
Abstract
The traumatic rupture of tendons is a common clinical problem. Tendon repair is surgically challenging because the tendon often retracts, resulting in a gap between the torn end and its bony insertion. Tendon grafts are currently used to fill this deficit but are associated with potential complications relating to donor site morbidity and graft necrosis. We have developed a highly reproducible, rapid process technique to manufacture compressed cell-seeded type I collagen constructs to replace tendon grafts. However, the material properties of the engineered constructs are currently unsuitable to withstand complete load bearing in vivo. A modified suture technique has been developed to withstand physiological loading and off load the artificial construct while integration occurs. Lapine tendons were used ex vivo to test the strength of different suture techniques with different sizes of Prolene sutures and tissue-engineered collagen constructs in situ. The data were compared to standard modified Kessler suture using a standard tendon graft. Mechanical testing was carried out and a finite element analysis stress distribution model constructed using COMSOL 3.5 software. The break point for modified suture technique with a tissue-engineered scaffold was significantly higher (50.62 N) compared to a standard modified Kessler suture (12.49 N, p<0.05). Distributing suture tension further proximally and distally from the tendon ends increased the mechanical strength of the repairs. We now have ex vivo proof of concept that this suture technique is suitable for testing in vivo, and this will be the next stage of our research.
Introduction
Tendon ruptures may occur either due to traumatic lacerations or excessive loading of the tendon. 1 Worldwide 3–5 million people experience tendon-related injuries every year. 2 In the United Kingdom every year half a million people experience work-related tendon and joint disorders. 3 Surgical reconstruction of a ruptured tendon is challenging because tissue fragmentation into individual fibers and fascicles hence sutures are unable to hold a tension. 4 Additionally, tendons are usually under physiological tension, and following rupture the ends of the tendon retract, leaving a gap either between the torn tendon ends or its bony insertion. Various graft materials have been used to fill this deficit including allografts,5–7 autografts,8–10 xenografts,11,12 and synthetic grafts.13–16 These strategies have inherent weaknesses such as autografts leading to donor site morbidity and having limited availability,17–19 while allografts are expensive, require storage, and may elicit an immune response leading to rejection.20,21 Xenografts and synthetic polymer grafts are less immunocompatible, and graft rejection foreign body reaction often occurs.22,23
Collagen is an important protein component in the mammalian connective tissue. The tendon matrix is predominantly type 1 collagen, and we have used collagen as a naturally occurring polymer. It has certain inherent advantages because collagen is a structural protein, and ∼85% dry weight of tendon consists of collagen type 1.24–27 Our center has developed an ultrarapid engineering method using plastic compression of collagen hydrogels to form biocompatible scaffolds for various tissue engineering applications such as skin, blood vessels, bladder, nerve, and cornea.24,28–30 This type I collagen tissue-engineered (TE) graft is “off the shelf,” easily reproducible, and nonallogenic.31–33 These TE grafts have previously been seeded with different cell types and implanted in vivo into the nursery site in a lapine model with successful graft integration. 34 But the TE tendon material properties were not suitable for holding the sutures and taking the load of a tendon like a normal tendon graft. We have now devised a strategy to modify the suture technique so that the suture loads are held proximal and distal to the inserted graft. We have tested this modification in an ex vivo model and compared it to the traditional modified Kessler's technique and tendon graft.
The purpose of study was to surgically optimize this graft insertion technique as a proof of concept ex vivo study, which will allow the next stage of testing in vivo.
Materials and Methods
Animal surgical procedure and tissue collection
New Zealand white rabbits aged between 16 and 25 weeks, weighing between 3.0 and 4.5 kg were sacrificed following ethical approval and under regulation of University College London, under Schedule 1 of Animal Procedure Act 1986. Surgical tenotomy was performed on the hind legs to extract the posterior tibial tendon (PT tendon). Harvested tendons (n=56) were snap frozen in liquid nitrogen immediately after extraction and stored at −20°C until further use. Prior to mechanical testing, the tendons were thawed for 2 h and brought to room temperature. All mechanical testing and ex vivo surgical procedures were carried out at room temperature.
Atomic force microscopy for analysis of intact tendon and TE collagen construct
Type 1 collagen fibrils were dissected from rat tail tendons and stored in phosphate-buffered saline azide at 4°C. An extract of the collagen tendon was sectioned with a scalpel and washed for 5 min in deionized water. A microscope glass slide (Agar Scientific, Essex, United Kingdom) was used as sample substrate. It was cleaned with deionized water in an ultrasonic bath for 5 min and subsequently rinsed with 100% ethanol and dried in a stream of nitrogen. A few bundles of collagen fibers were deposited on the glass slide without smearing, using tweezers. The sample was then dried in a gentle stream of nitrogen. Collagen constructs were cast using the methods previously described by Levis et al. 28 Once prepared, the collagen constructs were rinsed in ultrahigh quality water before being cut into sections of approximately 5 mm2 with a scalpel. The samples were then deposited on a glass slide before being dried using a gentle nitrogen flow. Dimension 3100 (Bruker, Santa Barbara, CA) Atomic Force Microscope was used for imaging the samples in contact mode using CSC probes (MikroMasch, Tallinn, Estonia). Typical scan rate of 2 Hz was used for contact mode imaging, and the deflection set point was reduced to minimize the force applied onto the sample. Both deflection/amplitude and topography images were recorded using Multimode Nanoscope IV (Veeco, Santa Barbara, CA), fitted with an E scanner and NSC tips-D lever (MikroMasch).
Fabrication of collagen constructs
Collagen constructs were made using 4 mL of rat tail collagen type I (First Link, Birmingham, United Kingdom) and 1 mL of 10× minimal essential medium (Invitrogen, Paisley, United Kingdom), neutralized using 5 M and 1 M sodium hydroxide (Sigma-Aldrich, Dorset, United Kingdom). Five milliliters of this solution was poured into rectangular metal molds of 33 mm×22 mm×10 mm dimensions. Molds were kept in an incubator at 37°C and 5% CO2 for 15 min to allow fibrillogenesis. To mimic tendon shape and size four layers of collagen gels were compressed one on each other (Fig. 1). Discharged water from hydrogels was absorbed by four Whatman filter papers (Fisher Scientific, Loughborough, UK). Compressed gels were rolled and construct was cut into segment of 15 mm.
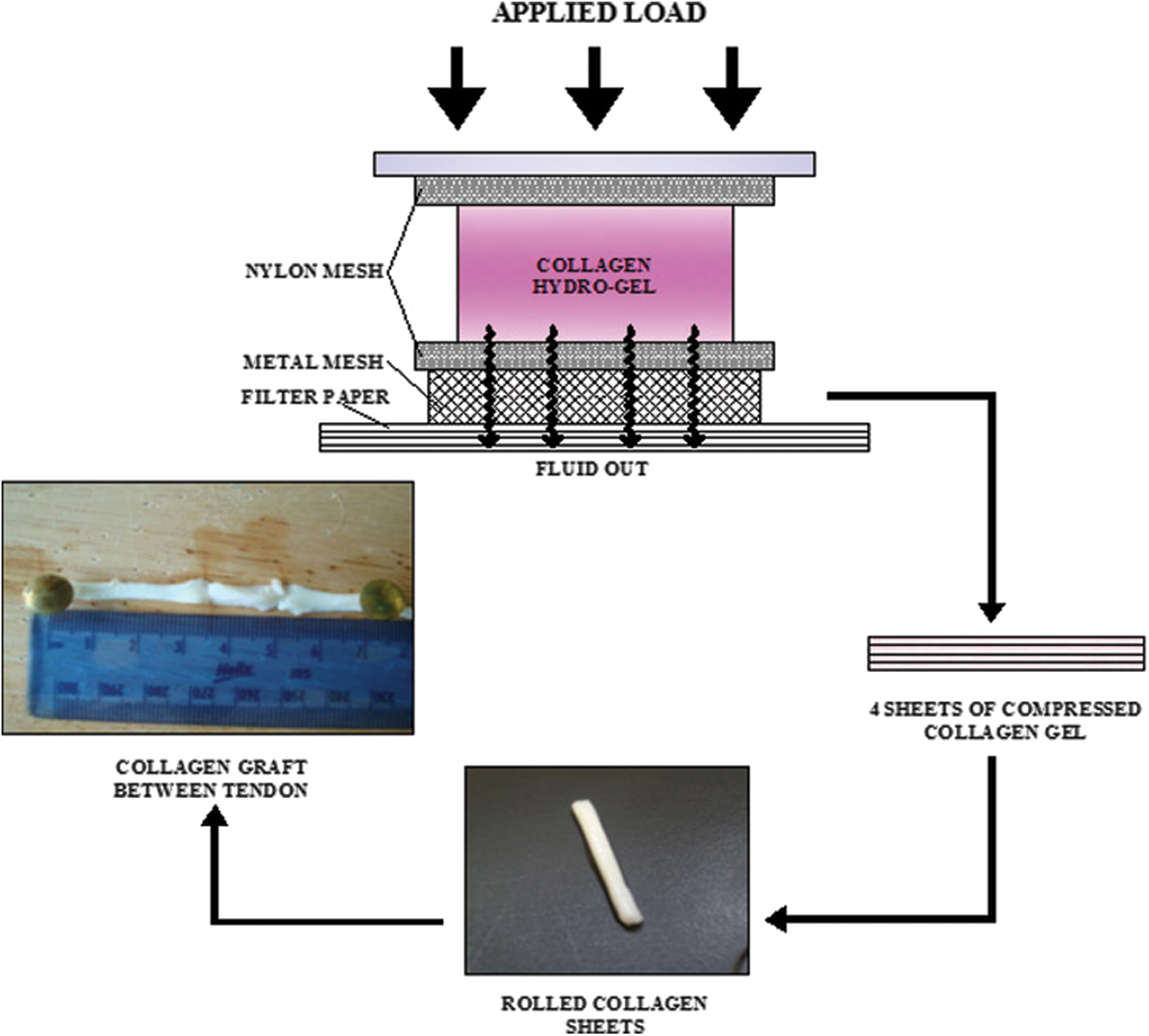
Mechanism of plastic compression method for the fabrication of tissue-engineered collagen construct inside tendon.
Suture technique
Three different repairs were performed: (1) standard repairs with modified Kessler (MK); (2) modified repairs of divided tendons with autograft repair (TAG); and (3) modified repairs of divided tendons with tissue-engineered graft repair (TEG). Prolene (Ethicon Ltd, Edinburgh, United Kingdom) monofilament and nonabsorbable sutures were used for all ex vivo experiments. Rabbit tendons were defrosted to room temperature and kept moist throughout the experiment. The average length of the rabbit PT tendon was 70 mm. Tendons were surgically divided at the midpoint with a sharp blade. A standard repair was performed using a MK technique (n=7). Four 6-0 Prolene core sutures were passed 15 mm from the tendon ends and through tendon graft (Fig. 2A) where tendon graft was then held together with a further 6-0 Prolene running suture around the whole periphery of the tendon.

In the TAG group, 15 mm of tendon was excised from the middle of the tendon, turned through 180°, and then repaired using the modified suture technique. In the TEG group, 15 mm of tendon was excised from the middle of the tendon and replaced with the TE collagen graft. Instead of two Kessler sutures being performed at each end of the graft, the 3-0 Prolene core sutures were passed through the middle of the entire length of the graft so that the graft could be moved easily on the suture and the tension was placed on the native tendon. Both ends of the graft were then secured to the native tendon with 6-0 Prolene running sutures around the periphery (Fig. 2B). This minimized the tension on the graft.
Mechanical testing of the repairs
Mechanical testing was performed on Prolene sutures of differing diameters (2-0, 3-0, 4-0, 5-0, 6-0, and 7-0) and on four different groups of tendons: (1) intact rabbit tendons (n=7), (2) divided tendons with MK (n=7), (3) divided tendons with TAG (n=7), 4) divided tendons with TEG (n=7). All specimens were tested under tension to failure using a Zwick/Roell (Z005 model, Ulm, Germany; Fig. 4A) loading machine with a test speed of 100 mm/min for intact PT tendons and 50 mm/min for repaired tendons. All tendons were brought to room temperature in phosphate-buffered saline prior to testing. Securing the tendon ends to the machine was challenging due to slippage of the tendon, and after different methods of clamping were tested, sand paper was finally used because tendons remained in the clamps and failed midsubstance. The area of tendon input was calculated, and force was applied until failure. Break strength output was generated by testXpert V10.0 software (Zwick, GmbH & Co, Ulm Germany).
In situ mechanical testing
The amputated hind legs of each rabbit and its average weight was 124 g. Each leg was shaved in the work region and a 4-cm incision was made with a number 20 surgical blade in the posterior aspect of the inferior tibiofibular region to expose the PT tendon. A midsection of the tendon was divided, and MK repair was performed or a 15-mm section of the tendon was excised and a TEG was placed in situ and secured using the same suture technique as previously described. In situ mechanical testing was then conducted by applying force to flexor tendons of the cadaver rabbit's hind leg to exhibit maximum tension on the PT tendon, where the collagen construct or graft was placed. The leg was mounted on the Zwick test machine, and force was applied with speed of 50 mm/min (Fig. 4B).

Scanning electron microscopy sample preparation
Tendons after pull-out tests were fixed with 2.5% glutaraldehyde in 0.1 M sodium cacodylate buffer (Agar Scientific) pH 7.4 for 30 h. Samples were washed with 0.1 M cacodylate buffer and subsequently washed with 20%, 30%, 40%, 60%, and 90% ethanol twice with intervals of 5 min and with 96% and 100% ethanol washed for 15 min. These samples were rinsed with transition solvent hexamethyldisalazene (Sigma-Aldrich Inc., St. Louis, MO) for 3 min in the fumehood and air dried for 20 h. Samples were mounted on stubs and gold sputtered for analysis under scanning electron microscope (JSM500, JEOL, Hertfordshire, United Kingdom). Imaging was done at secondary electron beam.
Finite element analysis
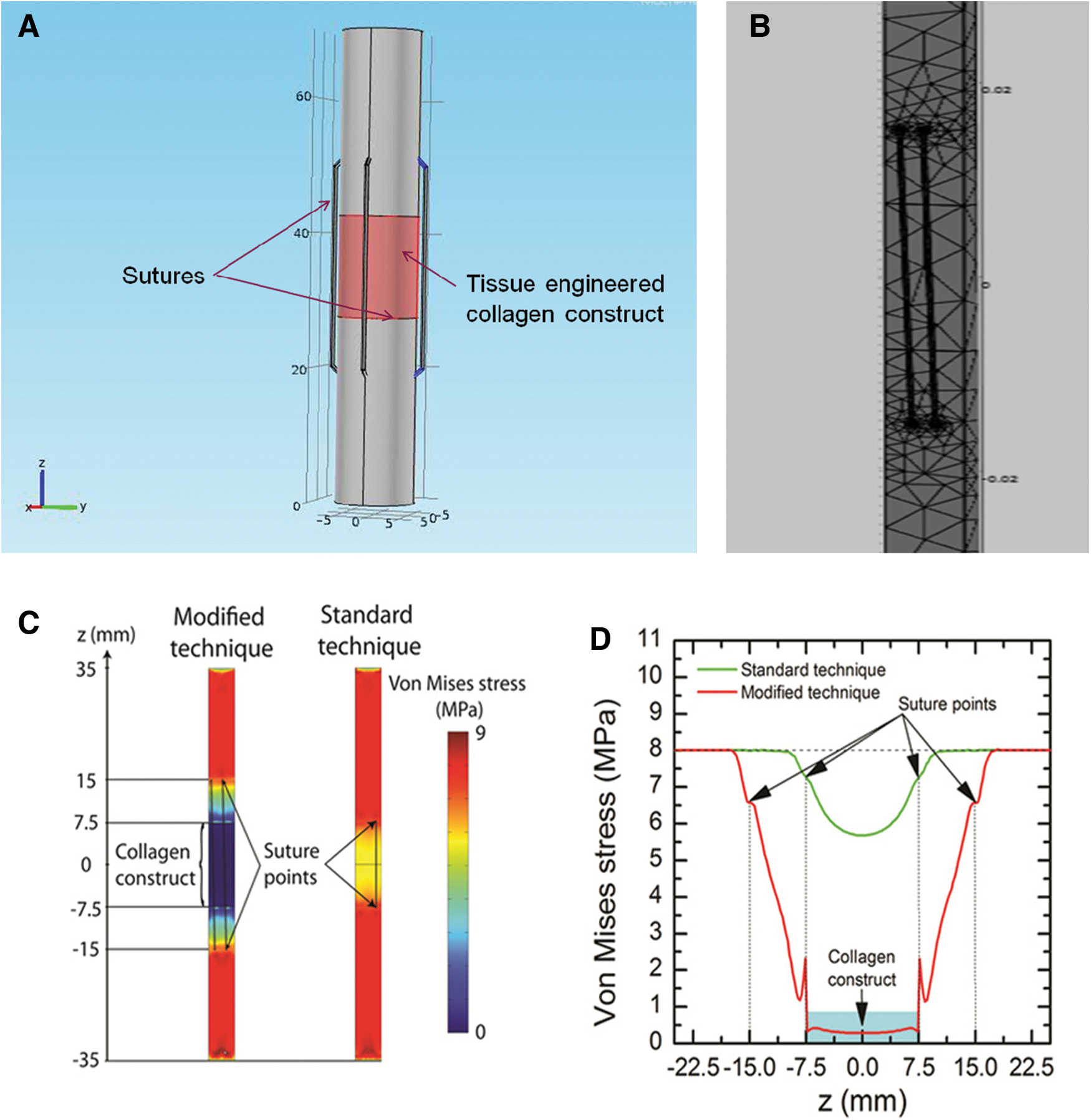
Finite element analysis was carried out to correlate experimental results and develop a computational profile of the force distribution across the tendon and engineered construct in a load-bearing model using dimensions of natural tendon as already described. We found experimentally that when the modified suture technique was carried out, the repaired tendon broke at a load of ∼7.6×106 Pa. This break load value was used in the simulations, which were carried out using COMSOL Multiphysics V3.5. (COMSOL Ltd., Cambridge, United Kingdom) software. Stress distribution was compared between the modified and standard suturing technique.
Statistical analysis
One way ANOVA was performed by using SPSS 20.0 (SPSS IBM cooperation, Chicago, IL) and post hoc analysis was done using Bonferroni correction. In all cases the p value was considered significant at p<0.05. Results are shown as mean±SD.
Results
Atomic force microscopy analysis of rat tail tendon in tail and TE collagen construct
Atomic force microscopy (AFM) imaging was carried out on the both the rat tail tendon and TE collagen construct as described. In both samples, collagen fibrils could be clearly observed. In the TE collagen construct the orientations of the fibrils were random (Fig. 3A), whereas in the natural tendon (Fig. 3B) the architectural alignment of collagen fibrils was exclusively unidirectional.
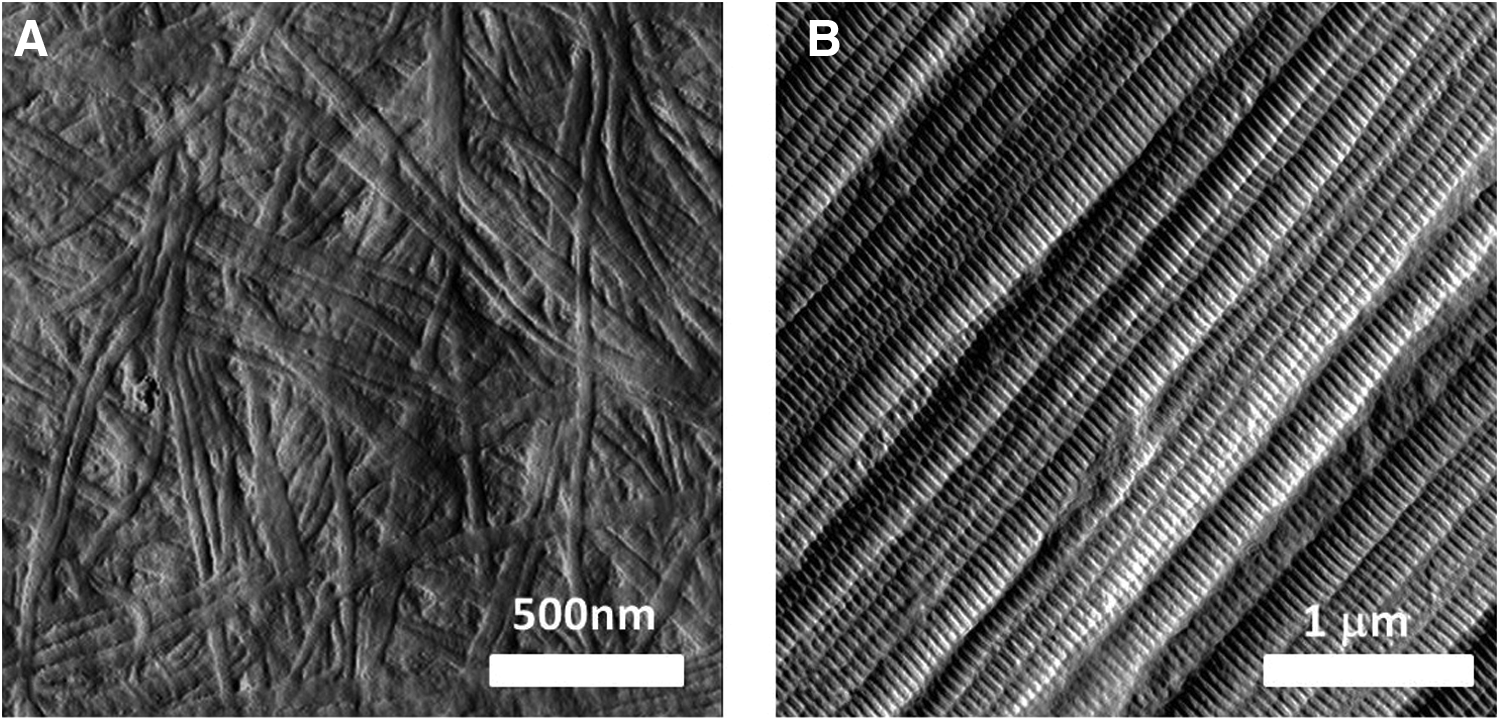
Atomic force microscopy image of collagen fibril alignment
Break strength of Prolene sutures
The suture break strength was calculated for different diameters of Prolene suture and was found to be directly proportional. Break strengths for Prolene 7-0, 6-0, 5-0, 4-0, 3-0, and 2-0 were 2.56±0.18 N (n=4), 4.46±0.11 N (n=4), 8.20±0.27 N (n=4), 14.16±0.12 N (n=4), 20.81±0.25 N (n=4), and 34.81±1.86 N (n=4), respectively. Given that the rabbit PT tendon has an average length of 70±2.5 mm (n=15), width of 5±1.3 mm (n=15), and thickness of 1.5±0.85 mm (n=15), Prolene 3-0 sutures were used for outer interlocked sutures, while Prolene 6-0 sutures were used to hold the TE collagen construct in place with running sutures.
Breaking strength of rabbit PT tendon and tendon repairs
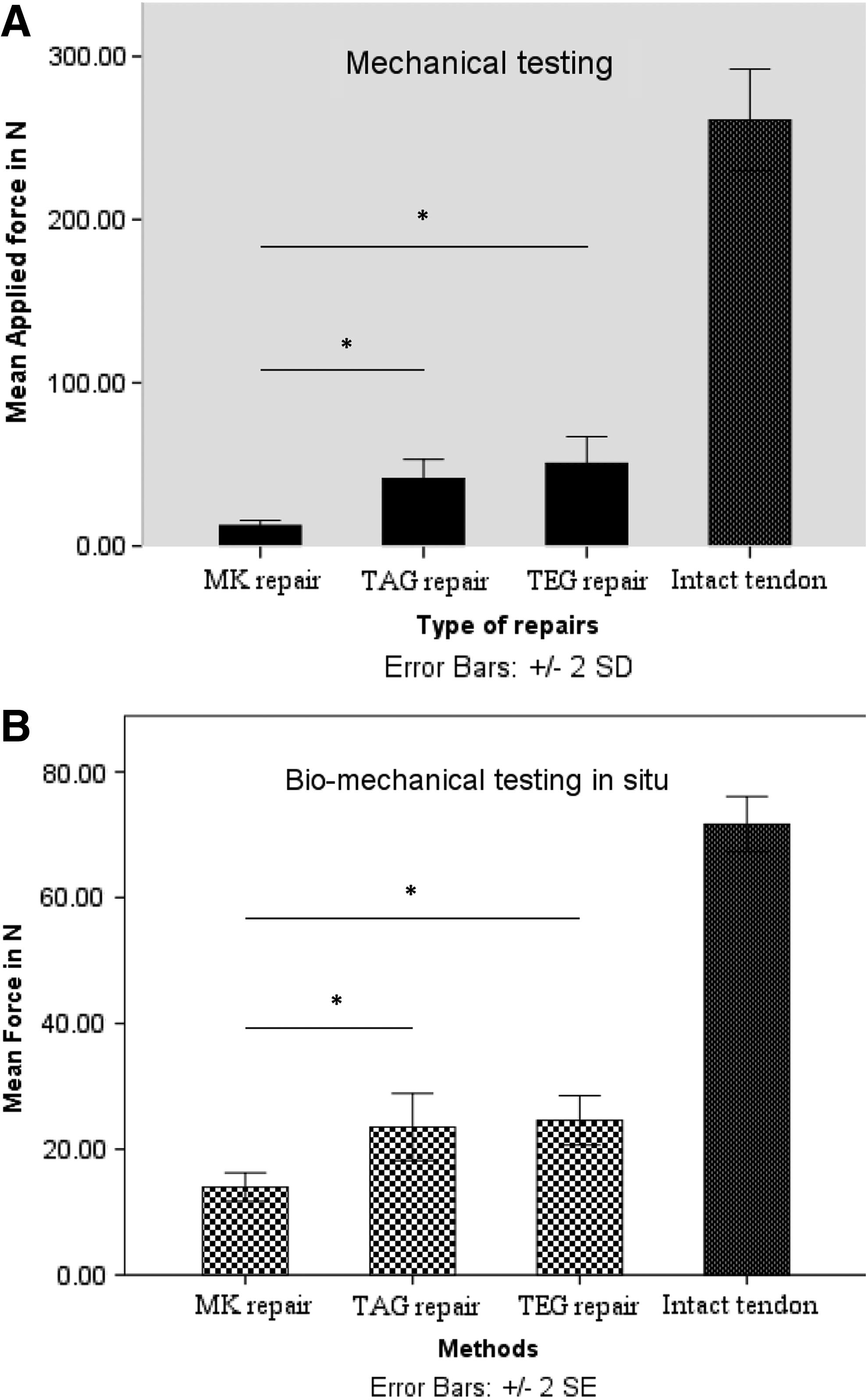
The breaking strength of rabbit PT tendon was measured on the Zwick/Roell loading machine with test speed of 100 mm/min. The breaking strength of intact PT tendon of rabbits was 261.08±15.57 N (n=7). The average break strength of a standard MK tendon repair using a MK suture was 12.49±1.62 N (n=7). The average break strength of the TAG using our modified suture technique was 41.4±5.87 N (n=7; p<0.05), and the average break strength of the TEG was 50.62±8.17 N (n=6; p<0.05; Fig. 5A). On the stress–strain curve, when tendons were stressed more than 15%–20% of their original size they failed.
Biomechanical in situ analysis
Testing of the tendons within the hind leg revealed that intact tendons failed at 71.69±4.39 N (n=7). Tendons repaired in situ within the hind leg had a break strength of 13.98±2.26 N (n=7) for MK repairs; 23.52±5.35 N (n=7; p<0.05) for TAG and 24.60±3.92 N (n=7; p<0.05) with TEG (Fig. 5B). All graft repairs failed at the sutures site. In the pull-out test it was observed that, for MK all repairs broke at suture point, but in some experiments for the modified suture technique, the tendon avulsed from muscle end. On the stress–strain curve, the maximum strain on the tendon was up to 8%–10%.
Scanning electron microscopy analysis of repairs
Surface topology for the intact tendon was used as a standard control (Fig. 6A). Tendons subjected to a pull-out test gradually lost their crimp pattern with evidence of microscopic failure at 8% strain (Fig. 6B). In MK repaired tendon (Fig. 6C) after performing a pull-out test, evidence of rupture at the edge at suture points and the surrounding tendon was seen. At <4% strain the tendons lost their crimp pattern at the suture points. In the modified TEG tendon (Fig. 6D), stress was seen only around suture points, and the surface topology of the tendon was unchanged until 10% strain was exceeded. At this point, loss of the crimp pattern was observed.

Scanning electron microscopy image of tendon (×35).
Finite element analysis
Experimentally, we found that at a load of 8×106 Pa the Von Mises stress in the middle of the geometry, that is, in the middle of the collagen construct (for the modified technique TAG or TEG) or at the point of the running sutures (for the standard MK technique), was 5.6×106 Pa for the standard technique and 2.8×105 Pa for the modified technique (Fig. 7C) hence it was evident that the stress was only 1/20 of the standard technique if the TEG suture technique was used. The stress was independent (differences are smaller than 5%) of the “bite depth,” that is, how far the suture goes into the material. These values were also independent of whether “contact pairs” between the sutures and the collagen construct were implemented into the model or not, demonstrating that the simulations are fairly robust. At a load of 8×106 Pa, the Von Mises stress on the sutures in the vertical center of the geometry was 1.6×108 Pa for the standard technique and 2.6×108 Pa for the modified technique. Stress was actually higher for the modified technique (Fig. 7D). These results were surprising at first, but one has to keep in mind that although the force was distributed onto four sutures in the case of the modified technique (compared with two sutures for the standard MK technique), the collagen construct basically takes no load off the sutures.
Experimentally, it was found that it is not always the same component that breaks first. The break point of the collagen construct by itself was measured as 3.8×105 Pa. This was ∼36% greater than the calculated stress (at an overall load of 8×106 Pa), in agreement with the experimental data generated, which showed that the collagen construct did not break.
The calculated stress on the sutures needs to be compared with their break stress, which was measured to be 3.7×108 Pa (for the 0.27-mm-diameter polypropylene sutures). The break stress was indeed close to the calculated stress of about 2.6×108 Pa. It was actually expected that the calculated stress was underestimated to some degree because the model assumes a “perfect suturing”; that is, each of the four suture points are at the same vertical positions and of the exact same length. In reality, one of the suture connections may be slightly longer than the others and hence experience a larger stress. Such a connection would then break first. This model was in good agreement with the experiment.
Discussion
Tendon rupture is a common phenomenon worldwide. Surgeons have been using tendon grafts since the 17th century. 35 Many methods and strategies have been developed for tendon repair, but still it remains a challenge.
Collagen as a polymer has been fabricated and used as a biomaterial for various tissue-engineering applications36,37 and also for tendon tissue engineering.31,38–40 Collagen exhibits all characteristics of an ideal biomaterial for tendon TE described by Liu et al. 41 and by Henson and Getgood, 42 but the mechanical properties of TE collagen construct are currently inferior to the intact tendon. Therefore, we visualized alignment of collagen fibrils by AFM, which showed that when force was applied to the natural tendon (break strength, 261.08 N; Fig. 3B), almost all collagen fibrils contributed to the force transmission and the linear alignment of fibrils made them a stronger network. In the TE construct (break strength, 2.82 N; Fig. 3A) only a few fibrils that were aligned linearly in the direction of applied force contributed to the force transmission. The rest of the fibrils distributed force randomly, hence the TE construct was weak. In view of our collagen constructs being mechanically weak post tendon repair, the mechanical strength of the repaired tendon graft was entirely dependent on the suture technique and material, but not on the tendon/tendon graft.43,44 We have developed and described a four-strand grasp modified interlocking suture technique by inserting the suture point distally and proximally away from the tendon cut end, which distributes suture tension further proximally and distally away from the tendon cut end. Results were compared with the standard MK repair technique, which is considered one of the gold standards for a tendon repair because it is less obstructive and damaging to the tendon.45,46
Break strength of intact tendon was measured (261.08±15.57 N) to provide evidence that our repairs were stronger than the conventional method and close to the break strength of natural tendon. The break strength of tendon with the MK repair (12.49±1.62 N) was less because when two ends of tendon were pulled together and sutured, it led to tension in the sutured region and repair failed at low force. Interestingly, we found that the modified suture technique for TAG (41.4±5.87N) and TEG (50.62±8.17N) differed, although the method and operating person was the same. This might be due to suture bite depth or individual variation in the suture techniques.
Earlier testing was performed ex vivo, and for the suturing technique to be applicable for in vivo testing we had to test in situ whether it was feasible within the anatomic space available. Also, the ex vivo strain on tendon was more than 20%, but in vivo the tendon can take strain up to 8%–10%. In situ break strength for modified repair was stronger to MK repairs (13.98±2.26 N) and break strength for modified repair with TAG (23.52±5.35 N) and TEG (24.60±3.92 N) grafts were approximately equal, which signifies that it does not matter whether the tendon graft or the collagen construct suture takes the load.
Sharing suture tension further away from the tendon ends increased the mechanical strength of the repairs, and the repairs were able to withstand higher magnitudes of force compared to MK repair. With modeling, we demonstrated that after applying force to the tendon, load was shared on sutures and not by the construct. Using this proof of concept data, we will now apply this modified suture technique in vivo to test integration and function in a lapine model by seeding a collagen construct with bone marrow stem cells and tendon fibroblasts. We hypothesize that over time the construct will mature into a fully formed tendon. If successful, this modified suture technique can be used across all tendon repairs to accommodate TE tendon constructs and reduce the use of tendon allografts and autografts.
Footnotes
Acknowledgments
We would like to thank the government of India for funding this project, Rebecca Porter (Institute of Orthopaedics, UCL) for helping us in the lab, and Cathy Gray (Northwick Park Institute of Medical Research [NPIMR]) for her surgical assistance.
Disclosure Statement
No competing financial interests exist.