
Abstract
Abstract
Objective:
To determine the possible relationship between pain experienced by mothers with breastfeeding and musculoskeletal impairment commonly seen in physiotherapy practice. Evidence-based principles of the evaluation and treatment of musculoskeletal impairment used in physiotherapy practice were applied and adapted to manage pain experienced by mothers with breastfeeding.
Subjects and Methods:
This report describes 11 mothers referred to a breastfeeding clinic for pain with breastfeeding. Mothers were initially assessed by a physician and a nurse clinician, both International Board-Certified Lactation Consultants, to rule out causes of breast or nipple pain. When the cause remained unexplained, it was deemed musculoskeletal, and mothers were referred to a physiotherapist for assessment and treatment with manual orthopedic therapy and mobilization of the myofascial system.
Results:
The physiotherapist's objective musculoskeletal assessment and mothers' impression showed an improvement in the overall clinical picture after the first appointment in most mothers. Pain was resolved or alleviated by 80% in five mothers after 1–3 weekly treatments. The most useful therapeutic approach was to make afflicted mothers aware of their posture to maintain spinal alignment and avoid shear posture (lateral displacement of the trunk). Shear posture is a consequence of sitting leaning to one side. This posture is exacerbated by thoracic rotation and flexion, for example, when turning the trunk and bending over the baby while giving the breast.
Conclusion:
Treating musculoskeletal impairment referred pain to the breast or nipple with physiotherapy practices used in a nonbreastfeeding clientele can help alleviate or resolve pain with breastfeeding.
Introduction
Persistent breast or nipple pain associated with breastfeeding is common. In one study, as many as 29.3% of mothers who stopped breastfeeding during the first month postpartum reported pain. 1 In another study, 20% of breastfeeding mothers still had nipple pain after 8 weeks postpartum. 2 Pain associated with breastfeeding is a common reason cited by mothers who did not reach their breastfeeding goals. 3
Musculoskeletal breast or nipple pain in nonbreastfeeding clientele is managed with physiotherapy.
Literature linking musculoskeletal disorders to breast or nipple pain with breastfeeding is scarce and, to our knowledge, there is only one reported case series attributing breastfeeding-related mastalgia of unknown etiology to muscle constriction. 4
The objective of this case series was to determine the possible relationship between pain experienced by mothers with breastfeeding and musculoskeletal impairment seen in physiotherapy practice. Management of musculoskeletal impairment used in physiotherapy practice in a nonbreastfeeding clientele was applied and adapted to manage breast or nipple pain experienced by mothers with breastfeeding.
Subjects and Methods
Rationale for referral to physiotherapy
The thorax is an area rich in anatomical structures that can be a source of referred pain to the breast such as muscles, fascia, joints, nerves, brachial plexus, and sympathetic nerve fibers. 5 Furthermore, the biomechanics of the thorax or optimal movement pattern is complex because each of its thoracic rings moves in synergy with all other thoracic rings. A thoracic ring consists of two ribs of the same number and the vertebrae to which they attach and the anterior costal attachments to the sternum. 6 Optimal biomechanics of the thorax is facilitated by neutral spinal alignment within the thorax. When a thoracic ring is abnormally translated and rotated, the ribs are unable to move correctly. Therefore, impairment of the biomechanics or optimal movement pattern of one or many rings may induce an intrathoracic segmental rotation or ring shift and affect thoracic muscles, fascia, joints, and nerves, which can refer pain to the nipple or breast. Referred pain is pain felt at a site remote from the site of origin.7–9 Furthermore, musculoskeletal conditions in regions surrounding the thorax, such as cervical, scapular, shoulder girdle, lumbar, and pelvic regions, can also be responsible for referred pain to the breast or modified thoracic biomechanics. Poor biomechanics of the thorax is often associated with multiple conditions across a wide variety of populations and optimal thoracic function is paramount for good health.6,10–13
Initial assessment and patients
Seventeen mother–baby dyads were assessed in a community hospital ambulatory breastfeeding medicine clinic. Mothers and babies in need of medical expertise regarding breastfeeding challenges are referred to this clinic by perinatal nurses and physicians. Mothers presenting for pain with breastfeeding were assessed by a physician and a nurse clinician, both International Board-Certified Lactation Consultants (IBCLCs). Mothers were assessed for usual causes of breast or nipple pain such as nipple damage (abnormal latch/suck dynamic or breast pump trauma/misuse), dermatosis infection, and vasospasm. 14 The physician and nurse, both IBCLCs, did a complete medical background history of mother and baby, pregnancy, birth and breastfeeding history, physical examination of baby and mother, and observation of a breastfeeding session. Between June 2015 and September 2017, 17 mothers assessed for pain with breastfeeding were referred to physiotherapy when the cause remained unexplained. It was deemed musculoskeletal in presence of a circumscribed unilateral or bilateral spot of sharp tenderness along the anterior axillary line close to the lateral border of the breast on physical examination. With the exception of two patients, all had pain since their baby's birth. They started physiotherapy appointments between the first and the 35th week after giving birth.
Of the 17 participant mothers, 6 were excluded from the case series because physiotherapy treatments were stopped. Two mothers were not seen for follow-up after first treatment. One mother had stopped breastfeeding and did not want to pursue treatments after two appointments. One mother did not notice any improvement and stopped after three treatments. Two mothers had concurrent mastitis. The 11 remaining mothers completed the treatments as prescribed. A physiotherapy chart review was performed to complete the musculoskeletal history after the treatments. All mothers gave written consent to report anonymously on the assessments and results of treatments.
Treatment
Mothers were treated weekly by a physiotherapist certified in orthopedic manual therapy. Principles of evaluation and treatment of thoracic pain in physiotherapy practice were applied and adapted to manage pain experienced by mothers with breastfeeding. Based on the physiotherapist's assessment findings, an individualized treatment plan was developed to relieve thoracic pain according to evidence-based techniques and approaches in nonbreastfeeding clientele.6,10–13 Treatments started on the first appointment. Treatment essentially consisted, after thorough assessment, in advising mothers to avoid shear posture (lateral displacement of the trunk) at all times. Shear posture is a consequence of sitting leaning to one side. This is exacerbated by thoracic rotation and flexion, for example, when turning the trunk and bending over the baby while giving the breast. At subsequent appointments, treatments consisted of reinforcing guidance on good postural habits, orthopedic manual therapy such as reducing tension of hypertonic muscles, increasing control of weakened muscles, mobilizing joints to gain a greater range of mobility within the rib cage, and mobilizing the myofascial system.
Results
The following Table 1 contains all the pertinent information related to the assessment and results of the physiotherapy treatments provided to the 11 mothers experiencing breast or nipple pain with breastfeeding.
Clinical Characteristics of Patients as per Physiotherapy Assessment and Time to Pain with Breastfeeding Reduction in Weeks
During the first physiotherapy assessment there was no consistency in pain descriptions reported by mothers. Ten out of 11 mothers had a localized unilateral or bilateral spot of deep tenderness along the anterior axillary line close to the lateral border of the breast. A thoracic ring biomechanical impairment was found on at least one of the thoracic rings in 10 of the 11 mothers. Moreover, a muscular tension overcharge was noticed in all 11 mothers in the following muscles (Fig. 1): serratus anterior (attaches from lateral ribs 1–9 to scapula), pectoralis minor (attaches anterior ribs 3–5 to scapula), rhomboids (attach from vertebras C7-T5 to scapula), trapezius (attaches from cervical and thoracic area to scapula and collarbone), external oblique (attaches from lateral ribs 5–12 to linea alba, thoracolumbar fascia, and pelvis), and paraspinal muscles (attach to ribs and vertebrae). A postural anomaly for thoracic kyphosis (six mothers) or thoracic flatness (three mothers) was an important contributing factor. In addition, shoulder girdle postural anomalies such as scapular protraction or an anteriorly displaced glenohumeral joint were found in eight mothers. During movement assessment, a neuromuscular girdle instability (impairment of movement control) in scapular or abdominal-lumbar-pelvic girdle was objectified in all 11 mothers.
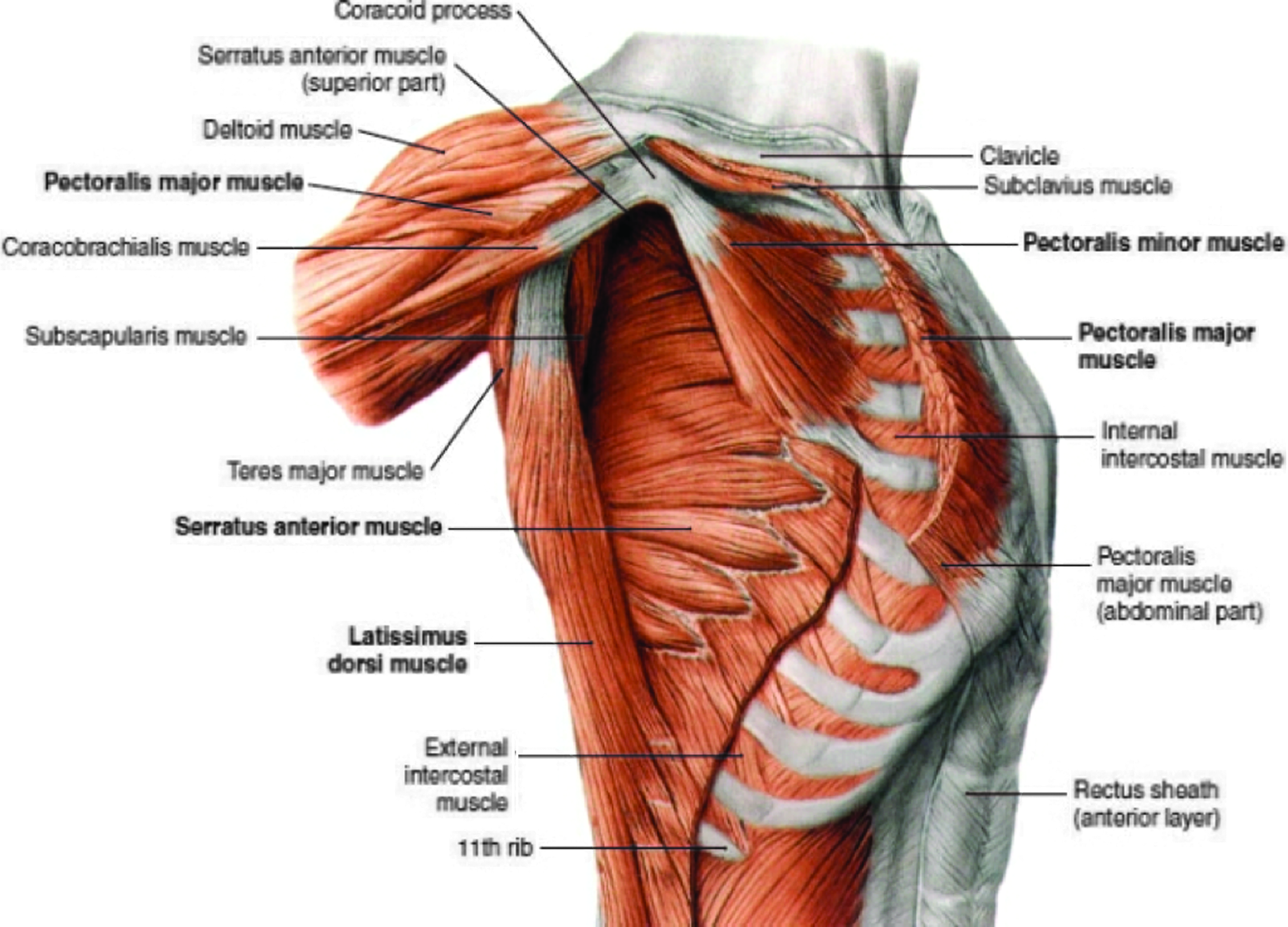
Pectoralis minor, serratus anterior, and latissimus dorsi muscles, lateral view (right). Original source: Benninghoff, Lehrbuch der Anatomie des Menschen ©Elsevier GmbH, Urban & Fischer, Munich. 5 With courtesy and permission of foreign rights, Elsevier, EMEALA Health.
Overall musculoskeletal condition was reassessed during each appointment. This included comparing with the initial visit for decreased muscle tension, fewer postural anomalies, improvement in movement control of the scapular and abdominal-lumbar-pelvic girdle, increase in the articular range of motion, and reduction of pain during costal palpation (data not shown). The two criteria retained to report progress are reduction of pain with breastfeeding and number of treatments required to attain this result.
The physiotherapist's objective musculoskeletal assessment and mothers' impressions showed an improvement in the overall clinical picture after the first appointment in most mothers. Among the 11 mothers receiving weekly treatments, pain was completely resolved or 80% alleviated in 5 mothers after one to three treatments and in 3 mothers after four to five treatments. The last three mothers saw their pain completely resolved, 90% alleviated or 80% alleviated after seven to eight treatments. It is interesting to note that the five mothers who required only one to three treatments to resolve or markedly alleviate their pain had experienced pain with breastfeeding for an average of 9.8 weeks (range 1–20 weeks). When chronic musculoskeletal conditions were present, for example, to the cervical, dorsal, lumbar, or shoulder girdle levels, more physiotherapy treatments were required to diminish or stop the pain with breastfeeding.
In reviewing the charts retrospectively, we found that five mothers had a documented history of a past or current head, jaw, neck, shoulder, back, or pelvic musculoskeletal impairment.
Discussion
In this case series, we looked at 11 mothers presenting with unexplained pain with breastfeeding for whom the overall clinical picture was improved after their first appointment in physiotherapy treatment, which essentially consisted of postural alignment guidance. The pain was resolved or significantly alleviated after one to three treatments in 5 out of the 11 mothers.
A case report has already proposed that breast pain could be caused by a thoracic muscle constriction on the mammary neurovasculature. 4 We suggest that musculoskeletal impairment in the thorax or within its vicinity could induce referred pain to the breast or nipple.
Shear posture (lateral displacement of the trunk) is one consequence of sitting leaning to one side or leaning sideways toward the baby while giving the breast. This posture could impair thoracic biomechanics and affect thoracic muscles, fascia, joints, and nerves, all of which can refer pain to the nipple or breast. During pregnancy, cervical and lumbar lordoses, as well as thoracic kyphosis, both increase. The abdomen and breasts expand. These conditions could continue in postpartum to influence thoracic ring movement, tension within joints, muscles, and fascia, thus contributing to referred pain to the breast or nipple. Furthermore, poor ergonomic postures requiring trunk rotation and forward bending, for example, when picking up the baby or carrying the infant in a car seat, may compound these factors.
When assessing unexplained pain with breastfeeding, we propose to broaden the differential diagnosis and to investigate for referred pain from musculoskeletal impairment using the same approach as for nonbreastfeeding patients experiencing thoracic pain. This is usually done by collecting general history regarding occupations, sport, or hobbies involving misaligned posture (shear posture, rotation, and forward bending of the trunk), repetitive movements such as pushing, pulling and lifting, and past or current musculoskeletal injuries. 6 On physical examination, we suggest looking for postural anomalies (exaggerated thoracic kyphosis, scapular protraction, or glenohumeral anteriority) and for a circumscribed unilateral or bilateral spot of sharp tenderness along the anterior axillary line close to the lateral border of the breast.
Breastfeeding mothers are frequently advised to place their baby so that their baby's head, neck, and body line up. In the same vein, a posture favoring the mother's neutral spine alignment and avoiding shear posture can be a simple and logical recommendation to ease or end unexplained pain during breastfeeding. Also, encouraging mothers to breastfeed in a semireclined position15–17 enhances not only the babies' but also mothers' comfort because it allows the spine to rest in a neutral alignment. When simple postural education is insufficient, treatment for musculoskeletal impairment referring pain to the breast or nipple could alleviate or stop pain with breastfeeding.
There is a need for outcome research in the population of mothers experiencing unexplained pain with breastfeeding to provide evidence basis for treatment of musculoskeletal impairment. Another area of research could be to link vasospasm with musculoskeletal impairment because high intensity referred muscle pain has already been linked to autonomic reflexes. 8 Likewise, we propose that a shift of one or several ribs could also affect the sympathetic ganglia lying just beneath the rib close to the thoracic spine. We hypothesize that impairment of thoracic biomechanics could impinge upon thoracic sympathetic fibers responsible for the innervation of peripheral vascular smooth vessels of the skin, which are responsible for vasospasms.
Conclusions
Breast or nipple pain with breastfeeding is common and could prevent mothers from reaching their breastfeeding goals. Teaching awareness of the neutral spine position is key to improving comfort when experiencing pain with breastfeeding. When simple postural education is insufficient, a referral to a physiotherapist who has been trained in the thoracic ring concept is warranted. The physiotherapist will assess and treat for musculoskeletal impairment that may refer pain to the breast or nipple in the breastfeeding mother. The intent of this case series is to propose extending the differential diagnosis of pain experienced with breastfeeding to musculoskeletal impairment and to provide advice on how to treat it with evidence-based physiotherapy practices used in a nonbreastfeeding clientele.
Footnotes
Acknowledgments
The authors are very grateful to all mothers who participated in this case series. They also acknowledge the contribution of Doreen Killens, Ghislaine Reid, and Kimberley MacKenzie in revising the article. Laura Haiek made substantial contributions in revising it critically for important intellectual content. The preliminary results of this case series were presented at the 2017 Grand Conference of the Association Québécoise des consultantes en lactation diplômées de l'IBLCE (Quebec Association of International Board Certified Lactation Consultants).
Disclosure Statement
No competing financial interests exist.