
Abstract
Background:
Interchangeable terminology and definitions of breastfeeding difficulties may inadvertently influence premature cessation of breastfeeding. Lactation failure is a distinct concept from breastfeeding cessation, and it is vital to differentiate between them, especially in educating health care professionals in communicating and supporting mothers perinatally.
Purpose:
Comprehensively review varying terminology and definitions, providing a more nuanced understanding of lactation failure versus breastfeeding cessation, and highlighting physiological and social, emotional, mental, and commercial factors that influence breastfeeding outcomes.
Method:
A scoping review of published literature from medical and scientific databases such as MEDLINE (via PubMed), Scopus, and Web of Science from 2000 to 2023.
Results:
N = 476 publications were collected during the identification phase; N = 49 from 28 countries around the world met the inclusion criteria and were used in the review. Only N = 13 studies ventured definitions for the terms used. Factors affecting breastfeeding were categorized as physiological leading to lactation failure and distinguished from social, mental, emotional, or commercial factors leading to breastfeeding cessation.
Recommendations and Conclusions:
Understanding the complexity of the factors underlying lactation failure and breastfeeding cessation can be improved by delineating the terminology and definitions variations used to communicate, provide awareness, education, design and delivery of interventions and support for initiation, and continuation of breastfeeding. Further in-depth research and analysis of the complex issues and factors influencing breastfeeding practices is required.
Background
The successful initiation and continuation of breastfeeding are pivotal for maternal and infant health, yet declining rates of breastfeeding globally are a cause for concern.1–3 Global health organizations such as the World Health Organization and United Nations Children's Fund advocate that breastfeeding be initiated within the first hour after birth and that infants continue to be exclusively breastfed for the first 6 months of life.2,4,5 These recommendations specify that no other foods or liquids are required to supplement breast milk, including water. However, the act of breastfeeding, a natural and essential aspect of infant health, nutrition, and development, can often be fraught with challenges that lead to early cessation, often inaccurately termed as “breastfeeding failure.” The literature reveals a wide array of interchangeable and overlapping terminology related to breastfeeding struggles that may inadvertently influence premature cessation of breastfeeding.
Many mothers do not initiate or cease to breastfeed, resorting to artificial feeding early on due to common misconceptions around breast milk production, supply, and their ability to do so or due to lack of education and support.1,2,6 Despite the overlap, lactation failure is a distinct concept from breastfeeding cessation, and it is vital to differentiate between the two, especially in educating health care professionals and communicating and supporting mothers perinatally. Outlining the factors underpinning lactation failure and breastfeeding cessation is vital to improving maternal and infant health outcomes, supporting breastfeeding interventions, and reducing the likelihood of early breastfeeding cessation.
Understanding the complex interplay of factors that influence lactation and breastfeeding outcomes is essential. This scoping review explores the various terminology and definitions of diverse factors contributing to lactation failure and breastfeeding cessation, differentiating between physiological, mental, emotional, social or cultural, and commercial aspects. Through this comprehensive review, we seek to inform health care practitioners, policymakers, breastfeeding advocates, and mothers considering or venturing into breastfeeding experiences while highlighting the importance of addressing the multifaceted nature of lactation and breastfeeding issues, and the ramifications they pose for maternal well-being and infant health.
Lactation is nature’s biological gift to mother and baby.4,6,7 The provision of sustenance via this dyadic relationship is essential to support optimal infant growth and development, and greatly influences maternal health and well-being.3,5–7 Lactation failure is not clearly defined in the literature and has been given several descriptions justifying the need to introduce artificial or supplemental feeds within hours or days after birth, because of total absence of, or insufficient milk production or minimal milk secretion from the mammary glands in the breast in sufficient quantities to meet the nutritional needs of the infant following 7 days of feeding, such as: (a) failure of breast tissue to produce a minimum of breast milk, (b) infant’s failure to thrive and sustain growth within 2 standard deviations of the norm, and (c) mother’s inability to reach personal goals for the duration of lactation.7–10 The term “lactation failure” encompasses various physiological aspects ultimately impacting milk production. These terms, used interchangeably, include lactation dysfunction, lactation insufficiency, insufficient milk syndrome, agalactia, hypogalactea, hypoplasia, and inadequate glandular tissue.7–12
Five percent of mothers (or 1 in 20) may have a primary inability to lactate, caused by inadequate glandular tissue resulting from conditions like hypoplastic breasts, as well as surgical procedures of the breast such as mastectomy, breast reduction or augmentation, cyst removal, or nipple piercing, which can lead to disruption of the intricate ductal and neurological pathways essential for successful lactation.7,11,12 Eighty percent of mothers may have a secondary inability to lactate caused by medical conditions such as anemia, hemorrhage, hypertension, retained placenta, or other hormonal or glandular disorders, such as Sheehan’s syndrome.7–12
Actual physiological lactation failure, although considerably rare, affects the nutritional well-being of the infant, leading to growth faltering and increased vulnerability to health issues, and has consequences for maternal health and well-being; however, the misconceptions surrounding the prevalence of these conditions lead to mothers often being misdiagnosed, mislabeled, and misguided, with perceptions of breast milk insufficiency, feelings of being under pressure, of inadequacy, guilt, and stress, ultimately influencing their mental and emotional health and the decision to discontinue or cease breastfeeding unnecessarily.13–16 It is crucial to distinguish from other social, environmental, cultural, or commercial factors that may be playing a major role in the circumstances surrounding the early postpartum period and breastfeeding.
Importance and value of this research study
The study highlights the necessity of raising awareness among health care practitioners and the public of the varying terminology and complex factors associated with lactation failure and breastfeeding cessation and the modifiable influences. It underscores the significance of prioritizing attention and care for mothers vulnerable to early cessation due to various challenges. Given the enduring impact of early infant breastfeeding behaviors on long-term health and well-being for both mother and baby, it emphasizes the urgency of high-quality research on lactation failure and breastfeeding cessation. This scoping review offers a comprehensive overview of research on these multifaceted issues, serving as a resource for policymakers, practitioners, and advocates seeking to promote breastfeeding for maternal and infant health through informed interventions.
Aim and Objective
In this scoping review, our aim was to comprehensively review the varying terminology and definitions used to map out and explore these multifaceted dimensions, providing a more nuanced understanding of lactation failure versus breastfeeding cessation, highlighting the physiological and social, emotional, mental, and commercial factors that influence these outcomes.
Specifically, our objective was to define and differentiate lactation failure from breastfeeding cessation to highlight how lactation failure pertains to the rare, predominantly physiological inability of the mammary glands to produce an adequate quantity of milk, while the multifaceted, more common, and often social nature of breastfeeding cessation encompasses a spectrum of challenges; physiological, mental, sociocultural, and commercial factors. This differentiation will help dispel misconceptions and promote a more nuanced understanding of the breastfeeding landscape. To achieve this objective, this scoping literature review followed specified guidelines, 17 and intends to contribute to the body of knowledge surrounding lactation failure and differentiate it from breastfeeding cessation, ultimately promoting a more informed and precise discourse on this critical issue in maternal and infant health.
Materials and Methods
Search strategy
We searched MEDLINE (via PubMed), Scopus, and Web of Science databases from their inception to March 2023. We devised a comprehensive search strategy employing specific terms and relevant keywords about breastfeeding cessation, lactation insufficiency, lactation failure, and breastfeeding problems, reasons, and causes (Table 1).
Keywords and Search Terms
Screening and study selection
In conducting our search, we adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 18 The search was conducted in January–March 2023. Two review authors (M.B.) and (H.Z.) screened and retrieved titles and abstracts independently to determine initial eligibility and develop a categorized list for further review using predefined inclusion/exclusion criteria. The reviewers established four categories for factors related to lactation failure or breastfeeding cessation: physiological factors, mental and emotional factors, social and environmental factors, and commercial factors (Fig. 1). Comparisons of selected publications were discussed to agree on the list for full-text retrieval and final inclusion in the review. Bibliographies of selected publications were also reviewed.
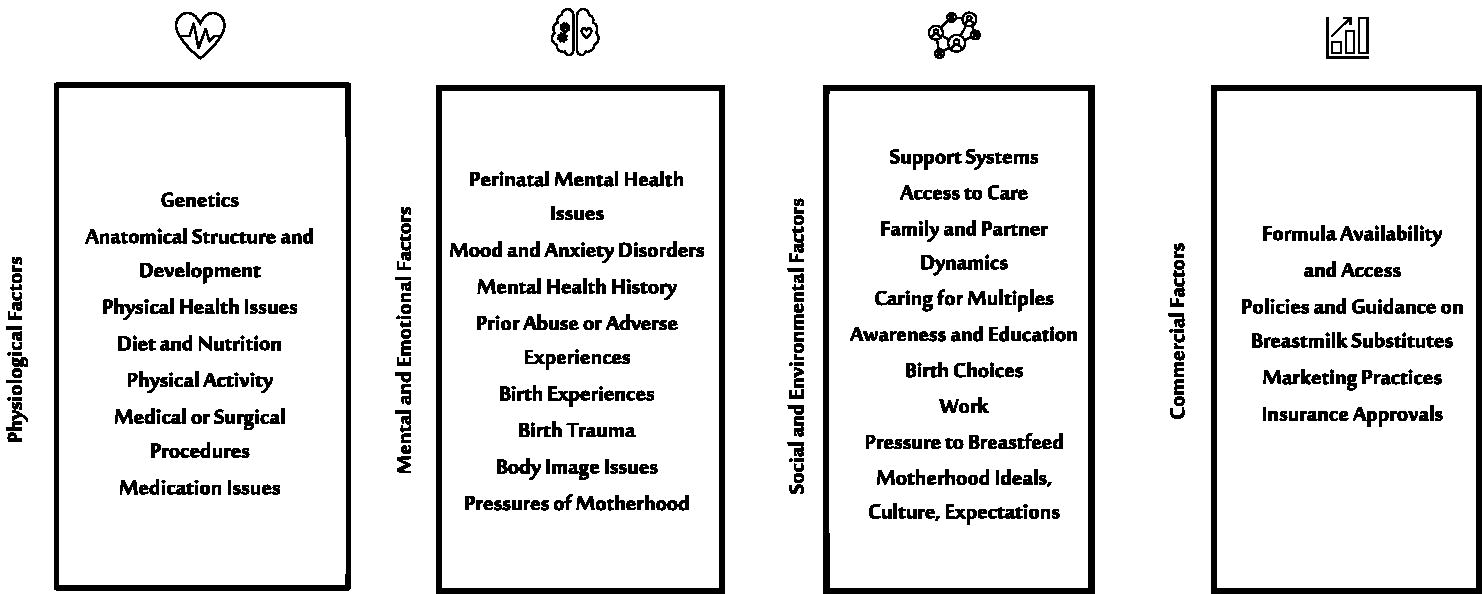
Factors related to lactation failure and breastfeeding cessation.
Eligibility criteria
The review included both primary studies and secondary investigations published in English. For primary studies, retrospective and prospective designs were acceptable, encompassing cohort, case–control, and cross-sectional investigations. We also included randomized trials. For literature reviews, we considered both narrative and systematic reviews. Studies published between January 2002 and March 2023 were considered for analysis to ensure the inclusion of contemporary terminology. Studies were excluded if they were unrelated to the issues of interest in this review and did not discuss aspects of breastfeeding cessation, lactation failure, lactation insufficiency, breastfeeding problems, difficulties, or stopping breastfeeding in women. We excluded studies discussing lactation in animals. We also limited our search to as far back as 2002 and excluded any studies published before that. We excluded lab-based or cellular-level research and studies not published in the English language. We also excluded research on the technical details of pumping devices and apparatus and related production amounts that did not specifically discuss the aspects concerning the difficulties or challenges relevant to breastfeeding mothers.
Data extraction and synthesis
Data from shortlisted studies was extracted from the full text using a developed Microsoft Excel template, which was used to support the synthesis of findings and write-up of the review, using a narrative approach due to the heterogeneity of the findings. Data extracted from each study included the study’s authors, year of publication, study design and measures, country, sample size, method, key findings, limitations, and recommendations were extracted (see Supplementary Table S1). Data extraction was performed by the two reviewers independently, with discussions to reach a consensus in case of inconsistencies. Findings were used to describe the issues relating to the aim and objective of this study, delineating, and analyzing the terminology, definitions, and factors associated with lactation failure and breastfeeding cessation, and supporting detailed discussion, development, and write-up of practical recommendations.
Results
Figure 2 summarizes the study selection process. In the identification process, n = 476 studies were retrieved. After eliminating duplicate records and irrelevant topics and abstracts, n = 238 studies were retained for screening. After initial screening, n = 169 studies were excluded. N = 69 studies met the eligibility criteria. Upon further assessment, n = 20 were excluded as unrelated or irrelevant. Finally, n = 49 studies were included in the review after confirming the inclusion criteria (Fig. 2).
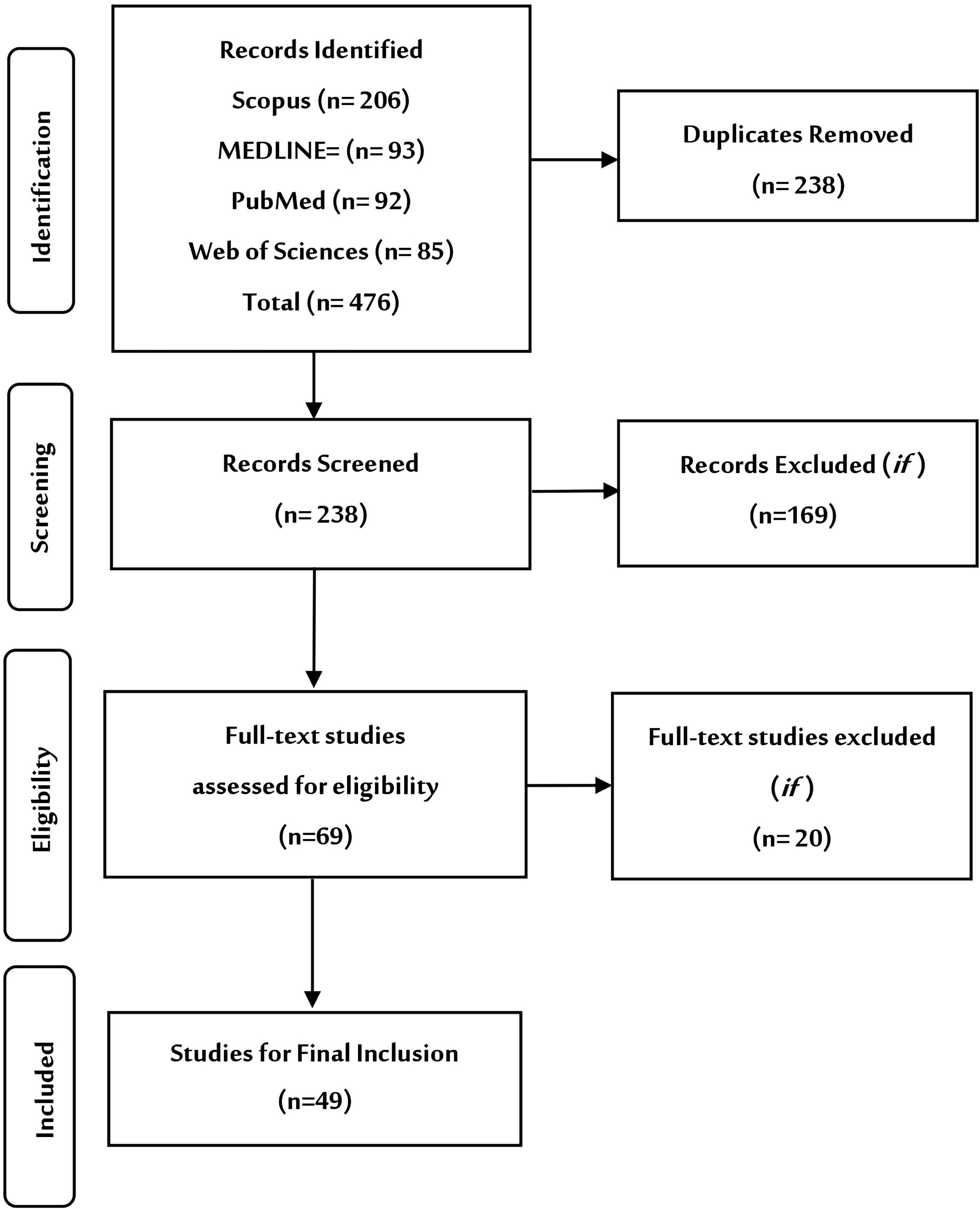
Search strategy and PRISMA flowchart. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
General characteristics of included studies
When reviewing the 49 included studies, we found a wide range of research methods (cohort, prospective, retrospective, qualitative, and cross-sectional) were used, which were assessed for methodological limitations. These investigations originated from 28 countries, with the largest number of contributions from the United States (n = 15), Australia (n = 4), Thailand (n = 2), and China (n = 2). The included studies were from countries all over the world: North America (the United States, Canada, and Mexico), Europe (France, Spain, Italy, the Netherlands, Germany, Poland, Lithuania, and Wales), Africa (Ethiopia, Botswana, and Senegal), the Middle East (Saudi Arabia, the United Arab Emirates, Iran, Kuwait, and Turkey), and Asia (Singapore, Pakistan, Japan, Thailand, Malaysia, India, and Taiwan) and Australia. The studies included in this review emphasize and discuss forms of lactation failure or breastfeeding cessation. The publication dates ranged from 2002 to 2023 (Supplementary Table S1).
Terminology and definitions of lactation failure and breastfeeding cessation
Clear variations were found in the terminology used in the reviewed literature, with studies referring to breastfeeding cessation, discontinuation, termination, weaning, stopping, giving up, ending breastfeeding, failure to breastfeed, lactation failure, lactation difficulties, delayed lactation, decreased human milk production, shortage of milk, and inability to breastfeed. Few studies (n = 13) ventured clear definitions of the terminology used, such as breastfeeding cessation,19–27 breastfeeding discontinuation, 28 breastfeeding termination, 29 insufficient milk supply, 27 and low milk quantity, 30 (Table 2). No definition was found for lactation failure.
Terminology and Definitions of Lactation Failure and Breastfeeding Cessation
Factors relating to lactation failure and breastfeeding cessation
To comprehensively explore the factors contributing to lactation failure or breastfeeding cessation, we categorize the findings into four distinct categories (Table 3).
Factors Relating to Lactation Failure and Breastfeeding Cessation
BMI, body mass index.
Physiological factors
Issues pertaining to physiological aspects that hinder the process of lactation such as mastitis (fever, plugged milk ducts, and breast engorgement), is extensively discussed in the literature as a contributor to lactation failure, interchangeably with cessation of breastfeeding.24,27,30,34,37,54,55,58 Pain and discomfort, attributed to factors such as latching difficulties or nipple issues,19,30,32,37,41,51,58 improper latching,26,33,41 oversupply or extreme fullness of the breast, 58 or inadequate or insufficient milk supply,19,20,29–31,35,40–42,55,57,58 are issues mentioned in the literature, which may make it difficult to sustain breastfeeding. Labor and birth complications, interventions, and type of delivery,21,24,26,28,32,35,37,40 or other maternal or infant physical health issues, such as fetal distress, failure to thrive, maternal incapacitation, or death, are also contributing physiological factors.24–27,29,31,33,35,37,40,50,52,55,58 Maternal body mass index or issues with obesity were mentioned,42,43,49,63 as well as maternal medications or the birth of multiples as contributing to challenges in breastfeeding. 56
Mental and emotional factors
Focuses on the emotional and psychological dimensions as emerging research underscores the role of mental health and emotional issues in breastfeeding challenges, highlighting postnatal depression.23,24,27,32,61,62 The emotional well-being of mothers, feelings of confusion, fear, pressure or stress, anxiety, frustration, and guilt can affect the bonding between the mother and child and shape breastfeeding intentions, outcomes, and the decision to stop as well as long-term relationships.19,24,26,27,35,40,48,55,60,61 Factors such as concern for the infant’s health, satiety and satisfaction from infant behavior and cues,19,28,34,42,43,47,49 and maternal perceptions of inadequate milk supply,25–28,33,34,36,37,43,49,51,54,63,65,66 can significantly impact maternal confidence and self-efficacy27,30,38,48,49 and the choices they make between breastfeeding, formula feeding, and supplementation.36,66
Social and environmental factors
The findings indicate a high prevalence of social and environmental factors impacting breastfeeding, including the availability of social support, cultural or institutional practices and beliefs, and socioeconomic issues. Low levels of education and other socioeconomic issues such as age, ethnicity, and income,19,22,27,29,31,33–35,40,41,43,45,46,48,52,57,58,63 as well as gaps in prenatal awareness and knowledge, limited understanding and appreciation of breastfeeding benefits, and a lack of experience or practice,20,21,26,32,35,38,40,42,45,48–50,54,56,57,60,61,64–67 significantly impact breastfeeding attitudes, intentions, initiation, and continuation,20,21,26,32,35,48,55,59,67 often leading to early cessation and supplementation with formula.
Inadequate postbirth counseling, support, and encouragement, particularly for at-risk mothers or those with premature infants, compounds the challenges faced by mothers,28,29,34,35,39,48–50,54,59,64,66,67 ultimately contributing to breastfeeding cessation and often conflicts with the advice of family and friends, culture, or traditions, leading to increased pressure and obligations,29,32,36,38,48,50,55,59–61,64–66 all of which are factors that can influence breastfeeding choices and decisions.
Hospital and nursery policies and clinical practices were also significantly prevalent in the literature as negatively impacting breastfeeding and linked to training and protocols of medical and health staff, such as lack of support or encouragement for initiation and skin-to-skin contact postbirth,22,27,32,35–40,46,48,52,53,59,67 understanding of breast milk benefits or supply development in the puerperium,34,35,48,49,59 bottle use or supplementation with formula as standard,21,26,27,34,39,40,60 and no rooming-in or separation of mother and baby postdelivery and during the hospital stay.26,30,33,35,39,48,67
Much of the literature indicates a direct link between being obliged to return to work and maintaining breastfeeding, including issues with feeling inconvenienced or embarrassed to breastfeed in public or in front of coworkers.24,27,33,34,36,38,41,49,53,59,62,65,66 Workplace-related constraints, including the duration of maternity leave, a lack of private space for feeding or pumping, or safe storage of pumped milk, long working hours, and lack of employer support, further affect decisions to cease breastfeeding.20,21,25,30,33,35–37,44,45,48,49,52,53,55,58,59,62,66,67
Commercial factors
The increasing dependency on artificial formula milk is linked to breastfeeding cessation, posing a significant global public health concern. 22 Poor clinical practices, often based on inaccurate evidence, and misdiagnosis of lactation failure and infant feeding practices contribute to this issue. 22 There are also issues with policies and regulations for the marketing and promotion of artificial formula milk and with clinical guidelines and the use of sources of supplementation, including for neonatal intensive care units, which further hinder the chances of breastfeeding success. 22
Discussion
This scoping literature review aimed to distinguish between lactation failure and breastfeeding cessation to shed light on the issues and distinguish the factors associated with these complex phenomena. The distinction between lactation failure and breastfeeding cessation is crucial in understanding the challenges faced by breastfeeding mothers and the underlying factors influencing these outcomes. The findings of the review indicate a wide variation in the definitions and terminology used to address breastfeeding challenges, which leads to confusion, misdiagnoses, and women being mislabeled and therefore misguided, struggling with perceptions of breast milk insufficiency and a sense of failure, leading to often unnecessary early breastfeeding cessation.
Physiological factors should be clarified and correctly categorized as lactation failure, not breastfeeding failure. Understanding physiological difficulties is essential for health care providers to offer appropriate treatment and interventions to mothers experiencing lactation difficulties while distinguishing from the wider social, mental, emotional, or commercial factors leading to mothers ceasing their attempts to breastfeed and support accordingly.
Addressing mental and emotional challenges during breastfeeding requires a comprehensive approach that includes mental health counseling for breastfeeding mothers that considers all aspects of a woman’s experience and needs in the short and long term, as mental health and well-being influence maternal–infant bonding and the cultivation of strong relationships, and support to navigate the expectations and the realities of early motherhood and parenthood, to better manage the pressures and build resilience to do so successfully, and achieve a better quality of life.
Social and environmental influences are among the most significant contributors to breastfeeding cessation. The review indicates that factors such as lack of support from family and health care providers, societal norms, and workplace policies can profoundly affect breastfeeding practices. The return to work is a major barrier for many mothers, as inadequate maternity leaves and lack of breastfeeding facilities in the workplace force mothers to discontinue breastfeeding earlier than intended. Cultural expectations and societal pressures also play a role in breastfeeding cessation. In some cultures, the use of formula is seen as a status symbol, while in others, extended breastfeeding may be stigmatized. These cultural norms can influence mothers’ attitudes and decisions to start or stop breastfeeding, highlighting the need for culturally sensitive breastfeeding promotion and support programs.
The commercial availability and aggressive marketing of artificial formula milk significantly impact breastfeeding rates. Although our findings in this regard were not many, we appreciate the weight of the work that has been done to review this issue, 22 as well as that of the Lancet Breastfeeding Series, 3 which discuss how artificial formula marketing practices undermine breastfeeding by promoting formula as a convenient and acceptable alternative to breast milk, as well as the issues with gendered power systems and the undervaluing of breastfeeding as care work and of breast milk as a valuable economic commodity, all of which are issues which will require more attention moving forward.
The rates of breastfeeding globally are well known, and it was fascinating to recognize that the factors discussed in the literature were universal, found in many countries around the world, especially with regards to the impact of COVID-19 and the undermining of breastfeeding, 39 and leads us to appreciate that the struggles women face are significant and that more should be done to unravel the complexities and provide increased support that will serve to enhance women’s capacity to breastfeed should they wish to do so.
Strengths and limitations of the study
This study has several strengths, as we used a comprehensive scoping review strategy and considered literature spanning 20 years from 28 countries around the world, which is reflective of the universality of the issues facing mothers in breastfeeding and offers valuable insight into the challenges and complexities of breastfeeding and facilitates the discussions on terminology, definitions used for communication, awareness, education, intervention design and implementation, and their influence on outcomes. There are also several limitations we acknowledge; the review only considered English language studies and may have missed other variations in terminology used to address breastfeeding issues, especially in other cultural contexts. It is important to note that some studies do not consider certain confounding factors of mothers’ circumstances such as poverty, domestic abuse, birth complications or traumatic experiences, the COVID-19 pandemic, or conflict zones. Despite these limitations, our findings may contribute to further addressing these factors in support of breastfeeding initiatives and better outcomes for maternal and infant health and well-being.
Implications for practice and policy
Further research is required to study breastfeeding definitions and terminology, the development of a robust lexicon, detailed consideration of specific factors, and the tailoring of practical and feasible interventions and solutions. These studies should also include qualitative investigations and observational studies, listening to mothers, and designing support according to their individualized needs and circumstances.
Public awareness campaigns and general education curricula should address the challenges and opportunities in the breastfeeding journey, encouraging a social paradigm shift and reducing the confusion and anxiety that many face when entering parenthood and attempting to breastfeed. This will better serve the achievement of breastfeeding goals.
Policymakers should focus on creating more supportive environments for breastfeeding mothers. This includes implementing family-friendly public spaces and workplace policies, providing adequate maternity leave, and ensuring the availability of breastfeeding facilities. Clarity of policies and regulations governing the marketing of artificial formula milk is required to protect and promote breastfeeding practices, prevent misleading information, and support breastfeeding as the optimal feeding choice for infants.
Multidisciplinary guidelines and policies should be developed to mitigate breastfeeding cessation risk factors, enhance the effectiveness of solutions, and expand service provision (counseling and support options).
Health and social support facilities should work to develop information and guidance in local languages and offer multiple options for counseling, both in person and virtually, to facilitate mothers’ access.
Health care provider training should be reoriented in light of the distinctions between the two concepts of lactation failure and breastfeeding cessation with clear terminology and definitions, which will improve their ability to identify mothers at risk and offer appropriate treatment and support. Mothers should be provided with appropriate information during their antenatal care, and provided with consistent intrapartum and postpartum support to best manage the breastfeeding issues they may face.
Conclusions
In our comprehensive scoping review, we acknowledge the complexity of the factors that underlie lactation failure and breastfeeding cessation, stemming from variations in the terminology and definitions used to communicate, provide awareness and education, and in the design and delivery of interventions and support for initiation and continuation of breastfeeding. Further in-depth research and analysis of the complex issues and factors influencing breastfeeding practices is required. By understanding the physiological, mental, emotional, social, and commercial factors identified in this review, health care providers, policymakers, and researchers can work together to facilitate supportive environments that promote and sustain breastfeeding for the benefit of both mothers and infants.
Footnotes
Authors’ Contributions
M.B.: Conceptualization, methodology, software, validation, formal analysis, investigation, resources, writing—original draft, writing—review and editing, supervision, and project administration. H.Z.: Conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, and visualization.
Disclosure Statement
The authors declare no conflict of interest.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.