
Abstract
A highly osteogenic hybrid bioabsorbable scaffold was developed for bone reconstruction/augmentation. Through the use of a solid free-form fabrication technology, a bioabsorbable polycaprolactone (PCL) cage scaffold with a desired size and shape was produced and then filled with osteogenic bone graft particles, that is, morselized autologous bone chips. A rabbit total lamina defect model was chosen to demonstrate its efficacy in regenerating bone with a complicated anatomic shape. Both iliac bone and morselized iliac bone grafts were used in this study for comparison purposes. Serum osteocalcin and collagen type I cross-linked C-terminal telopeptide (CTx) determination showed that active bone remodeling occurred after bone grafts were implanted. X-ray images showed that the bony defects were completely filled with bone mass in all the groups with bone grafts. However, biomechanical tests showed that only the iliac bone and hybrid scaffold groups could restore the mechanical properties to the normal level after 10 weeks of implantation. A histology study showed that both iliac and hybrid scaffold groups had extensive new bone formation, and no adhesion and fibrosis were found. These results indicated that this osteogenic hybrid scaffold can be a good alternative to autologous iliac bone, because it does not need a second iliac bone-harvesting surgery, and thus the morbidity and the possible infections that are often associated with the bone harvesting surgery can be avoided.
Introduction
Bone defects can be caused by trauma, surgical procedures, cancer removal, etc., and they come in various sizes and shapes. Severe bone loss can be difficult to treat because of the complicated anatomy and physiology of bone tissue. Bone tissue engineering offers a promising alternative treatment for these types of severe bone losses. 1 Implants that are used to repair these defects need to have the right size and anatomy shape to fit into the defects to repair. Using the patient's computed tomography (CT) or magnetic resonance imaging data, solid free-form fabrication can be a very powerful tool to produce defect specific scaffolds for bone repair.2–4 However, these scaffolds, fabricated either from ceramics or from polymers, lack the osteogenic capability. So, for large or difficult to repair defects, a highly osteogenic scaffold is needed to facilitate or promote the bone tissue regeneration.
Osteogenic bone grafts are available in a particulate form, such as allogeneic demineralized bone matrix (DBM) particles and growth factor-loaded microbeads and particles.5–10 Even fragments of autologous bone, the gold standard of bone graft, are frequently available from surgical procedures. For example, autologous bone fragments are often available from various types of surgical procedures, such as bone discs from skull trephine procedures and bone fragments from total laminectomy. These autologous bone pieces are often discarded as medical waste, because once they are broken into small pieces, they are difficult to put back into the defect and keep in the defect without migration.
On the other hand, the advantage of using particulate implant materials is that the particulates can be packed into a bony defect of any size and shape. To take the advantage of these particulate bone grafts, we have developed a totally bioabsorbable porous polycaprolactone (PCL) cage for packing osteogenic bone graft particulates and use for bone reconstruction/regeneration. After packing the particulates into the cage device with a porous wall, the packed implant can be fitted into the defect that needs to be repaired and/or restored both structurally and anatomically. To demonstrate the feasibility of this technology, we have chosen to conduct a rabbit animal study to rebuild the lamina after total laminectomy.
A laminectomy is a surgical procedure in which a surgeon removes a portion of the lamina to treat various clinical conditions such as spondylolisthesis, spinal stenosis, and discogenic back pain.11–14 In most cases, a laminectomy is an elective procedure rather than an emergency surgery.
Scar tissue formation and mechanical instability at the surgical site are the two common problems associated with the laminectomy and may lead to failed back surgery syndrome (FBSS) after laminectomy. 15 Postoperative epidural scar formation can cause extradural compression or dural tethering, which results in recurrent radicular pain and physical impairment. 16 In addition, the removal of lamina will cause lumbar instability from a biomechanical point of view.
Therefore, an ideal implant for reconstruction of a lamina should have two important roles. First, it should be able to prevent epidural scar tissue formation to prevent FBSS from happening. Second, the implant should be able to provide mechanical support eventually, if not immediately postlaminectomy. Reconstruction of spinal defects is critical for stabilization of the spine. Although the metallic hardware bears the majority of the stress during the first few months after reconstruction, as the bone graft incorporates or the implant is gradually being replaced by the new bone, the newly formed bone should bear the majority of the stress. If the hardware ever needs to be removed at any point after this, the patient's spine will still remain stabilized.
There also have been some attempts to develop an artificial lamina that can both effectively prevent the scar tissue formation and restore the mechanical stability of the spine. A biodegradable copolymer alpha–tricalcium phospate (TCP)/poly(amino acid) composite artificial lamina was prepared and used in goat cervical vertebra resection repair. 17 It was found that 24 weeks after the operation, the artificial lamina refrained from shifting, and no dural adhesion pressure was observed.
Bone autografts are the gold standard. Morselized autologous bone has been shown to have high osteoinductive potential. 18 Impacted morselized bone grafts were used successfully to restore bony defects in revision surgery in the acetabulum and the proximal femur.19–21 Morselized autologous bone has been used in vertebral augmentation and reconstruction. 22 It is of particular interest to use morselized autologous bone in this case, because some of the lamina bone will be removed and discarded during a laminectomy. Therefore, it would put the best use of this removed broken lamina bone as morselized autologous bone graft for lamina reconstruction.
To reconstruct lamina, these morselized bone grafts cannot be used directly, because they will not easily form the shape of a lamina and stay in the defect site. To resolve this issue, we developed a porous PCL cage scaffold that resembles the shape of a lamina (Fig. 1). PCL is a polymer that has excellent biocompatibility. It has been used in making tissue-engineering scaffolds for bone repair23–26 and also as suture (Ethicon's Monocryl®). The morselized bone can be packed into the PCL cage and placed into the defect. We hypothesized that this osteogenic scaffold will be able to induce new bone formation so that the lamina bone can be regenerated.

Polycaprolactone lamina cage.
Materials and Methods
PCL lamina cage
The PCL porous cages were fabricated by 3D Biotek using its 3D Precision Microfabrication technology, a type of solid free-form fabrication process. The PCL (Mw 43,000; Polysciences, Inc.) fiber in the PCL cage (Fig. 1) has a diameter of 300 μm and fiber-to-fiber distance (pore size) of 300 μm. The size of the cage is 1 cm (L)×0.8 cm (W)×0.4 cm (H). The cage was designed in such a way that the morselized bone chips can be packed into it through the openings at the two ends of the cage.
Surgical procedure
Animal experiments were approved by the Institutional Animal Care and Use Committee of the authors' university hospital. A total of 48 male rabbits (body weight 3–3.5 kg) were used in the study. Animals were grouped into four groups according to the implant to be used (Table 1). All rabbits were kept in their cages for 7 days before surgery. General anesthesia was administered with injection of 35 mg/kg ketamine hydrochloride and 15 mg/kg xylazin hydrochloride, intramuscularly.
Animal Experimental Groups and Sacrificing Schedule
After the rabbits were anesthetized and placed in a prone position, a midline skin incision was made. The lumbosacral fascia was then incised, and the paraspinal muscles were subperiosteally detached to expose the L4 and L5 lamina. Laminectomy was performed at L4 using an electric drill. Morselized autologous bone chips were obtained from morselzing the removed lamina and used either directly or filled into the PCL devices to form the hybrid implants. Iliac autologous bone was harvested from crista iliac during the surgery.
Implants were placed into lamina defects, except for the control group, which received no implants. All wounds were closed by following routine closure procedures. Fascia and skin incisions were sutured with nylon sutures.
The rabbits were sacrificed at 5 and 10 weeks after the surgery. The sacrificing process was performed with the sodium pentothal solution in 60 mg/kg doses. The paravertebral region was exposed, and the vertebral column, including the paraspinal muscle system, was resected in an en bloc fashion with an osteotome. Within each group, three of the rabbits were used for histological and immune-biochemistry (bone turn-over markers) analysis. The other three rabbits were sacrificed for X-ray, micro-CT, and mechanical testing to study the bone regeneration process.
Histology
After sacrificing, the spine specimens were visually examined before fixation. For histology, the tissue samples were fixated with 10% formaldehyde solution for 2–3 days and decalcified with 10% nitric acid. After decalcification, tissue samples were processed to obtain sections of 5-μm thickness. The sections were stained with hematoxylin and eosin.
Bone turnover markers
Bone turnover markers, that is, serum osteocalcin and serum collagen type I cross-linked C-terminal telopeptide (CTx), were chosen to study the bone resorption and regeneration process. Blood samples were drawn from the aorta of the rabbits before sacrificing. Osteocalcin, a bone formation marker, and serum collagen type I CTx, a bone resorption marker, were analyzed using commercially available enzyme-linked immunosorbent assay kits.
X-ray imaging
After sacrificing, three of the animals from each group were used for X-ray imaging. The bony defect and the reconstructed lamina with grafts were imaged with X-ray using a Faxitron Specimen Radiography System, Model MX-20.
Biomechanical testing
Biomechanical tests were performed on the spinal L4–L5 specimens (Fig. 2). A Shorewestern306 biomechanical tester was used. The range of motion (ROM) was measured under a fixed torque of 0.3 Nm. A 3D infrared sensor was used to capture the displacement and bending angle.

Biomechanical testing setup.
Results
Bone turnover markers
At week 5, the contents of serum CTx in all experiment groups were all significantly higher than that of the control group (Table 2 and Fig. 3). At week 10, the content of serum CTx further increased in all experimental groups, with the iliac group as the highest, whereas the control group did not show a significant increase.

Content of serum cross-linked C-terminal telopeptide in animal groups at both weeks 5 and 10.
Content of Serum Cross Linked C-Terminal Telopeptide
Significant difference between test and control groups.
The serum content changes of CTx in all experimental animal groups suggested that there were much more active bone resorption processes going on in all experimental groups than in the control group. The bone resorption processes were still very active at week 10. The results also suggested that all autologous bone grafts are being resorbed during the bone regeneration process.
Serum osteocalcin is a bone formation marker that represents the bone formation process, because osteocalcin is solely secreted by osteoblasts. As can be seen from Figure 4, at 5 weeks, all experimental groups showed a significant higher osteocalcin content than that of the control group, indicating that the animals with autologous bone implants were having a very active bone regeneration process than animals without implants. Among the experimental groups, animals with cage implant showed the highest osteocalcin content than both morselized bone and iliac bone groups. At week 10, there were further increases in all groups, including the control group. This indicated that the bone regeneration process is still ongoing in all animals with or without implants.
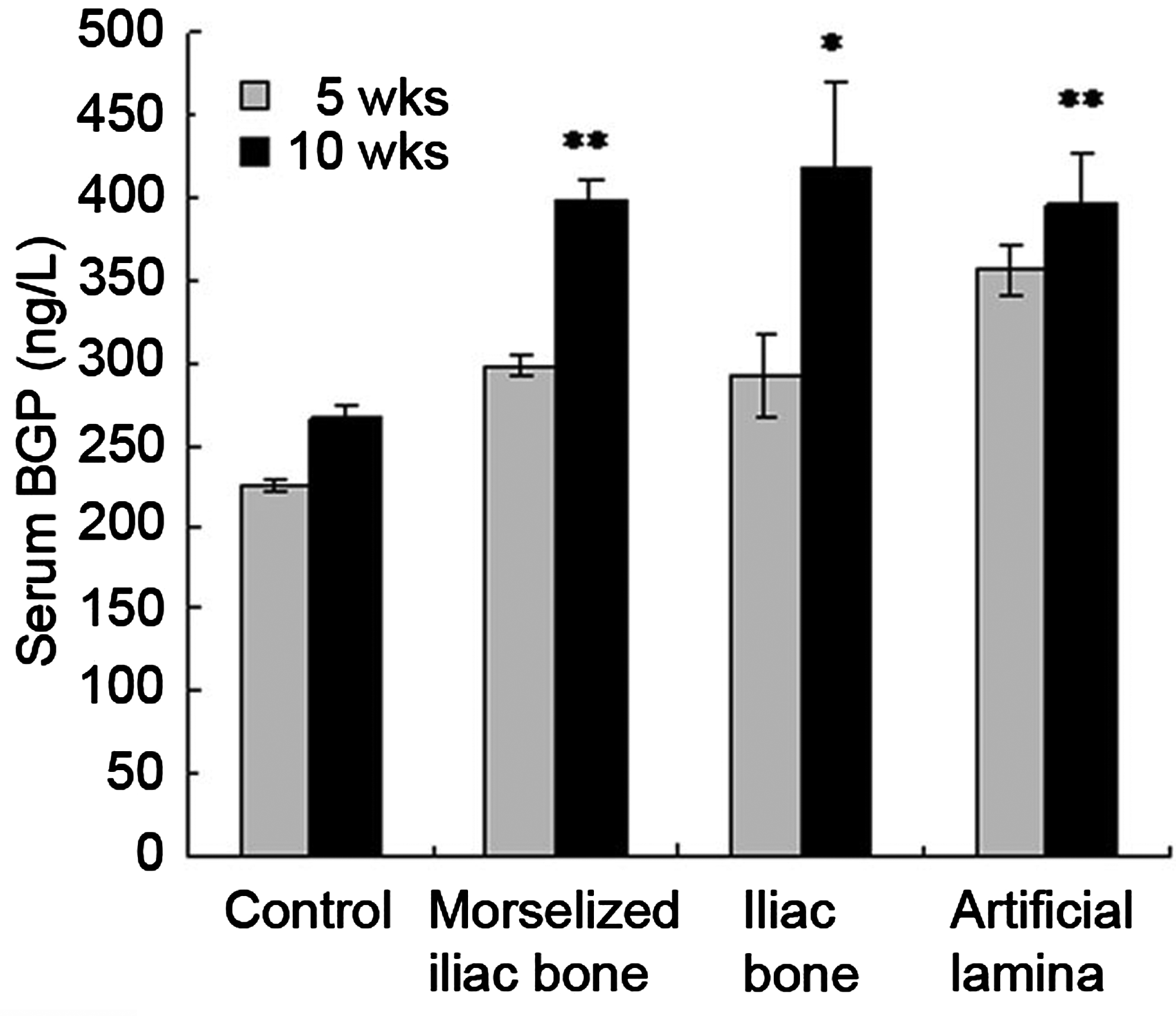
Osteocalcin content at weeks 5 and 10 in all experimental groups. *,**Significant difference between weeks 5 and 10.
Combining the serum content of both CTx and osteocalcin, it can be concluded that all animals with bone grafts had a very active bone-remodeling process: on one hand, bone grafts were actively resorbed; on the other hand, the new bone formation processes were significantly enhanced by the presence of autologous bone grafts.
Visual examination of explants
Gross examination showed that the cage implant had good fusion with the neighboring bone at week 5 (Fig. 5A). The cage implant was found to be firmly integrated in the defect site when examined using fingers. Excellent integration with neighboring bone with bone callus formation on the implant was observed at week 10 (Fig. 5B), indicating that the new bone formation was still ongoing beyond week 5.

Gross examination of the cage implant at weeks 5 and 10.
X-ray imaging
The bony defect and the reconstructed lamina with grafts were imaged with soft X-ray.
In Figure 6, an intact lamina structure can be seen in the normal group. In the control group, it was observed that the bony defect could not be completely repaired even at week 10. On the other hand, at both weeks 5 and 10, the bony defects were completely filled by bone masses that were from both autologous bone grafts and newly formed bone. More detailed observation showed that there was more osteogenesis in the treated areas at week 10 in morselized iliac bone, iliac bone, and PCL cage implant groups.

Lateral view of L4–L5 vertebrae at 5 and 10 weeks after the surgery by soft X-ray. The white short arrows indicate the morselized bone, and white long arrows indicate the iliac bone. Artificial laminas are marked in white round circles. N, normal; C, control.
Biomechanical testing
For the explants at week 10, it was found that under a fixed torque of 0.3 Nm, there were no significant differences in ROMs among the normal, iliac bone, and cage implant groups (Fig. 7), indicating that the mechanical properties of the spine were better restored with the iliac bone and PCL cage implants. On the other hand, both the control group and the morselized iliac bone group showed a much lower ROM than that of the normal group. Also, both groups of iliac bone and artificial lamina showed significantly higher ROMs than that of control group (p=0.03).

Range of motion of week-10 L4–L5 specimens.
Overall, these biomechanical test results indicated that both the iliac bone and cage implants promoted more new bone formation so that a better motion restoration effect could be achieved.
Histology
For control group animals, significant scar tissue or epidural fibrosis formation was found in the bony defects. No new bone formation was observed in the defects.
The interface between the grafts and medulla spinalis (Fig. 8) as well as the interface between graft and host bone (Fig. 9) were studied. Histology revealed that the spinal canal was better maintained in the iliac group at both weeks 5 and 10 (Fig. 8C1, C2). No adhesions and epidural fibrosis were found. New bone formation increased from week 5 to week 10 (Fig. 9C1, C2).
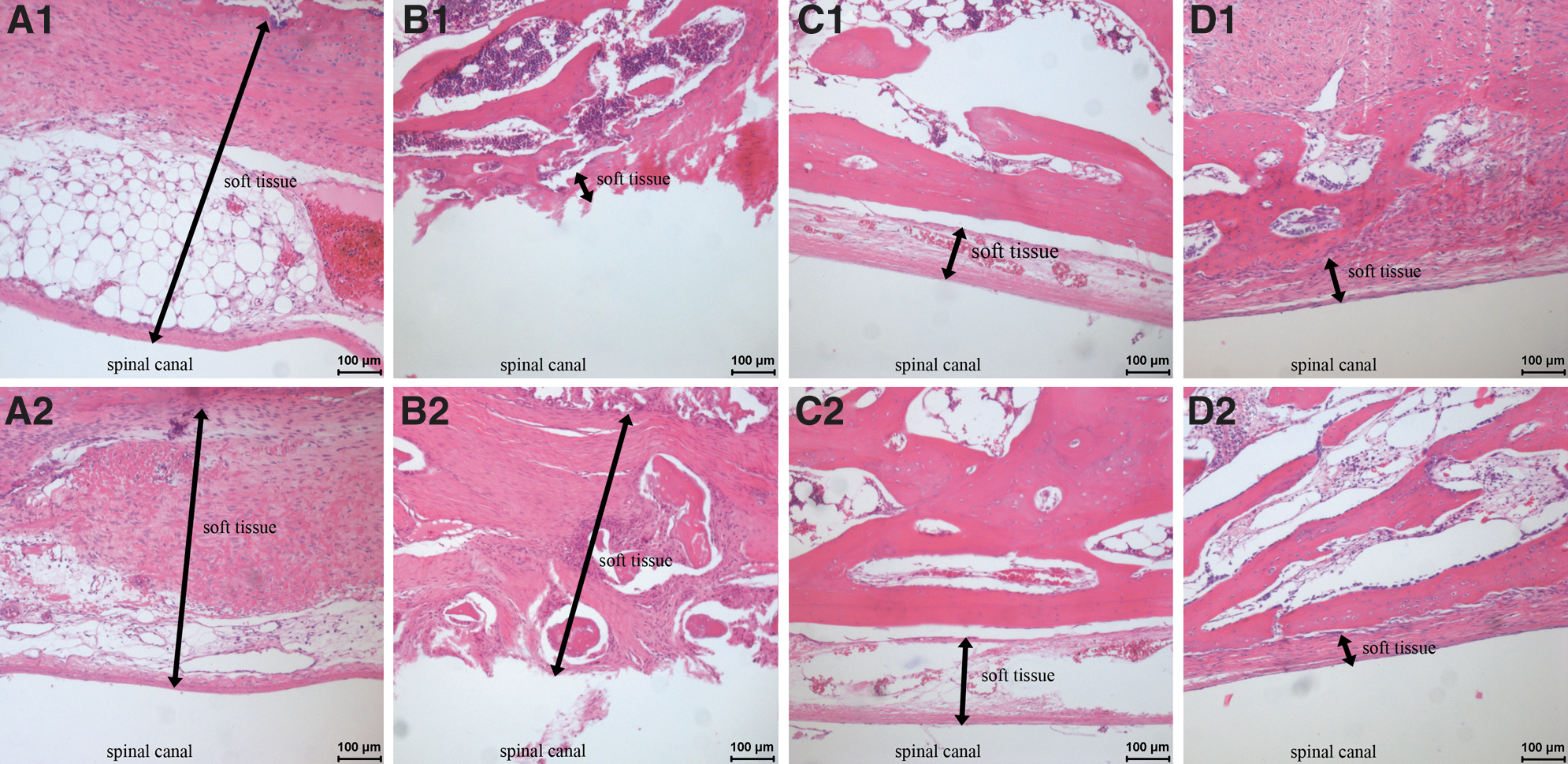
Histology of experimental groups: interface between grafts and medulla spinalis.
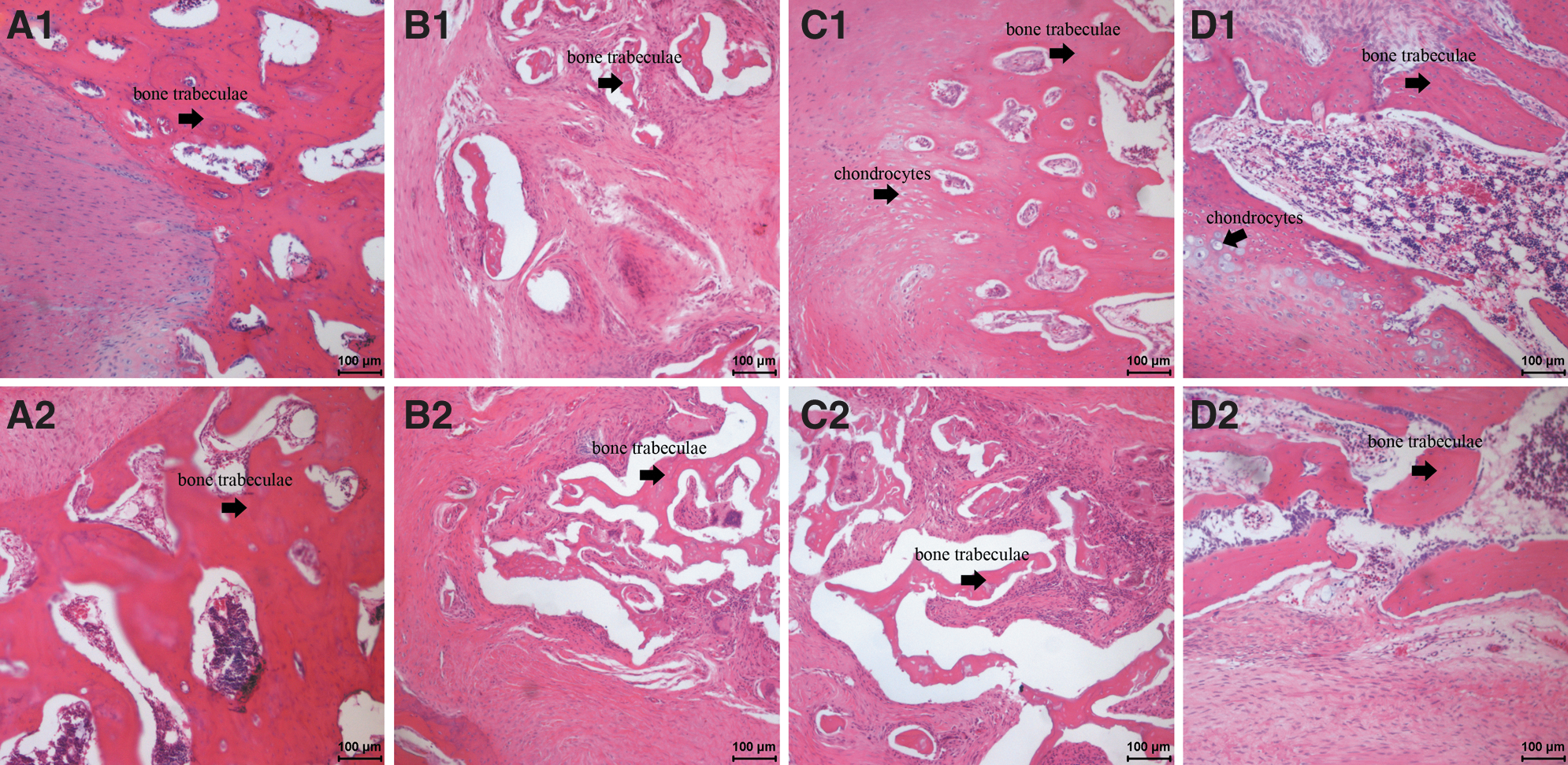
Histology of experimental groups: interface between grafts and host bone.
In the morselized group, it was found that the spinal canal had rough surfaces. At both weeks 5 and 10, significant epidural fibrosis was found (Fig. 8B1, B2), which resulted in narrowing of the spinal canal (spinal canal stenosis). Extensive soft tissue formation was found in the morselized bone group. Voids were formed due to the quick disappearance of the morselized bone. Scattered new bone formation can be found (Fig. 9B1, B2).
In the cage implant group, the spinal canal was better maintained with a smooth canal surface (Fig. 8D1, D2). Extensive new bone formation and penetration from neighboring bone were found. Scattered chondrocytes were found at the interface of new bone and host bone. More bone formation and bone contact were found at week 10 than at week 5 (Fig. 9D1, D2).
Discussion
In this study, an osteogenic scaffold was developed that composed of a porous PCL cage and filled with osteogenic bone graft particles. The hybrid scaffold was evaluated in a very challenging rabbit total laminectomy model because the full reconstruction of lamina is still a very challenging task due to the complicated anatomy structure and location of lamina. Using morselized autologous lamina bone particles as osteoinductive bone graft will have wide clinical implications, because the surgically removed lamina is often discarded as a medical waste in the current clinical practice.
PCL is a totally bioabsorbable polymer that has been extensive studied as bone tissue-engineering scaffolds.23,24,26,27 It has excellent biocompatibility and will be absorbed completely in vivo in about 24 months. Therefore, it was chosen as the material for fabrication of the cage scaffolds.
To demonstrate the feasibility of using the cage scaffolds for bone reconstruction, a total of three types of implants, that is, morselized iliac bone, iliac bone, and PCL cage filled with morselized bone grafts, were implanted into rabbits for up to 10 weeks after total laminectomy of L4–L5. Because all these implants were mainly composed of autologous bone, therefore, it is expected that these autologous bones grafts will go through bone resorption and bone regeneration processes. Bone turnover markers, that is, serum osteocalcin and serum collagen type I CTx, were chosen to study the bone resorption and bone regeneration processes.
Serum content of CTx is a bone resorption marker. It has been extensively studied in diseases that are associated with markedly high levels of bone turnover, such as Paget's disease, primary hyperparathyroidism, glucocorticoid-induced osteoporosis, or renal osteodystrophy.28–35 Collagen cross links are generally reliable markers of bone resorption, because they are stable in serum and urine. Collagen cross links bind three molecules of collagen in the bone and are released from the bone matrix after resorption, either free or bound to the N- or C-telopeptide of collagen.
In this study, it was found that at both weeks 5 and 10, the contents of serum CTx in all experiment groups were all significantly higher than that of the control group (Table 2 and Fig. 3). The content of serum CTx increased further from week 5 to 10, with the iliac group as the highest.
The serum content changes of CTx in all experimental animal groups suggested that there were much more active bone resorption processes going on in all experimental groups than in the control group. The bone resorption processes were still very active at week 10, suggesting that there were still autologous bone chips presented in the implant site at week 10, and the bone remodeling process was still active.
Serum osteocalcin is a bone formation marker that represents the bone formation process, because osteocalcin is solely secreted by osteoblasts. It has been found that higher serum osteocalcin levels are well correlated with the increases in the bone mineral density during treatment with anabolic bone formation drugs for osteoporosis. 34 Osteocalcin has been used as a preliminary biomarker on the effectiveness of a given drug on bone formation.
The osteocalcin level increased in all experiment groups as expected. As can be seen from Figure 4 at 5 weeks, all experimental groups showed a significantly higher osteocalcin content than that of the control group, indicating that the animals with autologous bone grafts were having a very active bone regeneration process than those without autologous implants. Among the experimental groups, animals with PCL cage implants showed the highest osteocalcin content than both morselized bone and iliac groups. At week 10, there were further increases in the serum osteocalcin content in all groups, including the control group. These results indicated that the bone regeneration processes were still ongoing at week 10 in all animals with or without implants.
Combining the results of serum content of both CTx and osteocalcin, it can be concluded that all animals with bone grafts were having a very active bone-remodeling process.
X-ray image showed changes of the lamina bony defect over time. Normal lamina showed a dense intact bone structure (Fig. 6). In the control group, the bony defect was not completely filled even at week 10 because of the lack of new bone formation. On the other hand, at both weeks 5 and 10, the bony defects in the morselized iliac bone group showed that they were filled with a bone mass. The iliac bone group showed that the bony defects were completed filled by a bone mass even at week 5 because of the presence of a single piece of iliac bone. In the cage implant group, the progress of the new bone formation can be clearly seen from the X-ray images at weeks 5 and 10. A much denser bone mass was observed for the cage implant group at week 10. Overall, the X-ray image showed that the bone defects can be restored by the iliac and cage implant groups.
One of the important aspects of the lamina reconstruction is to restore the spine's normal mechanical properties. To evaluate its biomechanical properties, a mechanical torque test was performed on the spinal L4–L5 specimens after 10 weeks of implantation.
It was found that under a fixed torque of 0.3 Nm, there were no significant differences in ROMs among the normal, iliac bone, and cage implant groups (Fig. 7), indicating that an excellent bone regeneration and bone integration happened in these two groups. On the other hand, both the control group and the morselized iliac bone group showed a much lower ROM than that of the normal group. These results indicate that both the iliac bone and cage implants have a better motion restoration effect, which were the results of better lamina reconstruction.
The histology study showed that the spinal canal was better maintained in the iliac group at week 5 (Fig. 8C1, C2). No adhesions and epidural fibrosis were found. New bone formation increased from week 5 to 10 (Fig. 9C1, C2), indicating that the iliac bone grafts have excellent osteoinductivity.
In the cage implant group, the spinal canal was also better maintained with a smooth surface (Fig. 8D1, D2). Extensive new bone formation and penetration were found in the cage implant group too (Fig. 9D1, D2), indicating that the cage implant had excellent osteoinductivity. Its osteoinductivity should come from the morselized autologous bone particles that were packed into the PCL cage scaffolds. Scattered chondrocytes (Fig. 9D2), usually an indication of an early stage of new bone formation, were observed at the interface between newly formed bone and host bone in the artificial lamina group. More bone formation and bone contact were found at week 10 than at week 5.
In contrast to above two groups, the morselized bone group showed extensive soft tissue formation within the bony defect. Voids were formed (Fig. 8B1, B2) probably due to the disappearance of the morselized bone particles, either by absorption or by the dislocation of the bone particles. Only scattered new bone formation was found (Fig. 8B1, B2).
From the histology study, it is evident that both the iliac and PCL cage implants are good bone grafts for lamina reconstruction.
Above results suggested that it is feasible to restore the bone shape and anatomic shape using a prefabricated polymer cage packed with osteoinductive bone grafts, such as autologous bone chips, allogeneic DBM particles, and growth factor-loaded beads. The bioabsorbable polymer PCL cage with a patient-specific defect matching the size and anatomic shape can be prefabricated with computer-aided design–based solid free-form fabrication technology to restore the missing bone segment to its original size and anatomic shape. Hence, this platform technology should have wide applications in orthopedic, craniofacial, and plastic surgery.
Conclusion
An osteogenic bone tissue-engineering scaffold for bone reconstruction/regeneration was developed and evaluated in a rabbit total lamina defect model. The scaffold is composed of a totally bioabsorbable PCL polymer cage and filled with osteoinductive autologous bone particles. When compared to the autologous iliac bone and morselized iliac bone grafts, the PCL cage with autologous bone chips showed comparable results to the autologous iliac bone graft in terms of its capability to repair the lamina defect and restore the biomechanical stability.
Therefore, the newly developed PCL cage implant showed a great promise as an alternative to autologous bone graft, because it does not need a second iliac bone-harvesting surgery, and thus the morbidity and the possible infections that are often associated with the bone harvesting surgery can be avoided.
Footnotes
Author Disclosure Statement
No competing financial interests exist.