
Abstract
Objective:
Mother’s own milk (MOM) sodium (Na) is an objective measure of secretory activation (SA), which is often delayed or impaired after preterm delivery. We sought to determine in pump-dependent mothers of preterm infants, impacts of maternal comorbidities on lactation outcomes using objective measures, including MOM Na, pumping frequency and MOM volumes for the first 14 postpartum days.
Study Design:
In this secondary analysis of four prospective cohorts, we examined outcomes using logistic and linear regression, survival analysis, and mediation and moderation sub-analyses.
Results:
A total of 143 mothers (57.3% Black, 30.8% Hispanic; 35.0% with hypertensive disorders of pregnancy [HDP]; 9.8% diabetic; 73.8% high body mass index [BMI]) delivered at 29.1 ± 2.8 weeks. Mothers pumped 4.7 ± 1.8 times/daily. Daily pumping frequency was a significant independent predictor of all modeled outcomes (p < 0.001 SA achievement, maintenance, and time to SA achievement; daily MOM volume; coming to volume [CTV; 500 mL/day]). 88.1% achieved SA by MOM Na ≤16 mM at postpartum day 5.6 ± 2.5. Only 41.3% of this subset continuously maintained SA until postpartum day 14. HDP was negatively associated with time to SA (p = 0.039). BMI values were negatively associated with MOM volume (p = 0.017) and CTV achievement (p = 0.02). Effects of daily pumping frequency were moderated by BMI (SA achievement and time to SA) and diabetes (CTV), with worse outcomes for higher BMI or diabetes despite similar pumping frequencies.
Conclusion:
Daily pumping frequency was the significant independent predictor for early lactation outcomes in a breast pump-dependent cohort of mothers of preterm infants. Further research on the interplay between modifiable and unmodifiable lactation risks in high-risk populations is needed.
Introduction
Receipt of mothers’ own milk (MOM) through the entire hospital stay and after discharge from the neonatal intensive care unit (NICU) is a critical best practice to improve health outcomes, lower costs and reduce risks of serious lifetime morbidities in preterm infants.1,2 MOM mitigates the impact of NICU exposures such as inflammation and undernutrition that affect immature organs and biological pathways, setting the stage for potentially preventable morbidities that include necrotizing enterocolitis, late onset sepsis, bronchopulmonary dysplasia and neurodevelopmental problems.1,2 MOM reduces risks of these morbidities and their costs in a dose-dependent manner, with higher amounts of MOM providing the greatest protection.1–3 However, high-dose MOM through to and beyond NICU discharge depends upon the mother’s ability to initiate and maintain lactation while breast pump-dependent, meaning that the breast pump rather than the infant regulates MOM removal and lactation processes.4,5 Four decades of research with this vulnerable population has highlighted both the modifiable and unmodifiable risks associated with provision of sufficient volumes of MOM through to and after NICU discharge.6–9
Topping the list of unmodifiable risks is the shortened duration of pregnancy-induced breast development (e.g., secretory differentiation) as well as specific comorbidities of pregnancy that are more likely to occur in this at-risk population. 6 These comorbidities, including overweight and obesity, diabetes and pre-eclampsia/pregnancy-induced hypertension (hypertensive disorders of pregnancy [HDP]), have been independently associated with suboptimal lactation outcomes in mothers of term and preterm infants.6,10–13 Similarly, medical management of these complications including medications, prolonged bedrest, and cesarean delivery, may further exacerbate lactation risk.12–14 These maternal comorbidities likely affect the achievement of secretory activation (SA; lactogenesis II; milk coming in) and coming to volume (CTV; pumping ≥500 mL/day of MOM) by postpartum day 14, both which predict receipt of MOM at NICU discharge.15–20 In previous research by our team, SA achievement, as measured objectively using MOM sodium [Na] concentration ≤16 mM, was significantly delayed (mean = 5.8 days) in a cohort of 29 breast pump-dependent mothers of preterm infants.6,10 Furthermore, of the mothers who achieved SA, only half maintained daily Na ≤16 mM consistently through 14 days postpartum and fewer than half achieved CTV.10,16 However, neither this cohort nor those in previously published studies has enrolled a sufficient sample to examine the impact of separate and combined maternal comorbidities on achievements of SA and CTV.
Therefore, the purpose of this study was to leverage prospectively-collected data from four cohorts in two institutions to study the impact of common maternal comorbidities (HDP, diabetes, high BMI) on lactation outcomes in pump-dependent mothers of preterm infants using objective measures of SA and pumped MOM volume. We also sought to examine the interplay between these unmodifiable maternal risks and maternal pumping behaviors. Although breast pump-dependency itself is unmodifiable, specific pumping behaviors such as daily pumping frequency can be modified if shown to have a moderating or mediating effect on achievement of SA and CTV.
Materials and Methods
Design
This secondary analysis of prospectively collected data merged datasets from two prospective non-randomized, observational studies (Illinois cohorts10,16) and 2 randomized controlled trials (Florida cohorts; 1 currently unpublished 21 ) All cohorts included detailed descriptions of maternal comorbidities and daily measurement of pumping frequency, pumped MOM volume and MOM biomarker(s) of SA between days 1 and 14 postpartum. For the two randomized cohorts, maternal co-morbidities were not a part of the randomized interventions and were recorded only as background data.
Sample
Mothers were recruited for the original studies from two medical center NICUs with high levels of NICU-specific proactive lactation care, including evidence-based lactation messaging from physicians, nurses, lactation consultants and/or breastfeeding peer counselors, hospital grade pump availability, pumping within 6 hours after birth and personalized hands-instruction during the first 2 postpartum weeks. By protocol, mothers for the prospective studies were approached either antenatally or in the first 24 hours postpartum, but informed consent was obtained only after delivery. Inclusion criteria have been previously published and were delivery at gestation <33 or <34 weeks (varied by cohort), English or Spanish speaking, decision to initiate lactation, and a presumably viable infant.10,16,21 The original studies were approved by the Institutional Review Boards of Rush University Medical Center (Chicago, IL, USA; 2 cohorts) and University of Florida (Gainesville, FL, USA; 2 cohorts) and written informed consent was obtained for mothers and their infants. For this study, IRB approval was obtained for secondary analysis of de-identified data, and data use agreements were in place between the institutions.
Measures
The following measures were collected from all cohorts: maternal and infant characteristics including maternal co-morbidities and daily pumping behaviors (measures of pumping frequency, pumped MOM volume) and daily MOM Na concentration.
Maternal and infant characteristics
For the original studies, maternal characteristics were collected from electronic medical records (EMR) and included age, parity and health conditions thought to affect lactation outcomes, including HDP, diabetes, and mode of delivery. Pre-pregnancy weight and height to calculate body mass index (BMI; kg/m2) and previous breastfeeding experience were acquired by subject questionnaire. In our analyses, BMI was used as both a continuous and as a dichotomous (normal [BMI 18.5–24.9 kg/m2] versus abnormal [BMI <18.5 or ≥ 25kg/m2]) variable. Infant characteristics were collected from the EMR and included sex, birth weight, and gestational age at delivery.
Pumping frequency
In three cohorts, mothers maintained pumping logs to record the start and end times for each pumping session. 22 For the second Illinois cohort, a Smart pump was used (Medela AG Switzerland) in which pumping frequency and durations were recorded and stored electronically. 10 Daily and cumulative pumping frequencies were determined by summing the number of individual daily pumping sessions in a 24- hour period (00:00–23:59). For incomplete pumping logs, the study staff used weighed MOM containers to fill in incomplete self-reported records. If no pumping log, weighed MOM, Smart pump data, or test weighing data were available for that day, it was assumed that no pumping had occurred.
Pumped MOM volume and achievement of CTV
All pumped MOM for the four cohorts was weighed (nearest 0.1 g) on a scientific scale (Tanita, Japan). Pumped MOM volume was calculated by subtracting the pre-filled from the filled MOM container weight (g) and converting 1 g weight = 1 mL volume. 23 For three cohorts, MOM weights were performed by the study team. For one Illinois cohort, MOM weights were by mothers using the same scientific scale but integrated into the data logger for the Smart pump. 10 Achievement of CTV was calculated as a dichotomous variable (yes/no) based on any day with pumped MOM volume ≥500mL between postpartum days 1 and 14.
Achievement of SA and maintenance of MOM Na ≤16 mM
All four cohorts collected daily (or twice daily) MOM samples for measurement of MOM biomarkers. Although different cohorts collected slightly different amounts of MOM (0.4–1.8 mL) and some measured additional biomarkers, all measured daily Na concentration, which has been the most highly predictive biomarker of SA achievement in previous studies.6,16,24 Identical freezing, thawing and measurement techniques were used in all cohorts, consistent with methodology papers on this topic. 25 In brief, after daily collection, MOM samples were labeled and stored at −20°C until analyzed in duplicate by ion electrode sensors (Horiba, Japan) either locally10,21 or after shipping to the University of Western Australia human milk laboratory. 16 Sodium concentration was measured in parts per million, then divided by its molecular weight (22.9 g/mMol). Sample collection occurred only when MOM was sufficient and not needed to meet infant feeding requirements.
For this analysis, we measured the proportion of the sample that achieved SA (defined as MOM Na ≤16 mM) as well as the postpartum day when SA was first achieved. We also measured the proportion of the sample for whom MOM Na ≤16 mM was maintained consistently (yes/no) from the time of first SA achievement through to postpartum day 14.
Data analysis
For each of the outcomes, we conducted direct comparisons of lactation outcomes between groups classified on the basis of individual comorbidities (HDP, diabetes, BMI abnormality) with Chi-square tests or t-tests. Multivariable regression models that included covariates such as demographics, delivery mode, previous breastfeeding/pumping experience and daily pumping session frequency, were constructed to examine the effect of comorbidities on outcomes. We used survival analysis to examine time to achieve SA. BMI was classified as normal versus abnormal in direct comparison and was used as a continuous variable in regression models.
Results
Of 149 subjects from the combined cohorts, 6 were removed for incomplete maternal comorbidity data, leaving 143 mothers for analysis. Characteristics of the sample are summarized in Table 1. A majority of subjects in this racially and ethnically diverse cohort were overweight/obese, delivered via cesarean, and did not have prior breastfeeding/pumping experience. Mothers pumped a mean of 4.7 ± 1.8 times/daily. In direct comparisons, mothers with HDP pumped less frequently (4.0 times daily) versus those without (5.0 times daily, Table 2). Average daily pumping frequency played an important role in all outcomes, so further analyses were conducted to examine potential relationships between this modifiable variable and unmodifiable maternal comorbidities. Specifically, we investigated moderation and mediation effects between daily pumping frequency and outcome variables for each comorbidity singly and in combination. Moderation means that a comorbidity affected the relationship between pumping frequency and outcomes, whereas mediation means that pumping frequency affected the relationship between the comorbidity and outcomes. Significant findings are presented below, with additional data summarized in Table 3.
Characteristics of the Sample
BMI, body mass index; SD, standard deviation.
Direct Comparisons of Lactation Outcomes by Maternal Risk Factor
Maintenance of SA only in those who ever achieved SA (n = 126).
BMI, body mass index (normal 18.5–24.9 kg/m2); CTV, coming to volume (pumped ≥500 mL/day); HDP, Hypertensive disorder of pregnancy; MOM, mother’s own milk; SA, secretory activation.
Additional Analyses
Limited to those who achieved SA (n = 126).
CTV, coming to volume; HDP, Hypertensive disorder of pregnancy; MOM, mother’s own milk; SA, secretory activation.
Daily MOM volume
Mean daily pumped MOM volume was 296.1 ± 263.2 mL. Mothers with an abnormal BMI had lower daily pumped MOM volume (269.7 mL) than normal BMI mothers (383.6 mL; p = 0.03, Table 2). In a linear regression model, mean daily pumping frequency was a positive predictor (p < 0.001) and BMI value a negative predictor (p = 0.02) of daily pumped MOM volume. There was no evidence of moderation or mediation in the relationship between average daily pumping frequency and daily pumped MOM volume.
Achievement of SA
Of the 143 mothers, 126 (88.1%) achieved SA. In direct comparisons, mothers with HDP were less likely to achieve SA than those without (80.0% versus 92.5%, p = 0.028, Table 2). No differences in the achievement of SA were noted for either diabetes or BMI category. Only daily pumping frequency was a significant predictor (p < 0.001) of SA achievement in logistic regression models that included the three comorbidities as well as delivery mode, previous breastfeeding, race, ethnicity, and daily pumping frequency. BMI as a continuous variable significantly moderated the effect of daily pumping frequency on SA achievement (p = 0.04), with abnormal (higher) BMI mothers less likely to achieve SA despite pumping as frequently as lower BMI mothers. Pumping frequency did not mediate effects between individual or combination of comorbidities on SA achievement.
Time to first achievement of SA
Mothers achieved SA for the first time at mean (SD) postpartum day of 5.6 ± 2.5. Mothers with HDP achieved SA later (7.9 ± 3.9 days) versus those without (5.8 ± 3.2 days, p < 0.001, Table 2.) No differences in first achievement of SA were seen for diabetes or BMI category. In a survival analysis of mothers who achieved SA that included the three comorbidities as well as delivery mode, previous breastfeeding/pumping experience, race, ethnicity, and daily pumping frequency, daily pumping frequency was a significant positive predictor (hazard ratio 1.35 [95% CI 1.21, 1.52]; p < 0.001) and HDP was a significant negative predictor (hazard ratio 0.64 [0.42, 0.98]; p = 0.04) of days to first achievement of SA. Only BMI category moderated the effect of mean daily pumping frequency on the first achievement of SA (p = 0.03), with high BMI mothers taking longer to first achieve SA despite comparable pumping. HDP directly affected the first achievement of SA (95% CI −0.06, 3.63), but daily pumping frequency mediated 33% of the effect attributed to HDP, meaning that less frequent pumping among mothers with HDP explained 33% of the variance in the statistical model (Fig. 1). However, this mediation effect was not statistically significant (95% CI −0.0318 to 1.68). Other moderation and mediation models did not show or approach significance with respect to first achievement of SA.
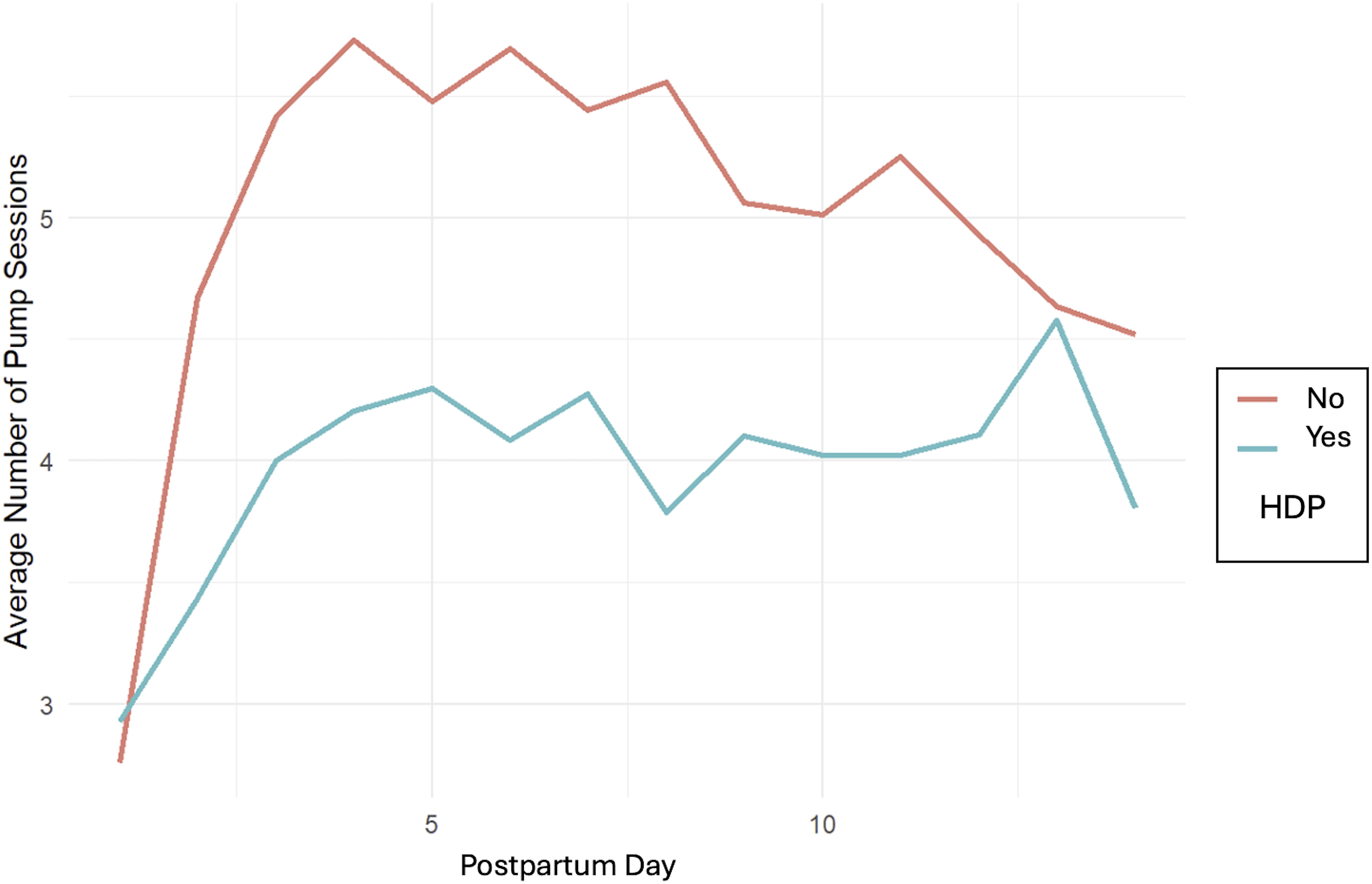
Daily pumping frequency in mothers with and without hypertensive disorders of pregnancy (HDP).
Maintenance of Na ≤16 mM after initial SA achievement
For the 126 (88.1%) mothers who achieved SA, 52/126 (41.3%) of mothers continuously maintained Na ≤16 mM through to postpartum day 14. No differences were seen in direct comparisons with HDP, diabetes or BMI categories (Table 2.) In a binomial regression model with days of Na ≤16 mM as the outcome variable and the three comorbidities, delivery mode, previous breastfeeding/pumping, race, ethnicity, and daily pumping frequency as covariates, daily pumping frequency was again significant (p < 0.001). There was no evidence that any comorbidity moderated or mediated the relationship between daily pumping frequency and SA maintenance.
Achievement of CTV
Of the 143 mothers, 63 (44.1%) achieved CTV. A logistic regression model revealed that mean daily pumping frequency was a positive (p < 0.001) and BMI value was a negative predictor (p = 0.02) of CTV achievement. Only diabetes moderated the relationship between average daily pumping frequency and CTV achievement (p = 0.03), with the positive effect of pumping sessions on CTV weaker for mothers with diabetes. The relationship between comorbidities and achievement of CTV was not mediated by pumping frequency.
Single versus multiple co-morbidities
All aforementioned models were also performed using combinations of morbidities (two or three) instead of the individual morbidities of HDP, diabetes, and BMI abnormality. None were significant, so further details of these analyses are not included.
Discussion
To our knowledge, this detailed analysis of the relationship between maternal comorbidities of pregnancy and early lactation outcomes in breast pump-dependent mothers of preterm infants is the first to combine a large sample size and objective measures for outcome variables. Overall, our findings reveal that pumping frequency was a primary direct predictor of all lactation outcomes, consistent with recent studies of breast pump-dependent mothers of preterm infants.6,10,17 However, we also found that maternal comorbidities affected these relationships via moderation and mediation effects. HDP directly affected SA achievement, but this relationship was partially mediated by pumping behaviors, because affected mothers pumped less frequently. Maternal BMI and diabetes, both unmodifiable risks at the time of birth, separately moderated relationships between pumping frequency and achievements of SA and CTV, respectively. Specifically, mothers with these morbidities had similar pumping frequencies as unaffected mothers, but did not achieve the same lactation outcomes. These novel findings have implications for clinical practice and highlight research gaps.
Although the vast majority of mothers in this combined cohort achieved SA, they took nearly twice as long as healthy breastfeeding mothers with term infants. 18 This finding is consistent with prior reports of delayed SA in breast pump-dependent mothers of preterm infants.16,24 Most previous studies of SA achievement in both healthy and at-risk dyads have used maternal perceptions of milk coming in rather than MOM biomarkers to measure SA achievement. 24 Our research with breast pump-dependent mothers of NICU infants has shown a lack of correlation between maternal perceptions and MOM Na concentration, highlighting the limitations of this subjective measure. 24 Therefore, differences in populations and methodologies should be carefully considered when comparing these findings to other studies.
After achieving SA, only a minority of mothers in our cohort continuously maintained daily MOM Na ≤16 mM during the 14-day study. This finding indicates a reopening of paracellular pathways in the mammary gland, usually associated with mastitis and involution.17,26,27 However, we speculate that re-elevation of MOM Na between achievements of SA and CTV signals a potential problem in the transition to autocrine/paracrine control of lactation, which is primarily regulated by effective and frequent MOM removal. 5 Numerous modifiable factors have been associated with ineffective MOM removal and should be addressed both for practice and research. These include assuring that MOM is being removed effectively from both breasts by optimizing pumping frequency, breast pump suction pattern and pressure, breast shield fit and duration of each pumping. 4 If not detected or mitigated, this early reopening of paracellular pathways may be the first step toward early, unplanned cessation of lactation in these pump-dependent mothers.
Of the three morbidities, only HDP was associated with a lower rate of SA achievement in direct comparisons and a longer time to achieve SA in the survival model. HDP are acute inflammatory complications that potentially affect lactation through multiple mechanisms as well as through side effects from therapies. In a recent study of 255 mothers with pre-eclampsia who delivered preterm, the majority had a cesarean delivery, post-operative pain, magnesium therapy, and sedation-inducing opiate treatment. 28 Although mothers in our study with HDP took longer to achieve SA, it had no significant effect on CTV achievement. One possible explanation is that although affected mothers started with fewer daily pumping sessions, by postpartum day 14 they were pumping as frequently as unaffected mothers (Fig. 1). Infrequent early pumping among these women is modifiable, and policies to ensure that providers or family members assist with pumping in the early postpartum days should be implemented.
Relatively few mothers (9.8%) in our study were diagnosed with diabetes, despite the majority being overweight or obese. Maternal diabetes was not associated with SA achievement or timing, nor pumped MOM volume, but did moderate the effect of pumping frequency on CTV achievement. In other words, comparable pumping frequency did not translate into CTV achievement for diabetic mothers at the same rates as for non-diabetic mothers. Previous studies have reported delayed SA and/or low MOM volume in mothers with both gestational and pre-pregnancy type II diabetes, albeit with different methodologies for SA measurement and excluding breast pump-dependent mothers of preterm infants.19,29,30 Our findings were remarkably similar to those of Arthur et al and Chertok et al, who reported significantly different MOM lactose and citrate concentrations over the first postpartum week in mothers of term infants with and without insulin-dependent and gestational diabetes.30,31 Whereas our findings measured only paracellular pathway closure, these researchers found disruptions in both transcellular (citrate, lactose) and paracellular pathway (lactose) mechanisms. Both gestational and pre-pregnancy type II diabetes are characterized by insulin resistance, which appears to be essential for secretory differentiation during pregnancy. Insulin-sensitive genes are upregulated during lactation, and insulin facilitates substrate availability for MOM synthesis. 32 Higher MOM insulin concentration has been associated with lower rates of exclusive MOM in a term population, presumably due to low MOM volume. 33
Our findings indicate that overweight/obesity negatively affected several lactation outcomes both directly and via moderation, consistent with previous human and animal studies and a Cochrane review linking high BMI to lactation risks in healthy and at-risk mothers.34,35 However, our study is among the few that examined lactation outcomes in the first 14 postpartum days and included only breast pump-dependent mothers of preterm infants. Biological mechanisms that may explain these findings include a blunted prolactin response, retained progesterone in adipose tissues, subclinical inflammatory state of the mammary gland, and elevated leptin and insulin concentrations associated with chronic inflammation and insulin resistance.27,33,36–39
While biological mechanisms almost certainly impact early lactation outcomes in overweight/obese mothers who are breast pump-dependent following preterm birth, clinical practices that optimize mammary gland stimulation and MOM removal are typically lacking. Mothers with overweight/obesity often cannot visualize correct placement of the breast shield, may not have access to customized breast shield sizing, and may experience body image concerns while using the breast pump in the NICU setting. It is unknown whether adherence to a more frequent pumping schedule would be beneficial, or whether different breast pump suction patterns—especially those that maximize duration of suction per cycle—might be more effective in extracting available MOM from larger breasts.
Our analyses did not reveal statistically significant differences with combinations of comorbidities, likely due to the small sample size and low incidence of diabetes. It is also possible that the strong effect of pumping frequency overshadowed the contribution of combined comorbidities. More recent studies have conceptualized obesity within a constellation of metabolic risk factors associated with insulin resistance and chronic inflammation. In particular, the pro-inflammatory signaling molecule tumor necrosis factor α (TNF-α) is known to suppress expression of certain proteins required for milk synthesis, such as glucose transporters and lipoprotein lipase.40,41 Therefore, chronic inflammation may be a physiological explanation for the reduced effectiveness of pumping in mothers with insulin resistance and obesity. The addition of metabolic measures in future research is imperative to thoroughly understand underlying mechanisms associated with maternal comorbidities.
Study strengths include the relatively large and racially, economically and geographically diverse sample of breast pump-dependent mothers of preterm infants from hospitals with optimized NICU-specific lactation care. Our objective daily measurement of MOM Na in this vulnerable cohort is also a study strength that allowed detection of reversal of threshold Na concentrations after achievement of SA. Limitations include a relatively small number of diabetic mothers despite a high prevalence of overweight/obesity. This study focused on objective MOM biomarkers and physiological risk factors, so we did not include nor control for maternal lactation goals. For example, it is possible that goals for partial versus exclusive MOM may have varied among mothers with different comorbidities in a way that influenced pumping behaviors. Finally, our data must be interpreted with the knowledge that in addition to comorbidities, mothers had a shorter duration of secretory differentiation, so generalization to mothers of term infants may be inappropriate.
In conclusion, in a relatively large, diverse cohort of pump-dependent mothers with significant medical comorbidities who delivered very preterm infants, the vast majority achieved SA by objective MOM biomarkers, albeit taking on average twice as long as healthy term breastfeeding mothers. However, most mothers had episodes of Na >16 mM after achieving SA, indicating a reopening of paracellular pathways, and only a minority went on to achieve CTV by postpartum day 14, a milestone that facilitates long-term exclusive MOM feeding. 15 We found that daily pumping frequency, although suboptimal in the cohort overall, was similar to the frequences reported in other preterm cohorts. 42 Importantly, pumping frequency was predictive of all lactation outcomes, suggesting a need to focus on increased early pumping frequency in the NICU population, especially in mothers with HDP who were more likely to pump less in the immediate post-partum period. Finally, mothers with high BMI and diabetes appeared to have biological risks that moderated the effect of pumping, with lower MOM volumes or rates of CTV than healthier mothers despite similar pumping frequencies. Further research is urgently needed to determine whether optimized pumping frequency or other targeted interventions can overcome physiological “pumping resistance” in this high-risk population.
Footnotes
Authors’ Contributions
All the authors made substantial contributions to the study design, analysis, and interpretation of data, and drafting and revising the article. All approve the final version to be published.
Ethics/Consent Statement
Written consent was obtained from all subjects for participation in the original cohort studies.
Disclosure Statement
R.H. serves on the clinical advisory board for Medela Americas and receives honoraria for occasional webinars. P.M.M. has a consultant agreement with Medela AG. L.A.P. is a consultant and speaker for Medela, and serves as a consultant for Otsuka Pharmaceutical Factory. No products are discussed in this article. The other authors state that they do not have any disclosures.
Funding Information
For the original cohorts, research was supported by grants from Rush University Children’s Hospital Department of Pediatrics (R.H.), Family Larsson-Rosenquist Foundation (Trainee Travel Award to C.M.P.), the University of Florida, and an unrestricted grant from Medela AG, Switzerland for research coordinator salary. T.G.M. is supported by the NICHD (1K99HD113880-01A1).