
Abstract
F
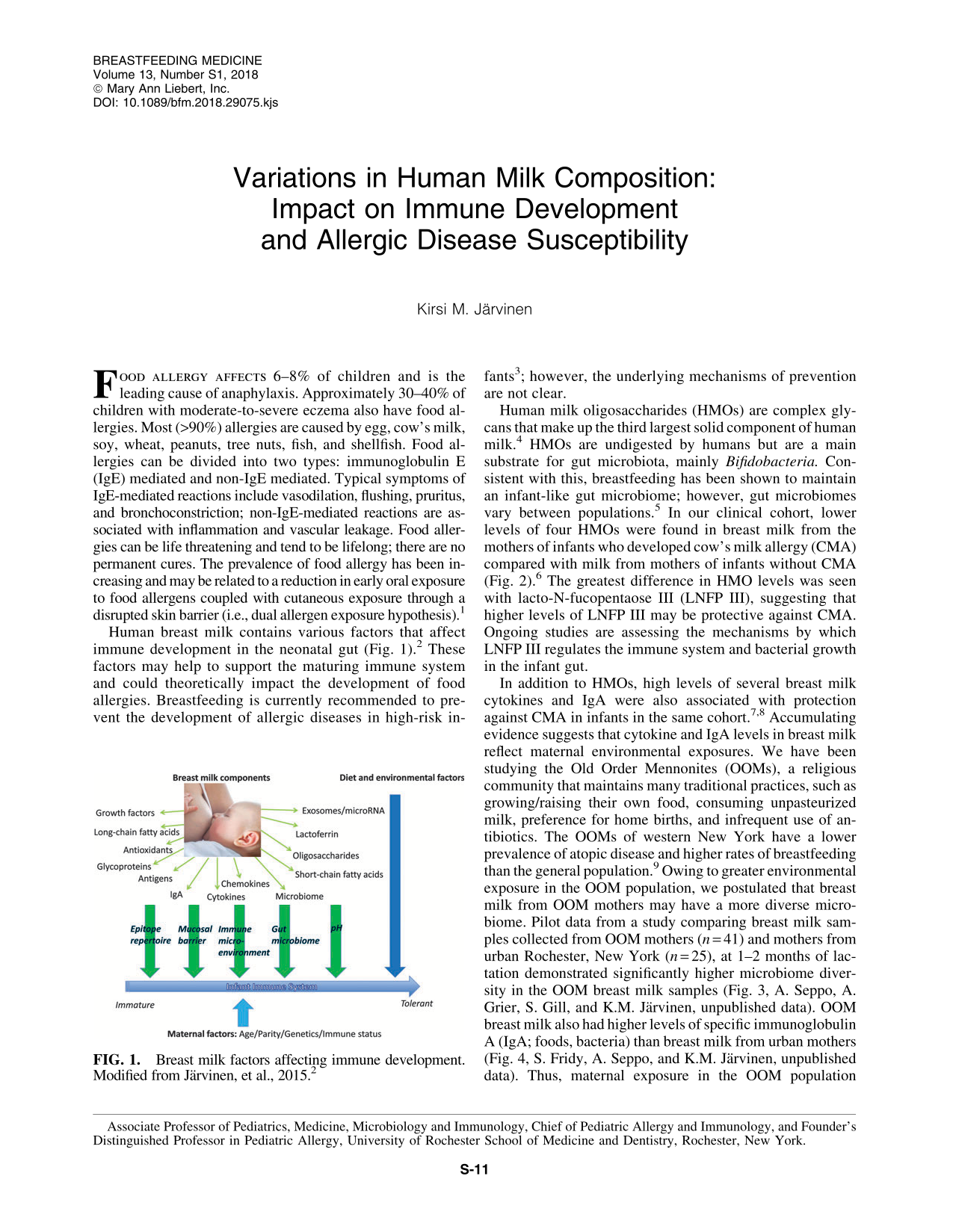
Human breast milk contains various factors that affect immune development in the neonatal gut (Fig. 1). 2 These factors may help to support the maturing immune system and could theoretically impact the development of food allergies. Breastfeeding is currently recommended to prevent the development of allergic diseases in high-risk infants 3 ; however, the underlying mechanisms of prevention are not clear.
Breast milk factors affecting immune development. Modified from Järvinen, et al., 2015. 2
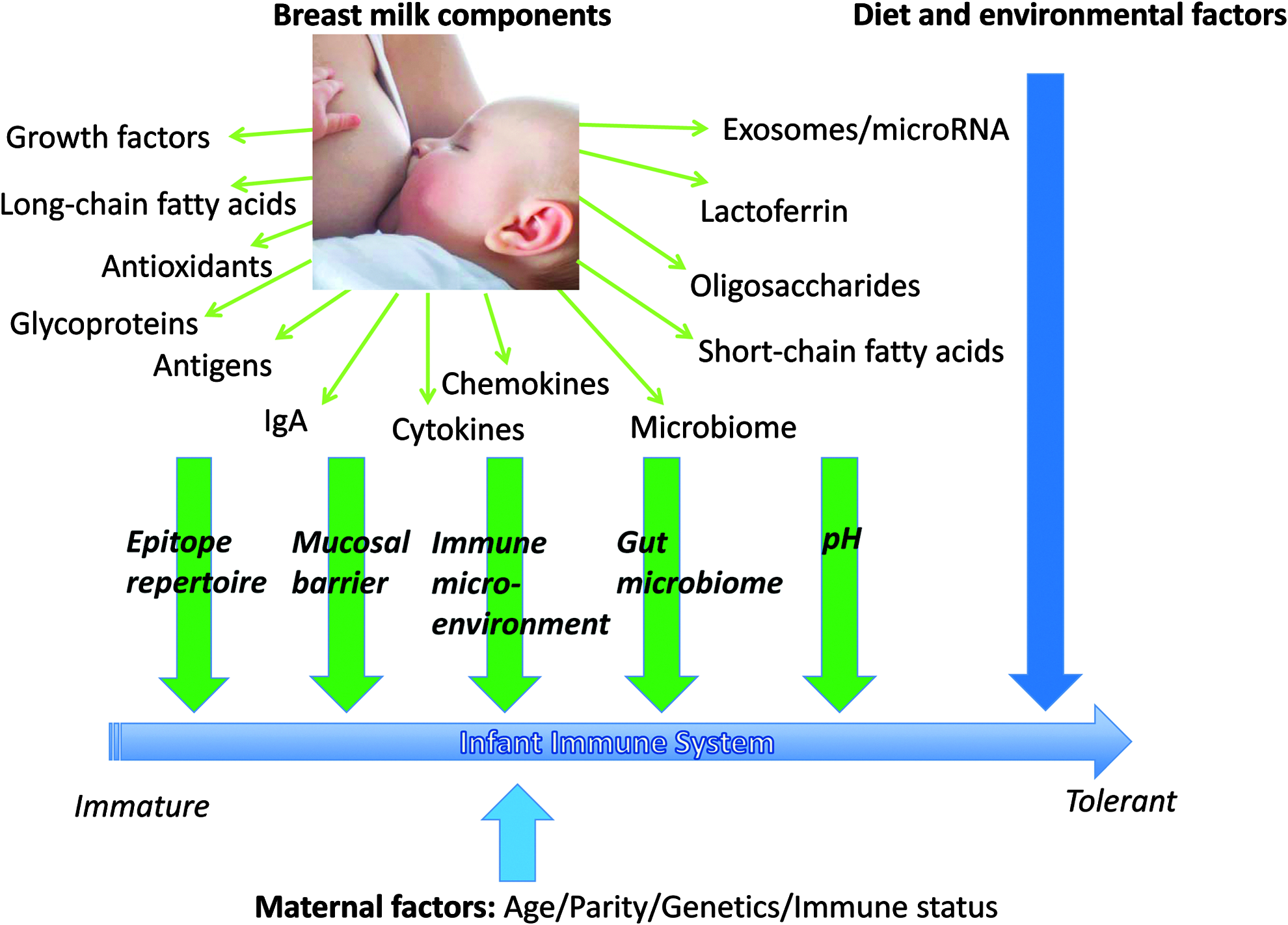
Human milk oligosaccharides (HMOs) are complex glycans that make up the third largest solid component of human milk. 4 HMOs are undigested by humans but are a main substrate for gut microbiota, mainly Bifidobacteria. Consistent with this, breastfeeding has been shown to maintain an infant-like gut microbiome; however, gut microbiomes vary between populations. 5 In our clinical cohort, lower levels of four HMOs were found in breast milk from the mothers of infants who developed cow's milk allergy (CMA) compared with milk from mothers of infants without CMA (Fig. 2). 6 The greatest difference in HMO levels was seen with lacto-N-fucopentaose III (LNFP III), suggesting that higher levels of LNFP III may be protective against CMA. Ongoing studies are assessing the mechanisms by which LNFP III regulates the immune system and bacterial growth in the infant gut.
Possible mechanisms how LNFP III can impact infant immune system development, via its binding to dendritic cells or through its impact on the gut microbiome composition. DC, dendritic cell; IL, interleukin. Courtesy of Javier De Andres Leo.
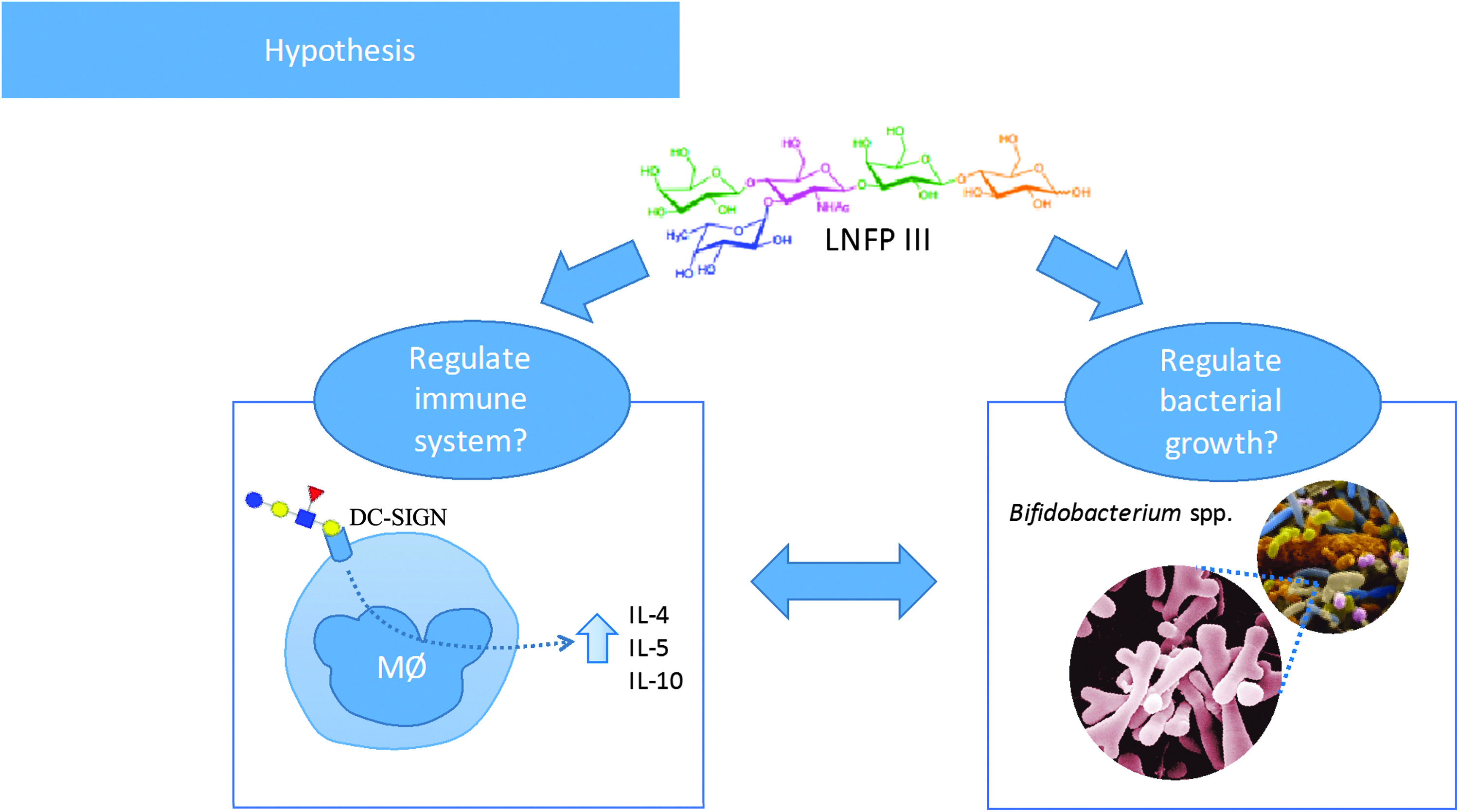
In addition to HMOs, high levels of several breast milk cytokines and IgA were also associated with protection against CMA in infants in the same cohort.7,8 Accumulating evidence suggests that cytokine and IgA levels in breast milk reflect maternal environmental exposures. We have been studying the Old Order Mennonites (OOMs), a religious community that maintains many traditional practices, such as growing/raising their own food, consuming unpasteurized milk, preference for home births, and infrequent use of antibiotics. The OOMs of western New York have a lower prevalence of atopic disease and higher rates of breastfeeding than the general population. 9 Owing to greater environmental exposure in the OOM population, we postulated that breast milk from OOM mothers may have a more diverse microbiome. Pilot data from a study comparing breast milk samples collected from OOM mothers (n = 41) and mothers from urban Rochester, New York (n = 25), at 1–2 months of lactation demonstrated significantly higher microbiome diversity in the OOM breast milk samples (Fig. 3, A. Seppo, A. Grier, S. Gill, and K.M. Järvinen, unpublished data). OOM breast milk also had higher levels of specific immunoglobulin A (IgA; foods, bacteria) than breast milk from urban mothers (Fig. 4, S. Fridy, A. Seppo, and K.M. Järvinen, unpublished data). Thus, maternal exposure in the OOM population results in greater microbial diversity and a more robust mucosal immune response, as reflected in their breast milk, which may impact the development of atopic diseases.
Microbiome diversity in breast milk from OOM and urban mothers. OOM, Old Order Mennonite; PD, phylogenetic diversity; ROC, Rochester, NY.
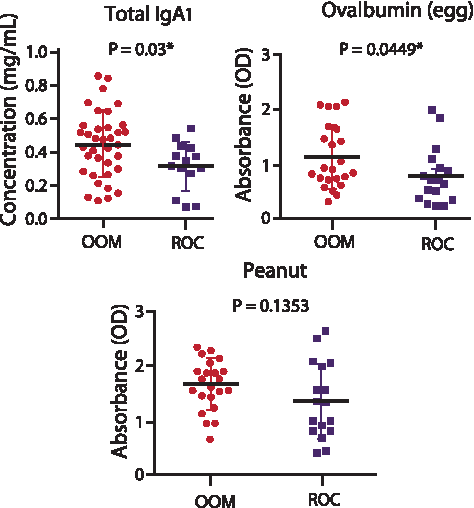
Food-specific lgA levels in breast milk from OOM and urban mothers.
In summary, breast milk is an immunologic support system, the composition of which varies between mothers. Immunomodulatory factors in breast milk (e.g., HMOs, cytokines, and IgA) reflect microbial and antigenic load, as well as host genetics. Together, these factors likely play a role in the development of the infant gut microbiome and immune system, and may provide protection against allergic diseases.