
Abstract
Background:
Before the COVID-19 pandemic, research studies indicated that breastfeeding was protective against postpartum depression (PPD). This study aimed to evaluate the impact of the COVID-19 pandemic on the protective association between breastfeeding and PPD.
Methods:
We performed a retrospective cohort study by comparing the Edinburgh Postnatal Depression Scale (EPDS) scores for patients in two cohorts, pre-COVID-19 (April 2019 to February 2020) and COVID-19 (April 2020 to February 2021). A cross-sectional design using descriptive statistics, Pearson correlations, analysis of variance (ANOVA), and stepwise multiple regression analysis (MRA) analyzed the EPDS scores of a prepandemic cohort (N = 448) and a pandemic cohort (N = 468) of women seen at a tertiary academic medical center for their first postpartum visit.
Results:
In the prepandemic cohort, 77.3% of breastfeeding women exhibited an unlikely risk for PPD compared with 78.5% in the pandemic cohort. Pearson correlations showed that the breastfeeding group in both cohorts had significantly lower EPDS scores, was less likely to exhibit PPD, and had a lower risk of severe PPD. ANOVA showed that nonbreastfeeding women had significantly higher EPDS scores in both cohorts. Stepwise MRA showed that the EPDS item Q8 (“I have felt sad or miserable”) was the most significant predictor of PPD in breastfeeding women (both cohorts) and nonbreastfeeding women (prepandemic cohort) but had escalated to Q9 (“I have been so unhappy that I have been crying”) for nonbreastfeeding women in the pandemic cohort.
Conclusion:
In both the prepandemic and pandemic cohorts, breastfeeding women had significantly lower EPDS scores.
Introduction
On March 11, 2020, the World Health Organization (WHO) declared COVID-19 a global pandemic caused by the severe acute respiratory syndrome known as SARS-CoV-2. 1 The health implications of breastfeeding for mothers and infants were more complex during the pandemic, requiring more in-depth analysis. Since breast milk did not appear to transmit SARS-CoV-2, mothers diagnosed with COVID-19 were encouraged to breastfeed with appropriate precautions since the absence of breastfeeding and mother–baby separation are associated with adverse health and emotional outcomes.1,2 Breastfeeding provides numerous benefits for the mother and infant, including protection from gastrointestinal and respiratory infections. 3 Breastfed infants have reduced risks for infectious morbidity, childhood obesity, diabetes, leukemia, and sudden infant death syndrome. Breastfeeding mothers have reduced risks for premenopausal breast cancer, ovarian cancer, weight gain, diabetes, myocardial infarction, and metabolic syndrome. 4
Most COVID-19 pandemic perinatal research studies have focused on maternal–infant physiological consequences. Fewer research studies have focused on the maternal mental health challenges impacted by the pandemic. 5 Studies have shown worsening mental health, especially those with risk factors for anxiety and depression.6,7 Postpartum depression (PPD) is a known postpartum mood disorder that can be seen up to a year after delivery and is associated with lower rates of breastfeeding. 8 Women who have difficulty breastfeeding, severe pain with breastfeeding, or early discontinuation of breastfeeding have increased rates of PPD. 9
Although several studies suggest that an association exists between breastfeeding and PPD, the pathophysiology of PPD is not yet fully understood due to its complexity. 10 Breastfeeding initiates hormonal responses that protect mothers against PPD, including oxytocin, prolactin, and adrenocorticotropic hormones.11,12 The hormonal theory of PPD helps explain how breastfeeding may safeguard mothers against PPD. 13 Other theoretical perspectives include biological, psychosocial, and evolutionary. 14 From a physiological standpoint, breastfeeding provides the optimum food source of nutrients and the first line of defense against infection. 15 From a psychological perspective, breastfeeding forms the earliest psychological bond between the mother and child.
Before the COVID-19 pandemic, the WHO recommended exclusive breastfeeding for the first 6 months of a child’s life to increase the infant’s and mother’s positive health outcomes. 16 During the pandemic, the WHO and UNICEF advised and reinforced the importance of breastfeeding when sufficient methods were in place to prevent the spread of COVID-19.17–19 Evidence supported the recommendation to continue breastfeeding during the pandemic, showing the mortality risk is 14× higher for infants not breastfed than infants breastfed exclusively, as breastfeeding protects against infectious diseases that disproportionately affect the most vulnerable infants.
The United States Preventative Services Task Force (USPSTF) and the American College of Obstetricians and Gynecologists (ACOG) recommend screening for perinatal depression both during pregnancy and in the postpartum period. To increase the accuracy and detection of PPD, ACOG recommends using a validated postpartum screening tool. 20 The USPSTF, ACOG, and the American Academy of Pediatrics recommend the Edinburgh Postnatal Depression Scale (EPDS) 21 questionnaire for PPD screening. The EPDS questionnaire comprises 10 Likert-scale questions about PPD symptoms. 22 If the patient’s EPDS score meets or exceeds a predetermined threshold, a follow-up clinical assessment determines the appropriate diagnosis and treatment. 23
The study’s primary objective was to investigate the impact of the COVID-19 pandemic on the protective association between breastfeeding and PPD by performing a comparative analysis of prepandemic and pandemic cohorts.
Materials and Methods
With IRB approval, we conducted a retrospective cohort study utilizing electronic medical records at a tertiary academic medical center. The Integrated Data Repository (IDC) provided investigators with a randomized list of medical record numbers based on the study’s inclusion criteria and time frame. Patients were selected based on the following inclusion criteria: (1) patients at least 18 years old, (2) patients who completed an EPDS survey during their first postpartum visit, and (3) delivered within a specified time frame discussed below. The patients represented two cohorts, pre-COVID-19 (April 2019 to February 2020) and COVID-19 (April 2020 to February 2021). This study included 916 patients in the two cohorts (pre-COVID-19: N = 448; COVID-19: N = 468). This study used several quantitative methods and a cross-sectional design to evaluate the protective association between breastfeeding and postpartum depression before and during the pandemic. Figure 1 shows the research flowchart, including the selection of participants, inclusion criteria, and data analysis.
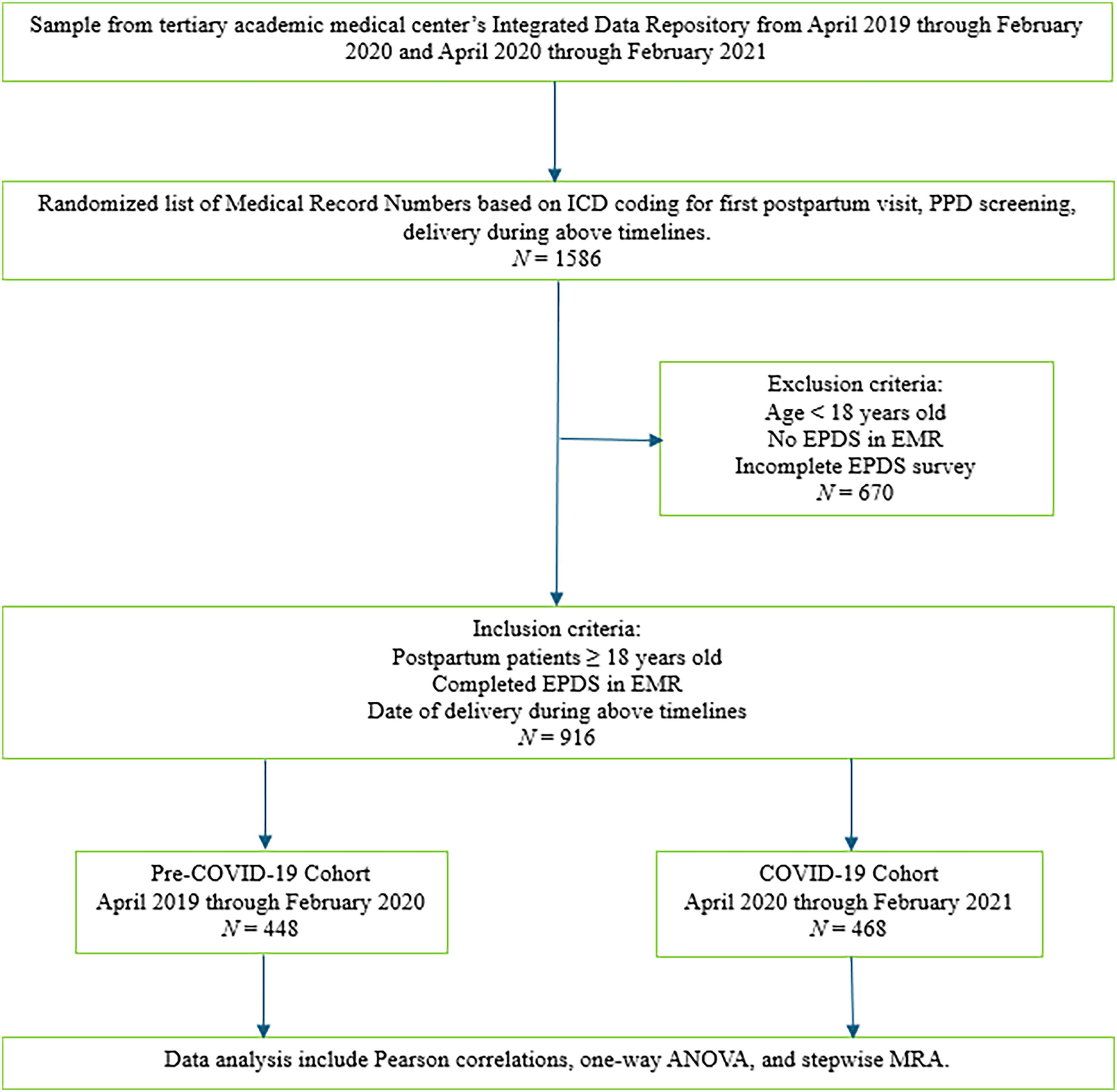
Research flowchart showing the research process, including the selection of participants, inclusion criteria, and data analysis.
Measuring instrument
The measuring instrument used in the study was the EPDS questionnaire developed by Cox et al. 21 The EPDS is a 10-item self-administered screening questionnaire asking the participants about possible depressive symptoms during the postpartum period. Each question has response choices from zero to three, with the total score ranging from 0 to 30. The higher the score, the more likely the patient has PPD.
The EPDS is the most frequently validated screening tool for PPD, with validations in 37 languages. 24 Whether validating EPDS scores against the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5) and International Classification of Diseases, 10th Revision (ICD-10) depression criteria, the results are consistent with no significant differences. At a cutoff score of nine or more, the sensitivities were 83.9% and 83.5%, and specificities were 89.4% and 89.4% for the DSM-5 and ICD-10, respectively. At a cutoff score of 12 or more, the sensitivities were 72.5% and 72.2%, and the specificities were 96.9% and 96.9% for the DSM-5 and ICD-10, respectively.
A systematic review of 37 studies validating the EPDS used in screening for PPD found a 9/10 cutoff score for possible PPD and 12/13 for probable PPD consistently used. 25 The researchers who developed and validated the EPDS also used 9/10 cutoff scores for possible depression and 12/13 for probable depression. 21 This study utilized four EPDS thresholds: 0–8, 9–11, 12–14, and 15–30, corresponding to unlikely, probable, moderate, and severe risk of PPD shown in Table 1.
Edinburgh Postnatal Depression Scale Cutoff Scores for Postpartum Depression Risk
EPDS, Edinburgh Postnatal Depression Scale; PPD postpartum depression.
Statistical analysis
IBM SPSS Statistics for Windows, version 28.0, performed the statistical analysis. Cronbach’s α provided the reliability analysis of the EPDS items for the questionnaire completed by each cohort. Pearson correlations evaluated the associations between breastfeeding and EPDS scores, including age, race, and EPDS thresholds. One-way analysis of variance (ANOVA) assessed whether significant differences existed in the EPDS score between the breastfeeding and nonbreastfeeding groups within each cohort. Stepwise multiple regression analysis (MRA) determined how much variance was explained by each EPDS item relative to the overall EPDS score for the breastfeeding and nonbreastfeeding groups in each cohort.
Results
Cronbach’s α, is the most recognized internal consistency and scale reliability measure for instruments used in medical education research, 26 with a recommended range from 0.70 to 0.95. 27 The EPDS questionnaire comprised 10 questions that exhibited high internal consistency and scale reliability for the pre-COVID-19 cohort (Cronbach’s α = 0.91) and the COVID-19 cohort (Cronbach’s α = 0.92).
Table 2 shows the descriptive statistics for breastfeeding, age, and race, including the EPDS score for the pre-COVID-19 and COVID-19 cohorts. In almost all cases, across all categories, the EPDS score increased in the pandemic cohort compared with the prepandemic cohort. The exceptions include EPDS score decreases for nonbreastfeeding patients in the pandemic categories 31–35 age-group (7.9 to 6.5) and other races (5.4 to 4.8).
Comparison of the Pearson Correlations (r) Between Breastfeeding, Age, Race, and the Edinburgh Postnatal Depression Scale Score for the Pre-COVID-19 Cohort and the COVID-19 Cohort
Sig. p-value is two-tailed.
Insufficient data.
EPDS, Edinburgh Postnatal Depression Scale; M, mean; SD, standard deviation.
The overall prevalence of breastfeeding remained relatively consistent for the pre-pandemic (72.5%) and pandemic cohorts (74.6%). Among the age-groups, the prevalence of breastfeeding, prepandemic to pandemic, in the 18–24 age-group increased from 67.0% to 68.5%, in the 25–30 age-group increased from 68.8% to 72.5%, in the 31–35 age-group decreased from 80.7% to 77.6%, and in the 36 and older age-group increased from 70.3% to 79.4%. Among the race categories, the prevalence of breastfeeding, prepandemic to pandemic, increased for White patients from 74.2% to 75.4%, increased for Hispanic patients from 78.9% to 83.7%, increased for Black patients from 59.6% to 66.4%, remained the same for Asian parents at 100%, and decreased for other races from 80.0% to 78.6%.
Table 2 compares the Pearson correlations (r) between breastfeeding, age, race, and the EPDS score for the pre-COVID-19 and COVID-19 cohorts. In the prepandemic cohort, breastfeeding (r = −0.25, p < 0.001) was negatively correlated to the EPDS score, indicating that breastfeeding is significantly associated with a lower risk of PPD. In the pandemic cohort, breastfeeding (r = −0.13, p = 0.005) remained negatively correlated to the EPDS score. Although the effect size decreased during the pandemic, the association remained significant. In both cohorts, breastfeeding patients aged 25 to 30 showed protective benefits against PPD (prepandemic: r = −0.33, p < 0.001; pandemic: r = −0.22, p = 0.007). Breastfeeding patients aged 31 to 35 in the prepandemic cohort showed protective benefits against PPD (r = −0.29, p < 0.001). However, no significant benefit appeared in the breastfeeding patients in the 31–35 age pandemic cohort. In either cohort, the 18–24 and 36 and older patients showed no significant correlation between breastfeeding and PPD. In both cohorts, White breastfeeding patients showed protective benefits against PPD (prepandemic: r = −0.26, p < 0.001; pandemic: r = −0.22, p < 0.001). Black breastfeeding patients in the prepandemic cohort showed protective benefits against PPD (r = −0.23, p = 0.019). However, no significant benefit appeared in the Black breastfeeding patients in the pandemic cohort. In either cohort, the Hispanic, Asian, and patients listing their race as other showed no significant correlation between breastfeeding and PPD.
Table 3 shows the descriptive statistics for breastfeeding within each PPD risk category under investigation, including unlikely PPD (EPDS <9), probable PPD (EPDS ≥9), mild PPD (EPDS 9 to 11), moderate PPD (EPDS 12 to 14), and severe PPD (EPDS ≥15), for the pre-COVID-19 and COVID-19 cohorts. In the group unlikely to exhibit PPD (EPDS <9), the prevalence of breastfeeding increased slightly from 77.3% prepandemic to 78.5% pandemic. Still, the prevalence of breastfeeding decreased from 62.3% prepandemic to 52.9% pandemic relative to the total patients in each cohort (pre: N = 448; pandemic N = 468). In both cohorts, the Pearson correlation showed that breastfeeding had a significant correlation for patients unlikely to exhibit PPD (pre: r = 0.22, p < 0.001; pandemic: r = 0.12, p = 0.009).
Comparison of the Pearson Correlations (r) Between Breastfeeding and the Edinburgh Postnatal Depression Scale Thresholds for the Pre-COVID-19 Cohort and the COVID-19 Cohort
Sig. p value is two-tailed.
EPDS, Edinburgh Postnatal Depression Scale; PPD, postpartum depression.
In the group that exhibited mild PPD (EPDS 9 to 11), the prevalence of breastfeeding decreased from 76.9% prepandemic to 72.4% pandemic. The prevalence of breastfeeding increased from 4.5% to 9.4% relative to the patients in each cohort. In both cohorts, the Pearson correlation showed no significant relationship between breastfeeding and patients who exhibited mild PPD (pre: r = 0.02, p = 0.607; pandemic: r = −0.02, p = 0.687). In the group that exhibited moderate PPD (EPDS 12 to 14), the prevalence of breastfeeding increased from 50.0% prepandemic to 75.0% pandemic. The prevalence of breastfeeding increased from 3.1% to 6.7% relative to the patients in each cohort. In the prepandemic cohort, the Pearson correlation showed a significant negative relationship between breastfeeding and patients who exhibited moderate PPD (r = −0.13, p = 0.006). The pandemic cohort had no significant relationship (r = 0.00, p = 0.948).
In the group that exhibited severe PPD (EPDS ≥15), the prevalence of breastfeeding increased from 36.4% prepandemic to 58.8% pandemic. The prevalence of breastfeeding also rose from 2.7% prepandemic to 8.9% pandemic relative to the total patients in each cohort (pre: N = 448; pandemic N = 468). In both cohorts, the Pearson correlation showed that breastfeeding had a significant negative correlation for patients who exhibited severe PPD (pre: r = −0.23, p < 0.001; pandemic: r = −0.15, p = 0.001).
One-way ANOVA tested whether significant differences existed in the EPDS scores between the breastfeeding and nonbreastfeeding groups within each cohort. Table 4 shows the one-way ANOVA between each cohort’s breastfeeding and nonbreastfeeding groups. The results showed significantly higher EPDS scores [F (1,158) = 19.2, p < 0.001, η2 = 0.06] in the pre-COVID-19 cohort for the nonbreastfeeding group (mean [M] = 7.5, standard deviation [SD] = 7.3) compared with the breastfeeding group (M = 4.4, SD = 4.5). The results also showed significantly higher EPDS scores [F (1,165) = 5.9, p = 0.017, η2 = 0.02] in the COVID-19 cohort for the nonbreastfeeding group (M = 8.6, SD = 7.9) compared with the breastfeeding group (M = 6.7, SD = 5.9).
One-Way Analysis of Variance Between Each Cohort’s Breastfeeding and Nonbreastfeeding Groups Using the Edinburgh Postnatal Depression Scale Score as the Criterion
F-ratio calculated using Welch statistic.
EPDS, Edinburgh Postnatal Depression Scale; SD, standard deviation.
Stepwise MRA calculates models to determine how much variance predictor variables explain an outcome variable. 28 Figure 2 is a quadrant showing a summary of four predictive models using the EPDS items as predictor variables and the EPDS score as the outcome variable. For the breastfeeding groups in both cohorts, the EPDS item, Q8. Sad_miserable, explained the most significant variance of the EPDS score (pre: ΔR2 = 66.7%; pandemic: ΔR2 = 71.3%). The EPDS item Q8 also explained the most significant variance in the EPDS score (ΔR2 = 77.4%) for the nonbreastfeeding group in the prepandemic cohort. However, for the nonbreastfeeding group of the pandemic cohort, the EPDS item, Q9. Unhappy_crying, explained the most significant variance of the EPDS score (ΔR2 = 82.6%).
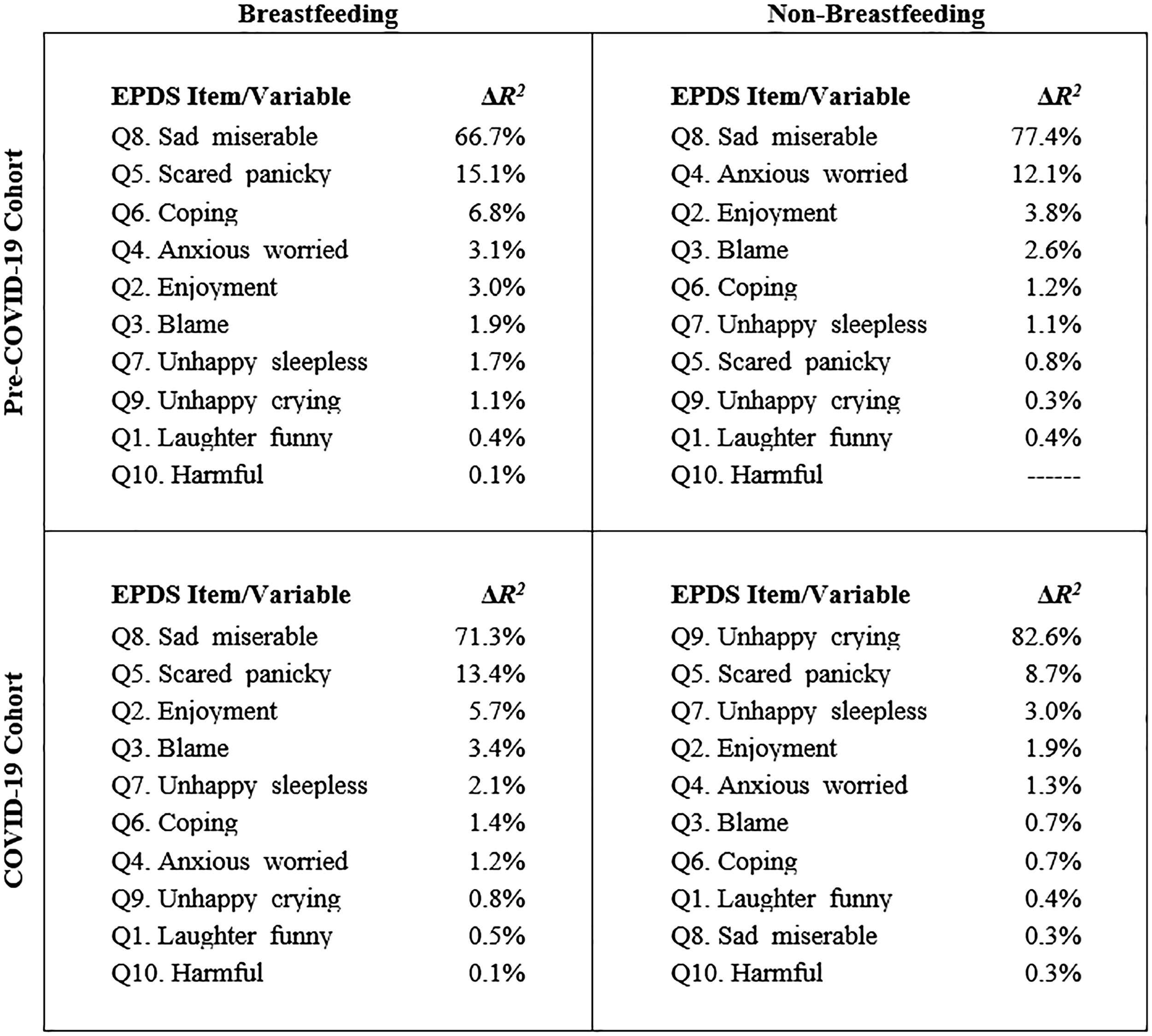
Multiple regression analysis (MRA) quadrant of models showing the variance of the Edinburgh Postnatal Depression Scale (EPDS) scores explained by the EPDS item/variable for the breastfeeding groups and the cohorts.
Discussion
This study investigated the protective benefit of breastfeeding on PPD before and after the onset of the COVID-19 pandemic by performing a comparative analysis of prepandemic and pandemic cohorts. Before the pandemic, evidence showed that breastfeeding provided physical and mental health benefits and protections for the mother and child.17,29 Our study showed that breastfeeding protected mothers against PPD during the pandemic based on EPDS scores. 21 Although the effect size of the protective benefit of breastfeeding on PPD lessened during the pandemic, this protective benefit remained significant.
PPD is frequently underdiagnosed, resulting in patients not receiving the necessary and applicable treatment. PPD can produce adverse outcomes for mothers, children, and families.8,22,23 If properly diagnosed, PPD is treatable. 23 Assessing risk factors, such as breastfeeding difficulties, and applying appropriate interventions may prevent PPD. 22 Evidence shows that PPD increases the risk for poor infant health outcomes due to compromised maternal–infant interactions. 30 Interventions for women with PPD may alleviate their symptoms, resulting in improved outcomes for their offspring. PPD is associated with lower attendance at well-child visits, decreased childhood immunizations, and sudden infant death syndrome. 31 When depression is present in the first 6 months postpartum, poor attachment, early childhood and adolescent behavioral problems, 32 poor language development, 33 and increased childhood gastrointestinal and respiratory infections are more common. 34
In early 2020, the COVID-19 pandemic disrupted professional and private lives, exacerbated by the implementation of quarantine measures. 5 The psychological impact of the pandemic associated with the lockdown and fear of infection negatively impacted women’s mental health, including those who already had known risk factors for PPD. One research study reviewed the evidence from 12 studies showing that COVID-19 disrupted prepandemic breastfeeding plans, resulting in adverse mental health outcomes. 35
A significant strength of this study is that it was the first to compare the associations between breastfeeding and PPD between two cohorts, one before the COVID-19 pandemic and one during the pandemic, from a tertiary academic medical center. Prior studies of the association between breastfeeding and PPD have limited their time frames to before and after the pandemic or used comparisons between disparate groups. Our study showed analogous results before and during the pandemic. Breastfeeding women (pre: M = 4.4, SD = 4.5; during: M = 6.7, SD = 5.9) had lower EPDS scores than nonbreastfeeding women (pre: M = 7.5 SD = 7.3; during: M = 8.6, SD = 7.9). Before and during the pandemic, breastfeeding women were significantly more unlikely to exhibit PPD symptoms (EPDS < 9) before (r = 0.22, p < 0.01) and during the pandemic (r = 0.12, p < 0.01). Severe PPD symptoms (EPDS ≥ 15) before (r = −0.23, p < 0.01) and during the pandemic (r = −0.15, p < 0.01) were significantly less likely in breastfeeding women. Our study showed that although the effect size for breastfeeding women decreased during the pandemic, the protective benefit against PPD remained significant.
The stepwise MRA results in this research study showed that before the pandemic, women in both the breastfeeding and nonbreastfeeding groups selected the EPDS item “I have felt sad or miserable” as the most significant predictor of PPD. During the pandemic, women in the breastfeeding group chose the same item. In contrast, women in the nonbreastfeeding group selected “I have been so unhappy that I have been crying” as the most significant predictor of PPD. The change of the most significant PPD predictor symptom from “sad or miserable” to “unhappy and crying” only affected nonbreastfeeding women during the pandemic, demonstrating the protective benefit of breastfeeding.
Assessment of location and EPDS cutoff thresholds may decrease the generalizability of the results and is, therefore, a limitation of this study. According to the Centers for Disease Control and Prevention’s Breastfeeding Report Card, breastfeeding rates vary significantly by region. 36 For infants born in Florida, USA, the location of this study, 71.0% of mothers breastfed compared with 94.0% in Colorado or 59.8% in West Virginia. Although the EPDS is used extensively in several countries and validated in 37 languages, studies show that the cutoff scores vary considerably. 24 Potential variations in cutoff scores include different PPD criteria, diagnostic systems, and cultural differences in the communication of depressive systems.24,25 Future research studies could consist of evaluating data from various regions.
Conclusion
Our research is consistent with prior studies showing that breastfeeding women exhibit a lower prevalence of PPD and lower EPDS scores than nonbreastfeeding women. Our research contributes to this body of knowledge by extending the evidence that breastfeeding maintained a significant positive association with a lower prevalence of PPD and lower EPDS scores during the COVID-19 pandemic. This research study was the first to compare the association between the protective benefits of breastfeeding and PPD between two cohorts from a tertiary academic medical center before and during the COVID-19 pandemic. The pandemic placed additional mental stress on postpartum women, placing them at greater risk of PPD. This research study showed that EPDS scores for breastfeeding women were significantly lower in both cohorts. This research study also showed that nonbreastfeeding women were significantly more likely to exhibit probable PPD and severe PPD risk. Although the effect sizes of these associations were smaller during the pandemic, the protective benefits of breastfeeding remained significant.
Footnotes
Authors’ Contributions
Study conception and design: A.V. Oversight and mentorship: D.R.-R. Data collection: A.V. Analysis and interpretation of results: A.V. and D.E.V. Synthesis and curation of data: D.E.V. Draft article preparation and writing: A.V. and D.E.V. All authors read and approved the final article.
Ethics Approval and Consent to Participate
The institutional review board approved this study at the University of Florida (IRB202100513). This study involves secondary research, which does not require informed consent and receives exempt status.
Data Availability
The datasets used and analyzed during the current study are available from the corresponding author at a reasonable request.
Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this article.