
Abstract
Background:
Today, no consensus exists regarding how human tissues are best preserved for long-term storage. Very low temperature storage in liquid nitrogen is often advocated as the superlative method for extended periods, but storage in −80 degrees Celsius (−80°C) freezers, while sometimes debated, is a possible alternative. RNA is the most easily degradable component of a biological sample in a molecular biology context and the quality can reliably be measured.
Aim:
To investigate to what extent long-term storage of tissues in −80°C affects the RNA quality and overall histomorphology. The tissue storage period represents nearly three decades (1986–2013).
Methods:
RNA extraction from 153 tissue samples with different storage periods was performed with the mirVana kit (Invitrogen). RNA integrity was assessed using an Agilent bioanalyzer to obtain RNA integrity numbers (RIN). Further, tissue representative testing using light microscopy was performed by two pathologists to assess tissue composition and morphology.
Results:
RIN values were measured in all samples, showing a variability that did not correlate with the storage time of the tissues. Microscopically, all samples displayed acceptable tissue morphology regardless of storage time.
Conclusion:
Long-term storage in −80°C does not adversely affect the quality of the RNA extracted from the stored tissues, and the tissue morphology is maintained to a good standard.
Introduction
E
In 2012, a Chinese group studied RNA from tissues collected over a 40-month period and obtained RIN values ≥7 for all samples, 7 but studies including long-term stored tissue samples are lacking. An article published in 2013 assessed the RIN values in blood samples stored for 4–19 years at −80°C in Sweden and for 11–19 years in liquid nitrogen in Italy and found no observable systematic effect of storage time. 8
Multiple factors at various stages—from excision during surgery to subsequent gene expression analysis—may potentially affect the quality of the sample and the experimental results. These factors include anesthesia type, surgical procedure (manipulation and time of ischemia during operation), transport method, preservation routine, the occurrence of freeze-thaw cycles, and storage length. 9 Furthermore, RNA may be degraded through exposure to heat, UV, urea, salts, and results may also vary with different methods of RNA extraction. 10
Regarding transport, a Brazilian group concluded in 2012 that cold ischemia time no longer than 30 min was superior for maintaining RNA integrity compared to longer ischemia time. 11 In 2009, Johnsen et al. concluded that overall RNA quality was similar when comparing samples stored after snap-freezing to treatment with RPA (RNA preserving agent). 12 Several authors and groups have tried to standardize the collection of human frozen samples for research. In 2008, a complete European infrastructure for the exchange of frozen tumor samples was introduced, named OECI TuBaFrost. It consists of a virtual microscopy database and a code of conduct on how to exchange samples. 13
In general, long-term preservation of biological tissues demands the indisputable inhibition of biological and enzymatic processes to protect and preserve the structure of those molecules one wishes to study. In broad terms, the glass transition point (Tg) of organic compounds (liquid to solid matter, ranging from −90 to −140°C) is generally accepted as a critical temperature level at which most (if not all) biological processes demanding enzyme-driven activity are brought to halt. As a consequence, freezing and preserving biological specimens in liquid nitrogen (−196°C) would in theory keep the samples at least 60°C below this critical level, which in turn would give a large margin in the event of extensive fluctuations in temperature. On the downside, maintaining samples in liquid nitrogen tanks is more expensive compared to standard preservation in −80°C freezers, and present some work environment hazards. At present, no clear consensus exists on how to store biological samples effectively for long-term uses from biomolecular, economical, as well as practical points of view. The tissues' storage time in the freezer should also be taken into consideration, as longer storage times may result in deteriorating tissue quality due to intrinsic (enzyme activity, dehydration) and extrinsic factors (freezer malfunction, improper temperature ranges, freeze drying, and/or thawing of the samples during removal from the storage tubes).
We have consequently stored human endocrine tumors as fresh frozen samples exclusively in −80°C freezers (Forma Freezers, Thermo Scientific). The oldest samples were collected in 1986, meaning 27 years of storage prior to extraction, performed in 2013. In the current study, RNA from 153 tissue samples from this time period was extracted and its integrity was validated using a bioanalyzer. We specifically aimed to establish; 1) whether long-term preservation at −80°C is adequate to maintain good quality RNA and tissue morphology in tissue samples; and 2) will this storage option proportionally and negatively affect the quality of RNA from endocrine tissue samples over a period of time spanning almost three decades?
Materials and Methods
Samples, nucleic acid extraction, and quantification
The study comprised a total of 153 tissue samples, including 86 pheochromocytomas (PCC), 14 paragangliomas (PGL), 25 adrenocortical cancers (ACC), 11 anaplastic thyroid cancers (ATC), and 17 cases with normal adrenal gland tissue (nADR) adjacent to tumors collected from patients undergoing surgery at Karolinska University Hospital, Stockholm, Sweden during 1986–2011 (Table 1). All samples were collected with informed consent, with ethical permits for the adrenal and the thyroid samples, approved by the Regional Ethical Review Board in Stockholm (ID: 01-136 and ID: 03-517, respectively).
ACC, adrenocortical carcinoma; ATC, anaplastic thyroid carcinoma; nADR, normal adrenal gland; PCC, pheochromocytoma; PGL, paraganglioma.
The samples were collected through the established biobank organization where an experienced pathologist identified and macro-dissected the tumor and normal tissue. All samples included were divided in pieces and individually snap-frozen in liquid nitrogen and thereafter stored at −80°C without thawing. The pieces (6–8/tube) were stored in standard high density polypropylene cryotubes 14 with a small rubber o-ring sealing, as exemplified by the NUNC 2.5 mL CryoTube (Sigma-Aldrich, St. Louis, MO, USA). This method prevents desiccation of the tissue and facilitates rapid removal of a single sample piece from the tube without the risk of thawing the other samples. We do not use Tissue-Tek O.C.T or similar compounds to cover the tissue pieces.
RNA quality was assessed following extraction from fresh frozen tissue samples using the mirVana miRNA Isolation Kit (Ambion/Invitrogen, Carlsbad, CA, USA). RNA quality was measured using an Agilent 2100 Bioanalyzer (Agilent, Santa Clara, CA, USA) with the RNA Nano 6000 chips and reagents (Agilent) obtaining RIN values as summarized in Table 1 and detailed in Supplementary Table S1 (supplementary material is available online at www.liebertpub.com/bio). Statistical calculations (Spearman's rank-ordered correlation coefficient (Rho)) were made with STATISTICA v10 (STATSOFT Scandinavia, Sweden), and Figure 1 was generated with Think Cell (think-cell Software GmBH, Germany).
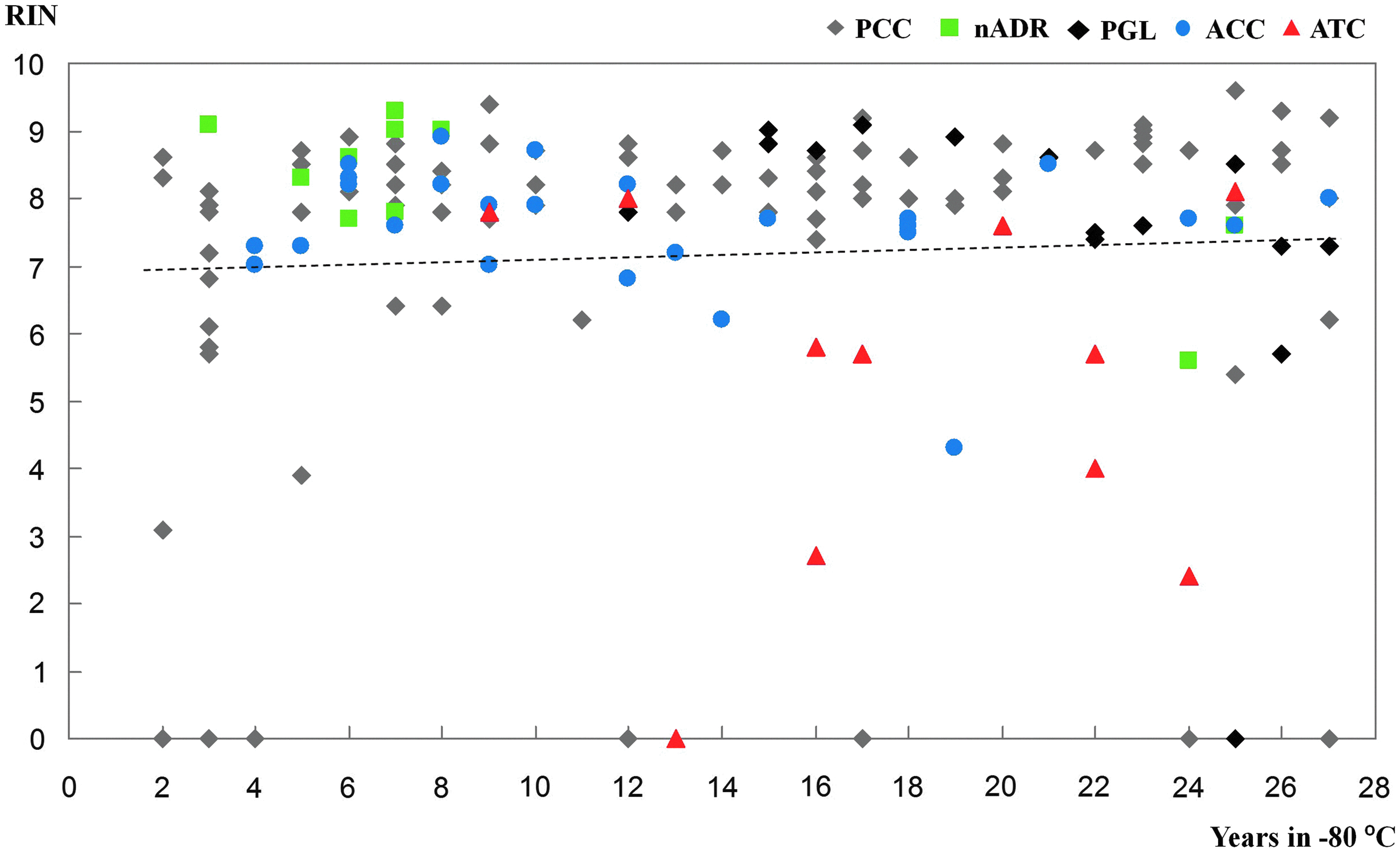
Scatter plot with trend line comparing RIN values and years in −80°C freezer. RIN values were measured in all samples, showing a spread that did not correlate with the storage length of the tissues [Rho=0.075, p=0.36]. A slight increase in RIN values was seen in older samples. This seems contradictory but is explained by gradually changed routines with optimal specimen handling in direct connection to the operation theatre during the first decade. ACC, adrenocortical carcinoma; ATC, anaplastic thyroid carcinoma; nADR, normal adrenal gland; PCC, pheochromocytoma; PGL, paraganglioma. A color version of this figure is available in the online article at www.liebertpub.com/bio.
Histological confirmation of the analyzed samples
A small representational and morphology piece was removed from 86% of all analyzed samples. The piece was thawed and routinely fixed in neutral-buffered 4% formaldehyde solution, embedded in paraffin, sectioned, and stained with haematoxylin and eosin. Tumor and normal cell content was determined by two expert pathologists independently. Representativeness was defined as samples with tumor or normal cell content of more than 70%. Retained morphology was specified as the characteristic cytological and structural appearance for respective tumor or cell type. Criteria such as autophagy, nuclear integrity, and autolysis was considered, and overall morphology were evaluated in a three grade scale as “excellent,” “acceptable,” or “bad” retained morphology.
Freezers, storage temperatures, and variations
In the first decade of the 27-year period during which the current samples were collected for the biobank, the specimens were processed in a laboratory connected to the surgical facilities that facilitated efficient handling of the tissues. Around 1996, the organization for collecting the samples gradually changed, and the specimens are now transported directly from surgery to the Department of Pathology in a pneumatic tube system; or if larger, by internal staff at the hospital. Post-surgically, the samples were examined immediately by the pathologist on duty who decided which part of the sample should be preserved in the biobank. The same pathologist was also responsible for the final diagnosis.
Results
We have assessed the quality of RNA from 153 tissue samples, obtaining RIN values for all cases as summarized in Table 1, detailed in Supplementary Table S1, and plotted in Figure 1. In accordance with our hypothesis, the RIN values did not correlate with the storage time of the tissues [Rho=0.075, p=0.36]. Within individual tissue groups, some significant correlations were found between storage time and RIN values for the PCCs and PGLs [Rho=0.367, p=0.0005 and Rho=−0.739, p=0.0025 respectively], but not for the nADRs, ACCs or ATCs as detailed in Table 2. Slightly higher RIN values were found in samples collected in the beginning of the collection period (Fig. 1 and Table 1). This might be explained by gradually changed routines with optimal specimen handling in direct connection to the operation theatre during the first decade. The anaplastic thyroid cancers show lower RIN values in general (Table 2), which may be explained by pre-surgical combined radio- and chemotherapy causing extensive necrosis and fibrosis.
ACC, adrenocortical carcinoma, ATC, anaplastic thyroid carcinoma, nADR, normal adrenal gland, PCC, pheochromocytoma, PGL, paraganglioma, Rho, Spearman's rank-ordered correlation coefficient.
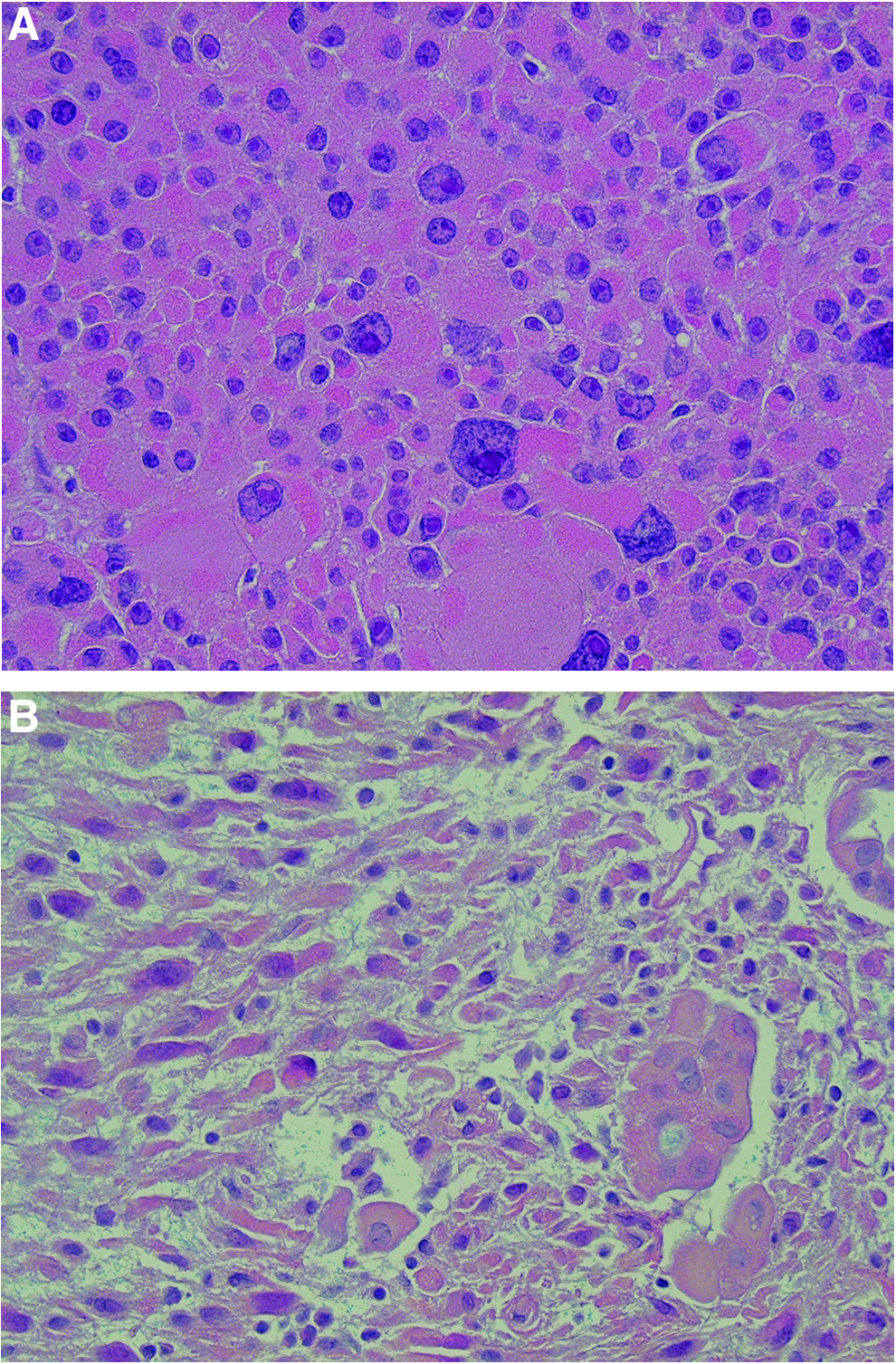
No evidence of lyophilizing of tissues was observed. Representativeness workup revealed tumor or normal cell content more than 70% in 88% of the cases (Supplementary Table S1). Morphology workup revealed “excellent” or “acceptable” tissue morphology in all cases studied (Supplementary Table S1). There was no correlation between the state of the tissue morphology and RIN numbers. A representative photomicrograph of a hematoxylin-eosin stained section from a sample stored 27 years in −80°C with “excellent” tissue morphology is shown in Figure 2A. A case of anaplastic carcinoma, stored since 1993, with ”acceptable” tissue morphology, most likely caused by combined extensive radiological and cytotoxic therapy pre-operatively is shown in Figure 2B.
Discussion
We have extracted and assessed RNA quality from a large number of tumors and normal tissues collected over the past 27 years (Table 1). Our results suggest that long-term storage in −80°C does not adversely affect the quality of the RNA extracted from the tissues.
Interestingly, the RIN values increase slightly with the storage time, and this is probably explained by faster tissue handling after surgery during the initial period of sample collection when a pathologist could be stationed close to the operation department. This might be put in context with additional procedures for postoperative documentation and/or intensified work load on the pathologist on call in recent years, thus prolonging the processing time and hence the time before final freezing of the biobank sample. Our conclusions were drawn from analyzing endocrine tissue samples consisting of tumor pieces from both the adrenal and thyroid glands, respectively, meaning there is little chance for tissue type bias when analysing our results.
When comparing RIN values with storage time from all extracted samples, no correlation was found, as in concordance with our hypothesis. Within individual tissue groups (PCCs and PGLs), some significant correlations were found with more virtually intact RNA among older samples for the PCCs and more degraded RNA among older samples for the PGLs. Since the PGL samples are quite few, these results did not seem to affect the overall correlation. For the individual tissue groups; nADR, ACC and ATC, no correlations were found as in agreement with the hypothesis.
Optimally, our study would contain aliquots of tissues that were RIN tested at the initial time point of collection and through a defined set of intervals during the storage period; however such a design is not feasible in our case since the data were collected retrospectively. In addition, to verify the fact that our RIN values also reflect mRNA integrity in addition to overall RNA quality, a subset of the samples were subjected to qRT-PCR for housekeeping gene expression assays using the TaqMan system with high quality results (data not shown).
The amount of intrinsic RNase in a given tissue sample is a factor that could affect RNA integrity in long-term storage. RNase content in turn is affected by tissue type. Pancreas and spleen express by far the highest levels of RNases.15,16 As such, biopsies from these tissues could possibly benefit from preservation at temperatures below the glass transition point. Little data regarding RNAse activity in human endocrine glands are retrievable from the scientific community; however, a previous study showed that rat adrenal glands contain slightly higher RNAse activity than rat liver. 17 As the human liver exhibits moderate amounts of RNAse activity, it is fair to assume that human adrenal glands therefore contain moderate amounts of RNAse activity themselves. Human thyroid glands have been shown to express RNAse activity in the follicular epithelium but not in the colloid, 18 although no published quantitative data regarding comparison with other tissues were retrievable. A methodical analysis of different RNAse protein expression patterns in endocrine systems using the Human Protein Atlas (http://www.proteinatlas.org) was also conducted, in which normal adrenal and/or thyroid tissues, as well as thyroid carcinoma specimen, displayed moderate to strong expression of several RNAse proteins (such as RNAse subtypes 7, 9, 10, 11, and T2). It is therefore possible that our endocrine samples contain a significant amount of RNAse molecules, making the likelihood that our conclusions are drawn from long-term storage of RNAse-devoid samples unfounded.
The time the tumor is without blood supply during surgery may also affect RNA quality. In this study, the majority of the tumors are pheochromocytomas. During surgical removal, restriction of blood supply and blood drainage constitutes the first step of the tumor extirpation and causes a considerable time of hypoxia. In this sense, our sample composition includes tumors that are affected by extended hypoxia.
Another unknown factor of long-term storage in −80°C is whether tissue morphology is altered as a consequence of poor enzymatic inhibition in temperatures higher than the assumed glass transition temperatures, or by formation of ice crystals.
Perhaps somewhat surprisingly, the histomorphology was adequately retained to ensure representativeness and quality control. The possibility to perform quality control when the tissue samples are to be used instead of when they are stored makes it possible to charge the control cost to the end-users.
Long-term storage could also cause freeze-drying of the tissue. In our material, the vast majority of samples were sectioned and assessed by conventional light microscopy in addition to RNA extraction. The frozen samples were hydrated, firm, and easy to cut, thus proving that there were no freeze-drying effects during storage. Some authors recommend Tissue-Tek O.C.T. or similar compounds to prevent desiccation. We used that method in a limited number of samples during the early 1990s but experienced difficulties with RNA extraction, and therefore this method is now avoided.
Our results suggest that well-monitored and maintained freezers are capable of excellent preservation of high-quality RNA for decades. Due to endogenous ribonucleases, RNA is the most easily degradable component in tissues 4 and its undegraded long-term preservation in −80°C freezers indicates the unequivocal suitability of this storage routine. Thus, the results presented herein challenge the most valid argument to use liquid nitrogen storage, suggesting that freezers are equally suitable for long-term preservation of tissue samples—without the possible added cost and work environment hazards. No evidence of lyophilizing of tissues was observed in our samples, which could be explained by the small rubber o-ring sealed cryotubes and that several pieces are stored together, increasing the tissue volume in the tube and minimizing the risk of desiccation.
We conclude that long-term −80°C storage of endocrine tissue samples does not negatively affect the quality of enzyme-sensitive molecules such as RNA, or overall tissue morphology. Ultra-low freezing could therefore constitute a simple and safe alternative to liquid nitrogen storage.
Footnotes
Acknowledgments
The authors wish to thank Ms. Elisabet Ånfalk for excellent tissue management and Mr. Hampus Nestius for valuable Think Cell guidance.
Author Disclosure Statement
The study was partly financed by the StratCan (Strategic Research Programme in Cancer at Karolinska Institutet), the Swedish Cancer Foundation, the Cancer Society in Stockholm, and through the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet.
The authors declare that they have no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.