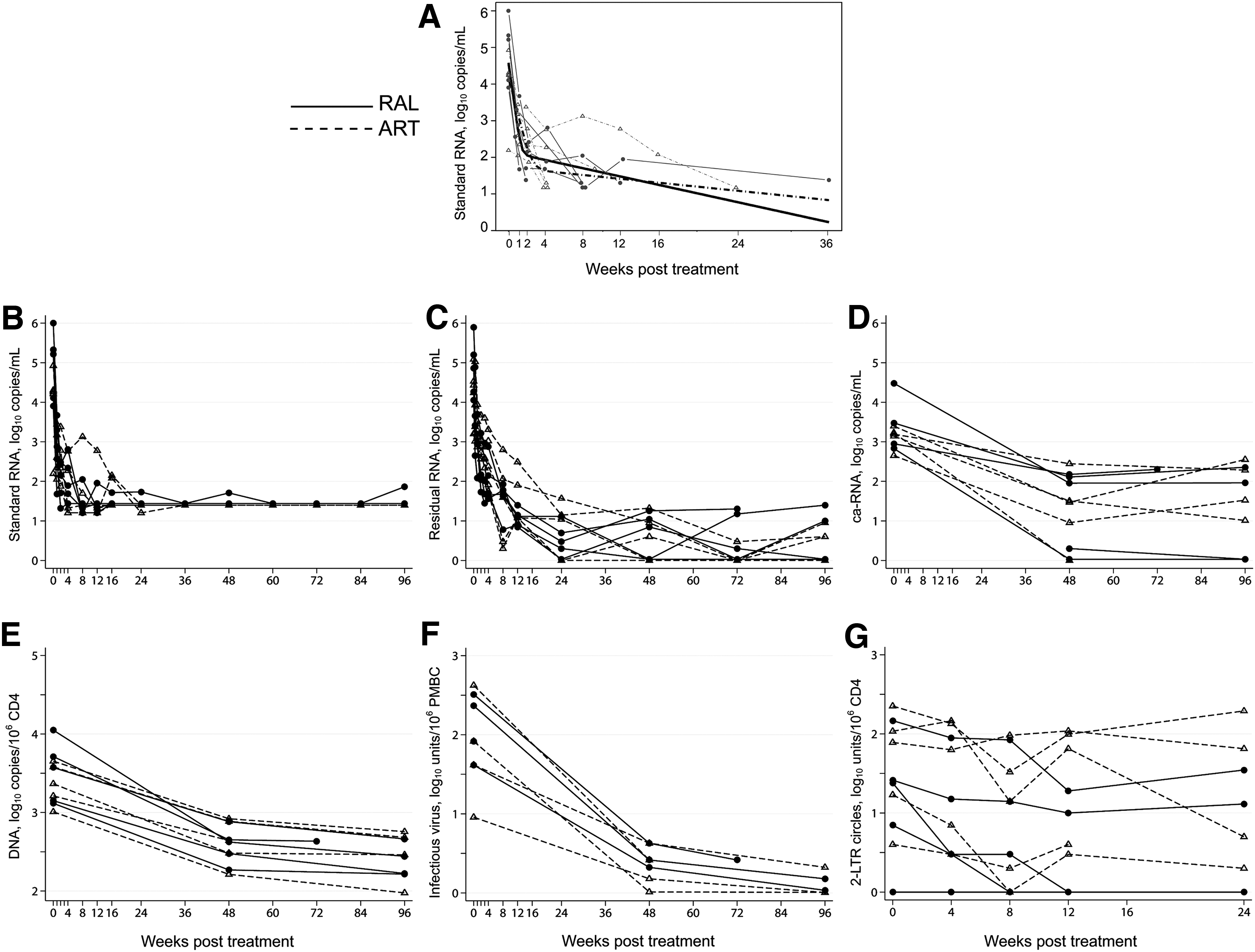
Virologic parameters by treatment group over time.
Given a trend toward differences between groups in screening plasma HIV RNA levels, we reanalyzed virological parameters by dividing subjects by median entry plasma HIV RNA level of 4.48 log10copies/mL. Among those with higher entry plasma RNA, 2LTR circle levels were significantly lower over time than in those with lower entry RNA (
DNA, deoxyribonucleic acid; HIV, human immunodeficiency virus; PBMCs, peripheral blood mononuclear cells; RNA, ribonucleic acid.
There were no differences between randomized groups in CD4+ or CD8+ T cell counts or CD4:CD8 ratios. No subjects developed AIDS-defining or HIV-associated illnesses. One subject had transient, self-limited grade 3 neutropenia unrelated to ART. All other signs, symptoms, and laboratory values were grade 2 or less and typical of the ART used.
Discussion
When ART was started during early HIV, our results suggest homogeneity of responses in residual viremia, cell-associated RNA, HIV DNA, and CD4+ T cells with infectious virus. First phase decay of HIV RNA was faster in subjects receiving RAL in addition to standard triple ART.
It was of interest that levels of 2LTR circles were lower over time among subjects with higher compared with lower pre-ART HIV RNA levels. We hypothesize that the difference in 2LTR kinetics represents differences in infected CD4+ cell clearance and different rates of replenishment between these two groups of initially viremic subjects. Some studies have suggested that 2LTR circles may increase in persons with chronic HIV when they are treated with RAL-containing regimens but others, including the present study in persons with early HIV, have not seen such changes.11,18,19 Following ART initiation, kinetics of 2LTR DNA did not reflect the kinetics of plasma HIV RNA decline.
Enrolling our study was unexpectedly challenging. Our group has enrolled 394 subjects with acute or early HIV since 2002 in an observational study that does not require or exclude ART; the proportion of immediate ART start has varied over time, likely reflecting evolving views of ART's potential benefits and risks. When the current study was conducted, U.S. treatment guidelines were not supportive of early ART. 20 Other issues included the lack of sensitive, readily available assays during the study to detect early HIV; eight potential participants with recent sexual HIV exposure and documented past negative HIV tests (as recently as 7 months previously), suggesting recent HIV infection, had positive LS-EIA assays so were excluded from participation. A wide variety of other reasons prevented potentially eligible persons from enrolling.
Limitations of this pilot study include being underpowered for treatment comparisons, selection bias toward participants with symptomatic primary infection, and lack of subject diversity (although reflective of the epidemic in the Pacific Northwest). Nonetheless, with increased interest in early ART and understanding relationships among different virologic parameters, the lessons learned from this study may increase knowledge about effects of ART in early HIV and help the design and implementation of future studies.
Conclusions
A diverse set of reasons adversely impacted enrollment in this pilot study. The RAL group had more rapid first phase decay than combination ART without RAL. Our results suggest homogeneity of responses in cell-associated RNA, HIV DNA, CD4+ T-cells with replication competent virus, and 2LTR circles to early ART in both treatment groups. Following ART initiation, the kinetics of 2LTR DNA did not reflect the kinetics of plasma HIV RNA decline.
Footnotes
Acknowledgments
This study was supported in part by a research grant from the Investigator-initiated Studies Program of Merck & Co., Inc., by a grant for supplies from Roche Molecular Systems, the University of Washington/Fred Hutch Center for AIDS Research (P30 AI027757), and NIH grant AI57005. We wish to thank the study participants, Helen Horton and her laboratory for separation and shipment of peripheral blood mononuclear cells, Audrey Wong and the UW Clinical Retrovirology Laboratory for performing the 2LTR assays, and the Puget Sound Blood Center for performing leukaphereses. We also acknowledge Terri Smith and Bess Sorensen for their assistance with data management.
The opinions expressed in this article are those of the authors and do not necessarily represent those of Merck & Co., Inc.
Author Disclosure Statement
A.C.C.: Membership on a Data and Safety Monitoring Board for Merck-sponsored studies and previous stock ownership in Abbott Laboratories, Bristol-Myers-Squibb, Johnson & Johnson, and Pfizer.
M.C., T.-W.C., R.W.C., D.M., S.E.H., J.S.J., J.M., J.I.M., K.T., J.D.S., and C.E.S.: No competing financial interests exist.