
Abstract
Objectives:
Describe pumping behaviors and pumped mother’s own milk (MOM) volume by achievement of secretory activation (SA; MOM sodium [Na] concentration ≤16 mM), coming to volume (CTV; ≥500 mL pumped MOM/day), SA maintenance (continued daily Na ≤16 mM), and opportunity costs in the first 14 postpartum days for pump-dependent mothers of preterm infants in the neonatal intensive care unit.
Methods:
A secondary analysis of two prospective cohorts. Mothers recorded pumping and MOM volume for each pumping session during the first 14 postpartum days. Daily MOM Na concentration was measured to determine SA. The opportunity cost was the dollar value of time spent pumping. Regression models evaluated pumping behaviors, pumped MOM volume, and opportunity cost by SA and CTV achievement and SA maintenance.
Results:
Of 66 mothers, 94% and 41% achieved SA and CTV, respectively, and 44% of mothers who achieved SA maintained it through 14 days postpartum. Mothers who achieved SA had more pumping sessions (5.6 versus 4.3/day, p < 0.001), longer pumping duration (108 versus 83 minutes/day, p < 0.001), and higher pumped MOM volume (349 versus 218 mL/day, p < 0.001). Mothers who achieved versus did not achieve CTV pumped 5.6 versus 4.9 times/day (p = 0.050). Opportunity costs were $376 for mothers achieving SA, $155 higher than not achieving, and $441 for mothers maintaining SA, $94 higher than not maintaining SA.
Conclusion:
Pumped MOM volume and opportunity costs were higher for mothers who achieved and maintained SA. Strategies offsetting opportunity costs during the stressful early postpartum period for breast pump-dependent mothers of preterm infants are needed.
Introduction
The vast majority of mothers of preterm (<34 weeks birth gestational age [GA]) infants initiate mothers’ own milk (MOM) feedings. 1 However, only 57% of extremely preterm (<32 weeks GA) and 52% of moderately preterm (32 to <34 weeks GA) infants receive any MOM at 3 months of age. 1 The lack of MOM through to and after neonatal intensive care unit (NICU) discharge increases risks of potentially modifiable complications of prematurity and their costs as well as postdischarge infections such as respiratory syncytial virus (RSV).2–6 However, long-term MOM provision is dependent upon receipt of MOM at NICU discharge, but many mothers are unable to provide a sufficient MOM volume to achieve this goal, despite an intention to do so. 7 The primary predictors of MOM receipt at NICU discharge are the early lactation achievements of secretory activation (SA; lactogenesis II, milk coming in) and coming to volume (CTV; ≥500 mLs MOM/day) by postpartum day 14. 8 Thus, the early postpartum period represents a critical window during which breast pump-dependent mothers of preterm infants must invest time and other resources to reduce the risk of longer-term infant health problems and their costs.
Although early pumping frequency is strongly associated with achievements of SA and CTV in this high-risk population,8–11 studies reveal that mothers of preterm infants do not pump as frequently as instructed. 12 Infrequent pumping may be partially modifiable through timely access to NICU-specific lactation care and effective breast pumps. However, unmodifiable is the fact that mothers are often sick themselves with comorbidities of preterm birth while simultaneously coping with the overwhelming stress of the NICU admission.9,10 They must balance trade-offs between time spent pumping and other essential activities, such as sleeping and recovering, caring for other family members, household responsibilities, self-care, and paid work. 13 Thus, an overlooked contribution to the early, unplanned cessation of lactation may be maternal opportunity costs—the time spent pumping that must be balanced with other unpaid and paid work. Few studies have examined the actual time investment and pumping behaviors of breast pump-dependent mothers of preterm infants in the NICU,12,14 and none have described the time and pumping behaviors needed to achieve SA and CTV and maintain SA.
This study sought to describe daily pumping behaviors as well as daily pumped MOM volume during the first 14 postpartum days for mothers who did and did not achieve SA and CTV. We also examined pumping behaviors and pumped MOM volume for mothers who maintained versus did not maintain SA once achieved. A final objective was to estimate the maternal opportunity costs of achieving SA, achieving CTV, and maintaining SA.
Methods
This was a secondary analysis of data from 66 breast pump-dependent mothers of preterm (<34 weeks GA at birth) infants from two prospective observational cohorts in which detailed serial data were collected daily for the first 14 postpartum days, including number and duration of pumping sessions and objective measures of SA and pumped MOM volume. Both studies were conducted in the same urban level III NICU in Chicago, with the studies conducted between October 2016 and April 2017 (cohort 1) and October 2019 and October 2020 (cohort 2), respectively.8,9 All participant mothers received evidence-based lactation care from a multidisciplinary team that included certified NICU breastfeeding peer counselors as the standard of care.15,16 The same hospital-grade double electric breast pump (Medela, Switzerland) was used for all pumping sessions in the maternity setting, the NICU, and at home. All mothers were instructed to use the initiation breast pump suction pattern until the pumped MOM volume was ≥20 mLs from the two breasts combined for two consecutive pumping sessions, then switch to the standard 2-phase pattern. 15 This study was approved by the University of Florida institutional review board (IRB202301833).
Sample
All mothers initiated lactation and reported a goal of providing exclusive MOM (i.e., no donor human milk or formula) for at least the first 14 postpartum days. Mothers were excluded if hormonal contraception and/or galactagogues were used or if their infant was unlikely to survive. This analysis excluded two mothers who were missing MOM Na data for ≥7 days in postpartum days 2–14. Four mothers who had missing MOM Na data after achieving SA were excluded from the analysis of SA maintenance (Supplementary Fig. S1).
Measures
Maternal and infant characteristics
Maternal and infant characteristics were retrieved from the hospital electronic medical record and maternal self-report. Maternal characteristics included age at delivery, race (Black, White, or other race), prepregnancy body mass index (BMI), 17 mode of delivery (vaginal, cesarean), lactation experience (any, none), and occurrence of maternal comorbidities of pregnancy such as preeclampsia and diabetes (yes/no). Infant characteristics included birth GA and sex.
Daily pumping behaviors and pumped MOM volume
Daily pumping frequency, total pumping minutes, and pumped MOM volume were recorded for postpartum days 2–14. Postpartum day 1 was excluded from the analysis because it did not represent a full 24-hour time period, and the amount of time varied across mothers depending on time of delivery. In cohort 1 (N = 38), mothers maintained paper pumping records with a standardized mother-friendly pumping log (My Mom Pumps for Me!®) that has been used in this team’s previous studies.7,14 These mothers collected pumped MOM in preweighed containers and brought the pumped MOM to the NICU, where they were weighed (Tanita, Japan) to the nearest 0.1 g by research team members. Pumped MOM volume was calculated by subtracting the prefilled container weight from the total weight and converting this value to mL (1 g = 1 mL). 18
In cohort 2 (N = 28), mothers used Smart Pumps (Medela, Switzerland) that incorporated electronic measurement, recording, and storage of the start and stop time for each pumping session. 9 Pumped MOM volume was weighed by the same digital scale as used in cohort 1, but the scale was integrated into the Smart Pump via a customized application so that mothers could perform MOM weights. These measures were stored until electronically transferred from the Smart Pump to a customized study database. Container weights were automatically subtracted from pumped MOM volume weights during data analysis.
Daily pumping frequency was defined as the number of separate pumping sessions recorded between 0000 AM and 1159 PM for postpartum days 2 through 14. For each postpartum day, we calculated the total pumping minutes and total pumped MOM volume by summing the individual pumping session data.
Handling of missing data
Mothers in cohort 1 recorded the number of pumping sessions but did not record the start and stop times for each session. For these mothers, we estimated daily total pumping minutes using a generalized linear regression model that controlled for pumping-specific variables, maternal characteristics, and infant characteristics. We evaluated five model specifications (Supplementary Table S1) and selected the optimal model based on the smallest mean squared error (model 2). The predicted duration of each pumping session was calculated based on the regression model coefficients and the actual values of the predictor variables for each mother in cohort 1. Daily total pumping minutes were calculated as the sum of the actual or estimated minutes for all pumping sessions on each postpartum day. Supplementary Table S2 reports the actual and predicted daily pumping minutes from the optimal model (model 2).
Achievement and maintenance of SA
For both cohorts, SA achievement was defined as MOM Na concentration ≤16 mM on any day during the first 14 postpartum days (yes/no). For mothers who achieved SA, we calculated the first day of SA achievement and whether SA was maintained on subsequent days, defined as MOM Na concentration ≤16 mM for all days between the first day of SA achievement and postpartum day 14 (yes/no). We analyzed both daily and overall SA achievement (defined as achieving SA on at least one day) for each mother.
For both cohorts, MOM Na samples were collected once or twice daily during the first 14 postpartum days by removing 1.8 mL of MOM from the original container(s) into which mothers had collected pumped MOM. For both cohorts, Na concentration was measured using selective ion electrode technology (Horiba, Japan) according to procedures delineated by Lai et al. 19
Achievement of CTV
Daily pumped MOM volume was used to determine CTV achievement (yes/no). A mother was considered to have achieved CTV if the daily pumped MOM volume was ≥500 mL on any day during the first 14 postpartum days. This analysis evaluated both daily and overall achievement of CTV for each mother.
Opportunity cost
To calculate the opportunity cost of providing MOM, we summed the total minutes spent pumping between postpartum days 2 and 14 and added 5 minutes per pumping session for cleaning equipment. The total time spent pumping was converted to hours and multiplied by $15 (Illinois minimum hourly wage rate as of January 2025) to calculate the total opportunity cost.
Statistical analysis
Descriptive statistics included frequency distributions, medians (interquartile range [IQR]), and means (standard deviation [sd]). Unadjusted mean differences in total pumping frequency, total pumping minutes, total pumped MOM volume, the first postpartum day that SA was achieved, percent of days SA was maintained, and total opportunity cost were calculated for SA achievement, CTV achievement, SA maintenance, CTV for mothers who achieved SA (SA without CTV, SA with CTV), and SA maintenance for mothers who also achieved CTV. To account for the skewed distribution of outcomes, 95% confidence intervals (CI) of the means were calculated using 10,000 bootstrap samples with replacement.
Line graphs were used to visually display the mean daily values of pumping frequency, pumping minutes, and pumped MOM volume by postpartum day and were stratified by SA achievement, CTV achievement, and SA maintenance. Additionally, heat maps were used to visualize the individual-level heterogeneity of daily pumping minutes and pumped MOM volume stratified by SA maintenance.
Generalized linear regression models were constructed to determine daily pumping behaviors and pumped MOM volume for achievement of SA and CTV. Models included the maternal and infant covariates most strongly associated with the respective outcome in bivariate analyses. Robust standard errors were used to account for correlation among repeated observations from the same mother. For each model, the optimal link function and distribution family were selected with the Pregibon link test and modified Park test, respectively.20,21 To isolate the effects of achieving SA and CTV, the method of predictive margins (also referred to as the method of recycled predictions) was used to calculate the predictive margin and marginal effect or adjusted outcome for all mothers, first assuming they achieved the outcome (achieved SA, achieved CTV, maintained SA), then assuming they did not achieve the outcome, holding all characteristics at their observed values.22,23 The difference in the adjusted outcome for each mother was calculated, and the mean difference (i.e., marginal effect) and corresponding 95% CI for the entire sample were reported.
Using a similar approach, generalized linear regression models were constructed to determine the total opportunity cost and marginal effects for (1) achieving SA and (2) achieving CTV and maintaining SA for mothers who achieved SA. Stata version 17 (College Station, Texas) and SAS version 9.4 (Cary, North Carolina) were used for statistical analyses.
Results
Sample characteristics
Table 1 describes the sample of 66 mothers. The median age was 30 years, more than half of mothers were Black (53%), and more than half had a BMI ≥27 kg/m2 (56%). 17 Supplementary Table S3 describes the sample by cohort.
Description of the Sample, N = 66
IQR, interquartile range.
Description of pumping characteristics, pumped MOM volume, and outcomes
Daily and total pumping behaviors, pumped MOM volume, achievements of SA and CTV, SA maintenance, and opportunity cost are described in Table 2. Pumping behaviors, pumped MOM volume, and opportunity costs by achievement of SA and CTV are reported in Supplementary Table S3. Over postpartum days 2–14, mothers pumped a mean of 4.8 (1.8) times and 91.3 (36.5) minutes per day. Over the 13 postpartum days, there was a cumulative mean of 61.7 (26.2) total pumping sessions and 1,172 (521) minutes per mother. Nearly all mothers achieved SA (93.9%), whereas only 40.9% achieved CTV. Of mothers who achieved SA, 43.6% maintained SA through to postpartum day 14. Overall, the mean opportunity cost of pumping MOM in the first two postpartum weeks, regardless of SA achievement, was $366 (156).
Description of Pumping Behaviors, Pumped MOM Volume, Secretory Activation, Coming to Volume, and Opportunity Cost for Postpartum Days 2–14, N = 66
CTV, coming to volume; IQR, interquartile range; MOM, mother’s own milk; Na, sodium; SA, secretory activation; sd, standard deviation.
Figure 1 depicts longitudinal trends in daily pumping behaviors and pumped MOM volume for achieving SA and CTV. Pumping behaviors differed visually for mothers who did versus did not achieve SA for most of the first 14 postpartum days. Pumping frequency differed visually for those who achieved versus did not achieve CTV, but pumping durations were similar. Daily pumped MOM volume was higher among mothers who achieved SA, with larger differences observed for those who achieved versus did not achieve CTV, due in part to the fact that CTV is defined as ≥500 mL of pumped MOM volume. Figure 2 reveals that the number of daily pumping sessions and total daily pumping minutes were significantly higher in postpartum days 3–14 for mothers who maintained versus did not maintain SA.
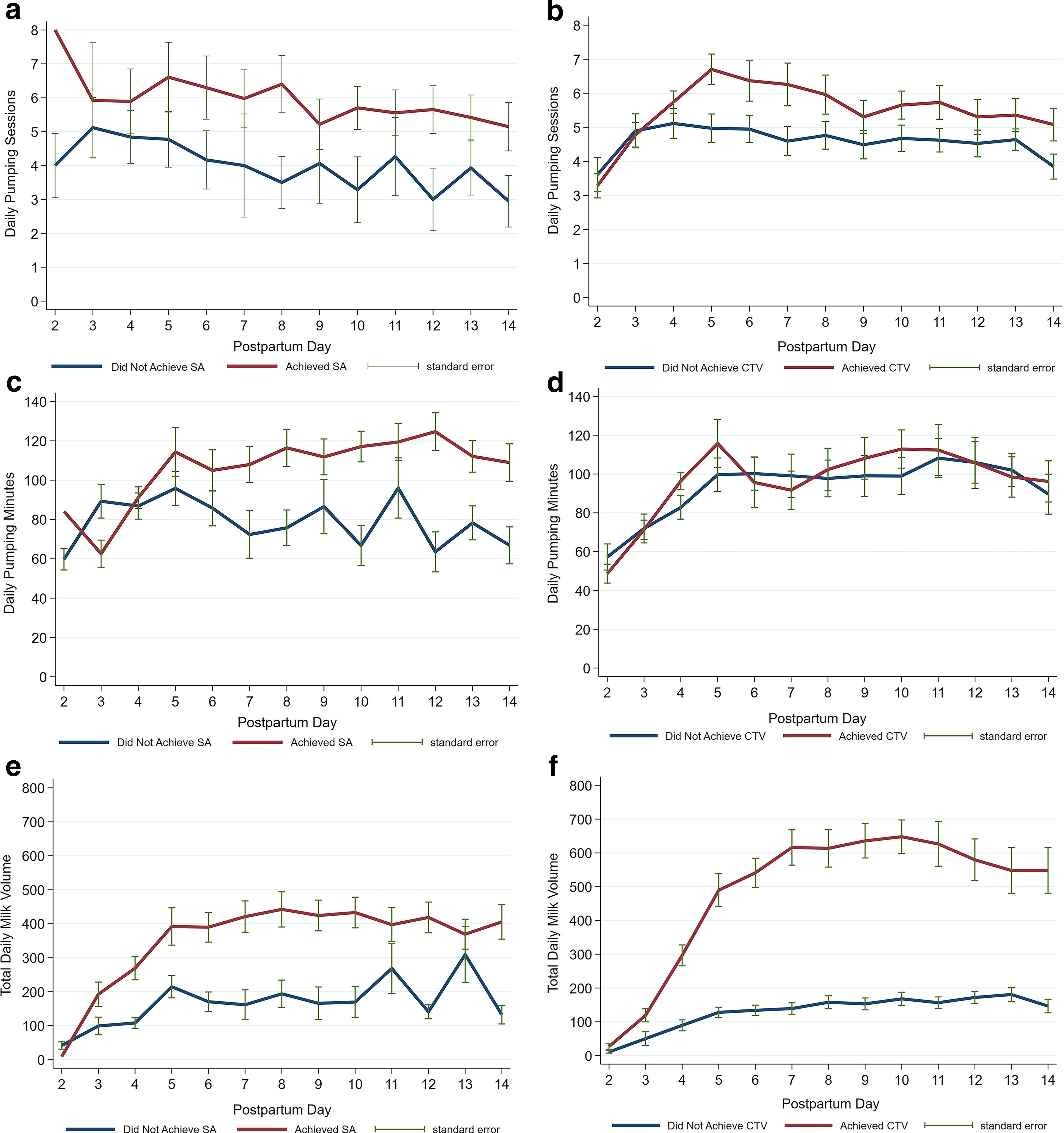
Mean pumping frequency, pumping minutes, and pumped mother’s own milk (MOM) volume by postpartum day and achievement of secretory activation (SA) and coming to volume (CTV).
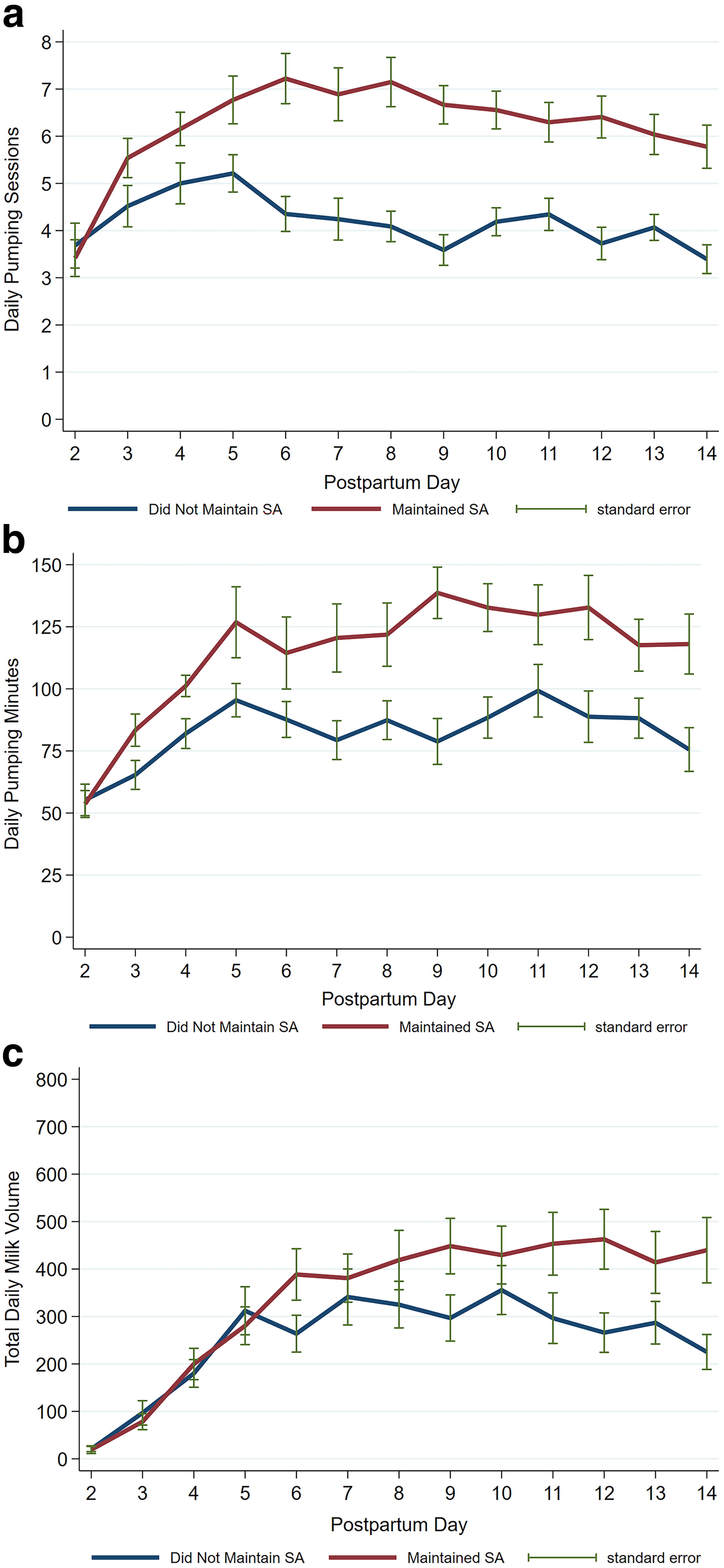
Mean pumping frequency, pumping minutes, and pumped mother’s own milk (MOM) volume by postpartum day and maintenance of secretory activation (SA).
The heatmaps in Figure 3 depict subject-specific pumping minutes and pumped MOM volume by postpartum day, stratified by SA maintenance. Figure 3a and b shows a greater concentration of days with ≥120 pumping minutes by mothers who maintained SA. For mothers who maintained SA, the heatmaps display relative consistency in pumping minutes, with many mothers pumping ≥120 minutes daily for multiple consecutive days. In contrast, mothers who did not maintain SA show greater variation in pumping minutes across days. Figure 3c and d shows similar patterns in daily pumped MOM volume between mothers who maintained versus did not maintain SA.
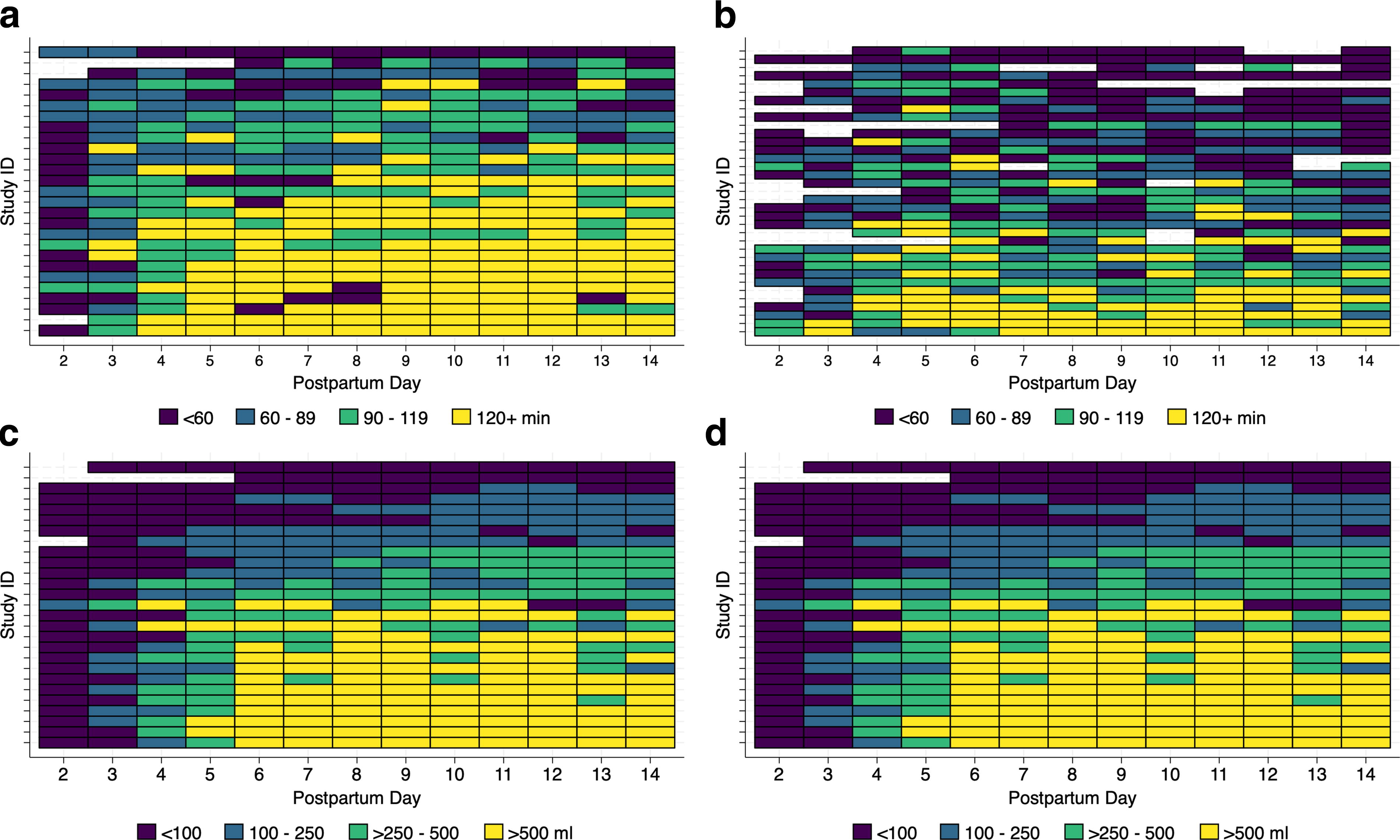
Heat maps of daily pumping minutes and daily mother’s own milk (MOM) volume by maintenance of secretory activation (SA).
Adjusted pumping behaviors, milk volume, and opportunity costs
After adjusting for maternal and infant characteristics, the mean daily pumping frequency across postpartum days 2–14 was 5.6 (95% CI: 5.2–6.1) if SA was achieved and 4.3 (95% CI: 3.9–4.8) sessions if SA was not achieved and, for an adjusted difference (marginal effect) of 1.3 sessions per day (p < 0.001) (Table 3). The mean daily pumping frequency was 5.6 sessions per day (95% CI: 5.0–6.2) on days mothers achieved CTV, which was 0.7 sessions more than for days that CTV was not achieved (p = 0.050). The mean daily pumping minutes was 108 (95% CI: 99–117) on days SA was achieved versus 83 (95% CI: 75–92) on days SA was not achieved, for an adjusted difference of 25 minutes per day (p < 0.001). No significant difference for achieving versus not achieving CTV was noted for daily pumping minutes. The adjusted difference in daily pumped MOM volume for postpartum days 2–14 was 131 mL higher on days SA was achieved versus not achieved (p < 0.001) and 354 mL higher if CTV was achieved versus not achieved. Additionally, the adjusted difference in daily pumped MOM volume was 331 mL for achieving CTV (p < 0.001), conditional on achieving SA (results not shown).
Adjusted Results for Daily Pumping Behaviors, Daily Pumped Mother’s Own Milk Volume, and Total Opportunity Cost
Generalized linear regression model (GLM) constructed with a Poisson distribution and power 1.23 link function; model adjusts for SA, CTV, day of life squared, Black race, maternal age, and cesarean delivery.
GLM constructed with a gamma distribution and power −1.4 link function; model adjusts for SA, CTV, day of life squared, Black race, maternal age, gestational age at birth, and preeclampsia.
GLM model is fit with a Poisson distribution and power 0.03 link function; model adjusts for SA, CTV, SA × CTV interaction term, day of life squared, BMI (≥27), previous breastfeeding experience, and cesarean delivery.
Generalized linear regression model (GLM) constructed with a Poisson distribution and identity link function; model adjusts for Black race, maternal age, breastfeeding experience, and number of days with pumping data.
GLM model constructed with a Poisson distribution and power 1.34 link function.
Limited to subjects that achieved secretory activation (N = 62); four additional observations were excluded due to missing sodium data after achieving secretory activation.
CTV, coming to volume; MOM, mother’s own milk; SA, secretory activation.
The total opportunity cost over postpartum days 2–14 was $376 if SA was achieved compared to $221 if SA was not achieved, for a mean difference of $155 (95% CI: 24, 285, p = 0.020) (Table 3). For mothers who achieved SA, the opportunity cost did not differ between mothers who achieved versus did not achieve CTV ($389 for both groups, p = 0.997). The opportunity cost of maintaining SA, conditional on achieving SA, was $441 compared to $346 if SA was not maintained, for a marginal effect of $94 (95% CI: 21, 168, p = 0.011).
Discussion
These results add an important economic perspective to the growing body of research addressing early unplanned cessation of lactation in breast pump-dependent mothers of preterm infants hospitalized in the NICU. To the best of our knowledge, this is the first study to describe how daily pumping behaviors and pumped MOM volume relate to achieving SA, achieving CTV, and maintaining SA, as well as how these outcomes translate into maternal opportunity costs. Overall, our findings highlight the importance of pumping frequency, minutes, and consistency in SA achievement and maintenance through the first 14 postpartum days. These pumping behaviors involve a time commitment that only the mother incurs and thus reflect the unique burden of maternal opportunity costs in this early postpartum period. These opportunity costs were $376 for achieving and $441 for maintaining SA, translating into an additional $155 for achieving SA and $94 for maintaining SA relative to mothers who did not. Our findings raise several considerations for practice and research.
The additional time spent pumping to achieve and maintain SA may seem small in a 24-hour day, but breast pump-dependent mothers are particularly “time poor” in this early postpartum period compared to healthy mother–infant dyads. These mothers are recovering from an early, often unexpected, complicated delivery and have an average of three comorbidities that necessitate additional rest, activity restriction, medications, and early postpartum follow-up visits. 9 Most mothers are discharged from the hospital prior to achieving SA, so they often must balance frequent pumping with childcare, family needs, household tasks, and traveling to the NICU. All of these competing time demands make it easy to “skip a pumping session” or to be in a venue where pumping is impractical or impossible, such as during lengthy medical follow-up appointments and commutes to and from the NICU. These opportunity costs may be especially burdensome for low-income mothers who lack paid maternity leave, childcare, and household help. 13 Exacerbating this disparity, public insurance and nutrition programs often provide lower-quality breast pumps that remove MOM less thoroughly, quickly, and comfortably, making an already high unpaid workload more onerous.
Although the majority of mothers in this study achieved SA, it was delayed (mean = 5.5 days), and once achieved, it was not maintained for over half of the sample. The normalcy of this fluctuation is unknown because previous studies have typically measured MOM Na concentration only once during the early postpartum period in healthy and at-risk dyads.24–26 Biologically, increases in MOM Na after SA achievement suggest an interrupted transition to the autocrine/paracrine control of lactation,8,10 affecting pumped MOM volume and CTV achievement. Mothers who maintained SA pumped more times and minutes each day between postpartum days 3–14 and had significantly more pumped MOM volume compared to mothers who did not maintain SA. Mothers who maintained SA pumped ≥120 daily minutes consistently over this time period, whereas mothers who did not maintain SA pumped sporadically. Mothers who maintained SA incurred significantly higher opportunity costs than mothers who did not maintain SA ($441 versus $346) due to increased pumping minutes. Since SA maintenance is a prerequisite for achieving CTV and involves significant maternal opportunity costs during a time-poor critical window, it is a priority area for research in this field.
One approach to addressing the maternal opportunity costs and other out-of-pocket costs associated with MOM provision in this population is the use of unconditional and conditional cash transfers made directly to families. Although studies that reimburse maternal opportunity costs for MOM provision or provide an unconditional cash transfer to NICU mothers are underway,27,28 none specifically target this labor-intensive first 14 postpartum days nor include objective measures of SA achievement and maintenance. The upfront costs associated with ensuring that mothers achieve SA and CTV might appear excessive, but they would pale compared to the downstream costs due to the increased risk of potentially modifiable complications of prematurity associated with feedings that are not MOM.3,29 NICUs acquire donor human milk and formula, meaning that these costs are borne by the institution or payers, whereas mothers incur opportunity costs of MOM provision. Future studies on this topic should address these economic realities.
Strengths and limitations
These detailed data represent the largest and most detailed set of pumping behaviors, pumped MOM volume, Na measures, and opportunity costs collected in a NICU with a “best practice” standard of lactation care. However, we acknowledge several limitations. Although we combined similar data from two prospective cohorts of mothers, there were a few differences in collection methods. One cohort used Smart Pumps to automatically collect data for each pumping session, including start and stop times, while the other cohort of mothers manually tracked pumping sessions on paper without recording the start and stop times. We estimated the pumping minutes for that cohort using regression modeling based on maternal and infant characteristics. Additionally, the NICU lactation standard of care for both cohorts controlled for modifiable interventions that otherwise may have affected study outcomes, including breast pump type, breast pump suction patterns, breast shield sizing and placement, and standardized, evidence-based messaging. 30 Thus, our findings may not generalize to NICUs where these practices are not in place.
Conclusions
Pumping frequency is a modifiable behavior that is positively associated with achieving and maintaining SA and achieving CTV but one that represents high maternal opportunity costs. Breast pump-dependent mothers of preterm infants in the NICU spend nearly two hours per day pumping to achieve and maintain SA, which may serve as an economic barrier to MOM provision in the early postpartum period and may contribute to the racial and income disparity in the receipt of MOM at NICU discharge and beyond. Our findings highlight the important gap in maintaining SA once it is achieved and suggest that maternal opportunity costs may play an important role in this critical lactation period. Further study of interventions that offset the maternal opportunity cost of providing MOM in the early postpartum period is needed to address early, unplanned weaning among these vulnerable mothers.
Footnotes
Authors’ Contributions
T.J.: Conceptualization, methodology, formal analysis, writing—original draft, writing—review and editing, and visualization. C.M.P.: Data curation and writing—review and editing. P.P.M.: Conceptualization, methodology, data curation, writing—original draft, and writing—review and editing. L.A.P.: Conceptualization, methodology, and writing—review and editing. R.H.: Conceptualization, methodology, data curation, and writing—review and editing.
Disclosure Statement
T.J.: Consultation agreement with Medela, AG. C.M.P.: None. P.P.M.: Consultation agreement with Medela, AG. L.A.P.: Consultation agreement with Medela, AG; research funds, Medela AG. R.H.: Scientific Advisory Board, Medela, AG.
Funding Information
This research was supported by grants from Medela, AG, Family Larsson-Rosenquist Foundation, and Rush University Children’s Hospital Department of Pediatrics.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.